The usability of robotic-assisted systems for total knee arthroplasty can be improved without hindering the accuracy of the bone cuts
Killian Cosendey, Julien Stanovici, Jaad Mahlouly, Patrick Omoumi, Brigitte M. Jolles, Julien Favre

TL;DR
This study shows that improvements in robotic-assisted knee surgery systems don't reduce the accuracy of bone cuts.
Contribution
The study demonstrates that system upgrades for robotic knee surgery maintain accuracy while improving usability.
Findings
RMS values for bone cut errors were mostly below 2 mm or 2°, except for specific tibial positions.
The largest error was in tibial external rotation (3.2°), but errors were consistent with prior system versions.
System upgrades improved usability without compromising accuracy.
Abstract
This study assessed the bone cuts accuracy of a robotic-assisted system for total knee arthroplasty (TKA) that was recently upgraded. Three orthopaedic surgeons planned and executed TKA on 24 sawbones. Bone cut accuracy was assessed using CT scans, comparing the planning and the actual bone cuts in all six degrees-of-freedom. The root-mean-square (RMS) values were below 2 mm or 2° for all error types, except for the medio-lateral position (2.4 mm) and internal-external rotation (2.3°) of the left tibias. The maximal amplitude of the 288 errors (6 degrees-of-freedom * 2 bones * 24 knees) was observed in tibial external rotation (3.2°). Most error types reported a bias, with limited variations among knees. The errors were in the same range as those of the prior version of the system, suggesting that the improvements brought by the system upgrade were not obtained at the expense of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2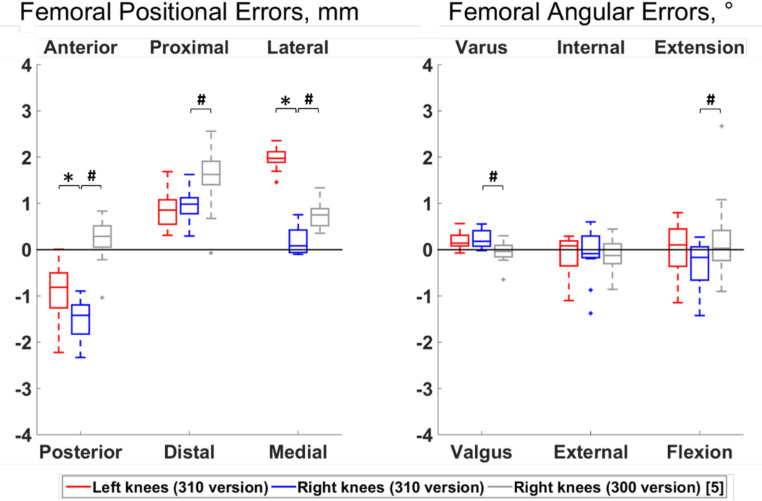 Figure 3
Figure 3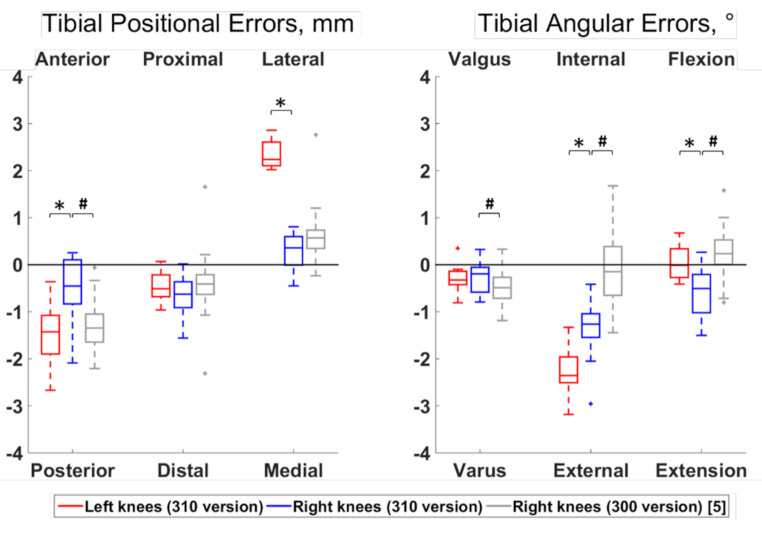 Figure 4
Figure 4- —University of Lausanne
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTotal Knee Arthroplasty Outcomes · Orthopaedic implants and arthroplasty · Orthopedic Infections and Treatments
Introduction
Robotic assistance is increasing in Total Knee Arthroplasty (TKA), particularly because it offers the possibility to improve the accuracy of the bone cuts compared to conventional methods [1–4]. This field is highly dynamic, with regular updates of the robotic tools. To confirm the improvement over time, it is therefore important to keep evaluating the new releases.
Recently, THINK Surgical Inc. (California, USA) released a new version of its TSOLUTION ONE^®^ system (310 vs. 300 previously, Fig. 1), where both the robotic-assisted surgery device that cuts the bone autonomously (310 TCAT^®^) and the planning workstation (310 TPLAN^®^) were upgraded. These upgrades bring a series of improvements, including faster calibration and registration procedures, as well as extended planning possibilities allowing a complete control of the implant placements in all six degrees of freedom. Although appreciable, it is necessary to ensure that these improvements did not lower the accuracy of the cuts that was shown to be appropriate with the 300 version [5]. Furthermore, when assessing the newer version of the system, it would be interesting to test both left and right knees and determine whether the accuracy varies by side. In fact, whereas various aspects could lead to accuracy differences between left and right knees, there is a paucity of data in this regard in literature [6, 7].
Fig. 1. Robotic-assisted surgery device (310 TCAT®, TSOLUTION ONE® Total Knee Application, Think Surgical Inc., Fremont, CA, USA)
The purpose of this study was to assess the bone cuts accuracy of the 310 TSOLUTION ONE system in terms of position and orientation. The study also aimed to determine if the accuracy differs between left and right knees.
Materials and methods
This study used the same methodology and involved the same three orthopaedic surgeons as an earlier work assessing the 300 version [5]. The orthopaedic surgeons were trained on the newer version of the system and each surgeon performed TKA on four right and four left sawbone knees (medium size, solid foam material, Pacific Research Company, Vashon Island, Washington), following the manufacturer’s recommendations. A sample size calculation based on the accuracy of the 300 version [5] indicated that groups of 12 knees were sufficient to detect left-right difference of at least 1 mm or 1° with a significance level of 5% and a power of 80%. The detection threshold was selected conservatively as smaller differences are certainly clinically irrelevant [8].
To assess the accuracy, 10 fiducial markers (metallic beads of 0.8 mm diameter) were embedded in each femur and tibia sawbones. The sawbones were then CT scanned using a Discovery CT750 HD machine (GE Healthcare, Chicago, USA) parametrized as follows: field of view of 250 × 250 mm, matrix size of 512 × 512 pixels, slice thickness of 0.312 mm, tube voltage of 120 kVp and tube current of 200 mAs. The resulting images were uploaded to the planning workstation to reconstruct the 3D bone models, enabling the surgeons to plan the TKA. Then, the sawbones were cut autonomously by the robotic-assisted device (Fig. 2). After the cuts, the sawbones were CT scanned a second time using the same parameters as the initial scan, except for the slice thickness (0.625 mm) and the 3D models of the cut sawbones were reconstructed using in-house software [9]. Then, the model of the original and cut sawbones were imported into Matlab (Mathworks, Natick, MA, USA) and registered using the fiducial markers. Separately, for both the tibia and femur, the registration was performed by identifying the center of the markers and computing the transformation that aligned the markers from the cut sawbone to those on the original sawbone [10]. To quantify the accuracy, reference frames were defined for the femoral and tibial cuts, based on the geometry of the cuts. Using the registered data, these reference frames were aligned to both the planned cuts on the original sawbones and the actual cuts. Finally, for each bone, the differences between the planned and actual reference frames were calculated for the femur and the tibia. The positional accuracy of the cut relative to the planning was measured along the medial-lateral, anterior-posterior and proximal-distal axes. Similarly, the angular accuracy was measured in the sagittal, frontal and transverse planes. All procedures were planned with “Persona Posterior Stabilized” components (Zimmer, Warsaw, Indiana).
Fig. 2. Example of a cut knee
Statistical analysis
Results were reported using median and interquartile range (IQR). The root-mean-square (RMS) errors and the percentage of outlier cuts, meaning cuts with errors exceeding +/- 3 mm or +/- 3° [11], were also reported in agreement with the literature. Wilcoxon rank sum tests were conducted to compare errors in left and right knees, whereas Wilcoxon signed-rank tests were performed to detect errors different from zero, therefore indicating biases in the cut. Comparisons with errors in an earlier study assessing the 300 version of the system on 30 right knees [5] was also performed using Wilcoxon rank sum tests. The significance level was set a priori to 5%.
The reliability of the error measurement method was already assessed in a previous study [5]. Two randomly selected knees were CT-scanned and processed five times each by the same operator. The results demonstrated RMS differences among repeats under 0.2 mm and 0.3° for all positional and angular errors.
Results
Differences between left and right knees were observed for 6 out of the 12 error types (Figs. 3 and 4). Specifically, the right femoral cuts were more posterior and medial compared to the left cuts (median differences of 0.61 mm and 1.89 mm, respectively; p ≤ 0.05), and the right tibial cuts were more anterior, medial, internally rotated and extended compared to the left cuts (median differences of 0.97 mm, 1.88 mm, 1.09° and 0.49°, respectively; p ≤ 0.05).
Fig. 3. Boxplot of the positional and angular errors for the femoral cut. Results from the present study on the newer version of the system (310 TSOLUTION ONE) are plotted in red for the left knees (n = 12) and in blue for the right knees (n = 12). Statistically significant differences among sides are indicted by stars (p < 0.05). For completeness, the errors from a prior work [5] assessing the earlier version of the system (300 TSOLUTION ONE) on right knees (n = 30) are displayed in grey. Statistically significant differences in right knee errors between both versions of the systems are indicated by hashes (p < 0.05). The directions at the top and bottom of the plots indicate where the actual cuts were comparted to the planned cuts. For example, a positive anterior-posterior error indicates a cut that was too anterior compared to the planning
Fig. 4. Boxplot of the positional and angular errors for the tibial cut. Results from the present study on the newer version of the system (310 TSOLUTION ONE) are plotted in red for the left knees (n = 12) and in blue for the right knees (n = 12). Statistically significant differences among sides are indicted by stars (p < 0.05). For completeness, the errors from a prior work [5] assessing the earlier version of the system (300 TSOLUTION ONE) on right knees (n = 30) are displayed in grey. Statistically significant differences in right knee errors between both versions of the systems are indicated by hashes (p < 0.05). The directions at the top and bottom of the plots indicate where the actual cuts were comparted to the planned cuts. For example, a positive anterior-posterior error indicates a cut that was too anterior compared to the planning
The RMS values of all error types were below 2 mm or 2° (Table 1), except for the medio-lateral (2.36 mm) and internal-external (2.34°) errors of the left tibias. In addition, 2 out of the 24 knees had one error qualifying as outliers, both towards tibial external rotation (3.03° and 3.18°).
Table 1. Positional and angular errors of left (n = 12) and right (n = 12) kneesError typeSide ^#^Median {IQR}RMSPercentage of outliersFemur Positional errors, mm Anterior (+) / posterior (-) ^γ^Left knees-0.81 {0.54}*1.090Right knees-1.42 {0.51}*1.590 Proximal (+) / distal (-)All knees0.90 {0.37}*0.990 Lateral (+) / medial (-) ^γ^Left knees1.97 {0.22}*1.990Right knees0.08 {0.46}0.320 Angular errors, ° Varus (+) / Valgus (-)All knees0.17 {0.27}*0.280 Internal (+) / External (-)All knees0.02 {0.43}0.510 Extension (+) / Flexion (-)All knees-0.13 {0.75}0.610Tibia Positional errors, mm Anterior (+) / posterior (-) ^γ^Left knees-1.43 {0.77}*1.60Right knees-0.45 {0.90}0.850 Proximal (+) / distal (-)All knees-0.51 {0.49}*0.690 Lateral (+) / medial (-) ^γ^Left knees2.24 {0.46}*2.360Right knees0.36 {0.53}*0.510 Angular errors, ° Valgus (+) / Varus (-)All knees-0.28 {0.37}*0.400 Internal (+) / External (-) ^γ^Left knees-2.36 {0.51}*2.3417Right knees-1.26 {0.46}*1.510 Flexion (+) / Extension (-) ^γ^Left knees-0.01 {0.49}0.370Right knees-0.51 {0.70}0.780Median, interquartile range (IQR) and root-mean-square (RMS) data are in mm for positional errors and in degree for angular errors^#^: In the absence of statistically significant difference between sides, errors were calculated for left and right knees togetherγ: Statistically significantly different between sides (p ≤ 0.05): Statistically significantly different from zero (p ≤ 0.05)The values in this table indicate where the actual cuts were comparted to the planned cuts
Apart from the flexion-extension and internal-external rotation of the femur, biases were observed with all error types (p ≤ 0.05). The median value of the error types reporting a bias were below 1 mm or 1°, except for the femoral cuts that were too posterior by 1.42 mm in right knees and too lateral by 1.97 mm in left knees and for the tibial cuts that were too posterior by 1.43 mm, lateral by 2.24 mm and externally rotated by 2.36° in left knees and too externally rotated by 1.26° in right knees.
Statistically significant differences between right knees processed with the 300 and 310 versions of the system were observed for 9 out of the 12 error types (Figs. 2 and 3). Specifically, the errors were of smaller amplitudes with the 310 version for the femoral proximal-distal and medio-lateral positions and for the tibial antero-posterior position and varus-valgus (median differences of 0.64 mm, 0.67 mm, 0.89 mm and 0.29°, respectively; p ≤ 0.05). In contrast, the errors had smaller amplitudes with the 300 version for the femoral antero-posterior position, varus-valgus and flexion-extension, as well as for the tibial internal-external rotation and flexion-extension (median differences of 1.71 mm, 0.22°, 0.19°, 1.12° and 0.74°, respectively; p ≤ 0.05).
Discussion
With only 2 out of the 288 errors (24 knees x 12 types of error) classified as outliers and RMS values below 1 mm or 1° for half the error types, the 310 TSOLUTION ONE system showed its capacity to achieve accurate bone cuts. Furthermore, biases were observed, especially in the error types showing the largest RMS values, suggesting that the accuracy could be improved by identifying and annulling the source of systematic deviations. The errors differed between left and right knees and looking more closely at these findings indicated that the side differences were in fact a consequence of different biases in left and right knees. Therefore, reducing the biases would certainly lower the amplitudes and the side differences of the errors at the same time. Further work would be necessary to determine the source of biases and manage them, possibly acting on the calibration or registration procedures. Nevertheless, the biases were relatively small and the impact of such errors on the clinical outcomes remain unknown [12]. Moreover, this study tested a single system once. Therefore, before engaging in any system modification, the variations in errors among systems and over time should probably be characterized. Until this has been done, it is important to consider the errors as indicative of accuracy ranges rather than as definitive values. Consequently, as presented above, a robust manner to summarize the accuracy of the system tested in this study is to report that the bone cut errors rarely exceed 3 mm or 3°, and are often below 2 mm or 2° or even below 1 mm or 1°.
Comparing the errors for the right knees in this study obtained with the 310 version to those from an earlier work on the 300 version [5] indicated globally similar results. Differences were observed, but they were too small and heterogeneous to suggest any compelling difference in the accuracy of the cuts achieved by both versions of the system. Nevertheless, looking at the results of both studies together reinforced the observations that the cuts are consistent from one knee to the other and that the errors are mostly biases.
Compiling data from bone cut accuracy studies of other robotic TKA systems provides valuable context, despite limitations due to methodological differences in robotic systems, sample sizes, knee conditions, and measurement techniques [13–17]. Generally, these systems have shown similar levels of accuracy, with prior studies reporting mean or median femoral bone cut accuracy between 0.1° and 1.1°, consistent with the 0.0° to 0.2° found in this study, and mean or median tibial bone cut accuracy between 0.1° and 0.7°, comparable to the 0.0° to 0.5° observed in the present study, except for tibial internal-external rotation (1.3° for right knees and 2.4° for left knees). This latter parameter is notably underreported in many studies [14–17], indicating a need for further research on this specific metric. Overall, these results highlight the effectiveness of robotic systems in achieving accurate bone cuts for TKA.
The use of sawbones was advantageous for the registration of the cut bones on the preoperative planning as fiducial markers could be embedded in the sawbones. Using sawbones also removed the natural variability among individual human knees, therefore resulting in standardized data that will facilitate systems comparison in the future. However, it is important to acknowledge the limitations associated with the use of sawbones. Unlike real pathological bones, which often present osteophytes, deformities, and varying stiffness, sawbones represent healthy bone structures and lack cortical, cancellous, or sclerotic bone characteristics. This discrepancy raises questions about the model’s ability to accurately reflect patient-specific conditions, potentially limiting the generalizability of the results to clinical settings. Nevertheless, it is important to note that the use of a robotic system in these procedures may mitigate some of the challenges posed by bone deformities. The precision and repeatability of robotic-assisted system could reduce the influence of anatomical irregularities, such as osteophytes or deformities, on the accuracy of the cuts. While these deformities may complicate manual procedures, the robotic system may perform consistently, regardless of such variations.
Given these considerations, future studies should incorporate more clinically representative models, including pathological bones with deformities, to better assess the system’s performance under real surgical conditions. Moreover, considering the preponderant role of biases in the errors and their variations among experimental conditions, further studies are encouraged to diversify the testing conditions, for example by assessing different copies of the system or different implants, in order to improve our understanding of the biases. Additional studies will also be necessary to determine the clinical implication of the biases.
Conclusion
The bone cut errors of the new version of the TSOLUTION ONE system were in the same range as those of its prior version, suggesting that the improvements brought by the 310 version were not obtained at the expense of accuracy. This study also highlighted an important role of biases in the errors. On one hand, this suggested that the accuracy could be improved by reducing the systematic components of the errors. While encouraging, further research is necessary to evaluate the clinical impact of the bone cut errors and therefore the attention that should be paid to them in the future upgrades of the system. On the other hand, the different biases among experimental conditions recommend considering the errors as indicative of accuracy ranges rather than as definitive values.
The reference list from the paper itself. Each links out to its DOI / PubMed record.