Effectiveness of Fatigue-Reducing Interventions in Pediatric Rheumatic Diseases: A Systematic Review
Afra Mohamed Awad Abdu Alla, Ashgan Elfadel Eltyeeb Elnour, Aminat Olayiwola, Ehab Zahran, Rayan Zakria Mohamed Edris, Nazik Abbas Mohammed Ahmmed

TL;DR
This review finds limited evidence for effective fatigue treatments in children with rheumatic diseases, highlighting the need for more research.
Contribution
The study systematically reviews the limited evidence on fatigue-reducing interventions in pediatric rheumatic conditions.
Findings
Aquatic-based physical therapy was more beneficial than land-based exercise therapy for reducing fatigue.
Prednisolone combined with vitamin D significantly reduced subjective fatigue in two placebo-controlled trials.
Creatine supplements did not show benefits in reducing fatigue.
Abstract
There are few intervention trials aimed at lowering fatigue in pediatric rheumatic conditions (PRCs), despite the fact that it is a common and upsetting symptom in these patients. The study's primary goal is to thoroughly examine the data pertaining to the effectiveness of treatments meant to lessen fatigue in PRC patients. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to search for relevant studies across four different databases (PubMed, Web of Science, Scopus, and Google Scholar). A total of 493 records were identified through database searches, and after removing 196 duplicates, 297 unique studies remained for screening. Following title screening and eligibility assessment, 45 studies were excluded for various reasons, and 10 studies met the inclusion criteria for this systematic review. The interventions included exercise…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
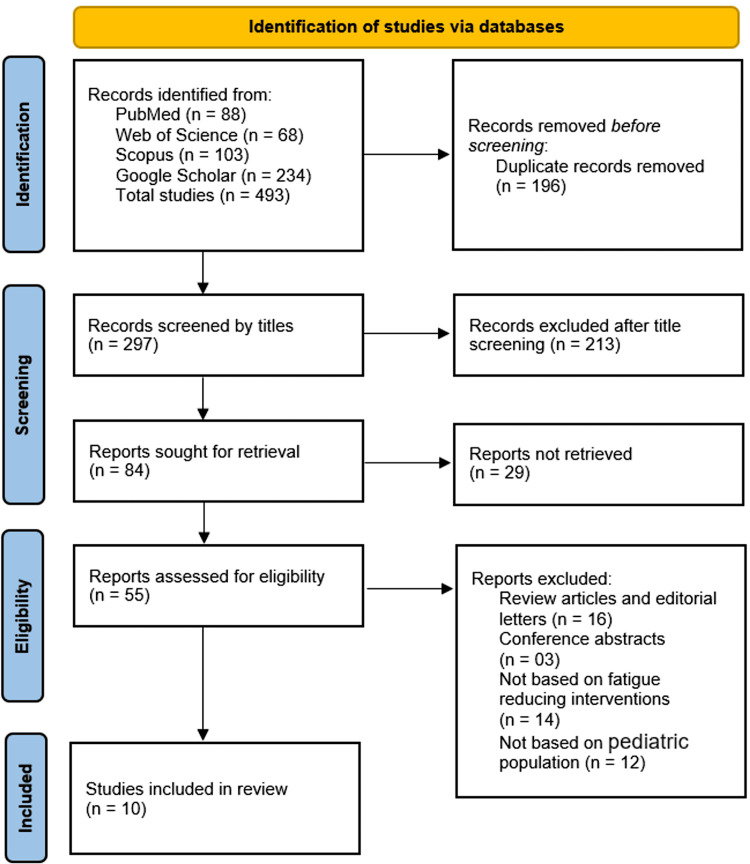 Figure 1
Figure 1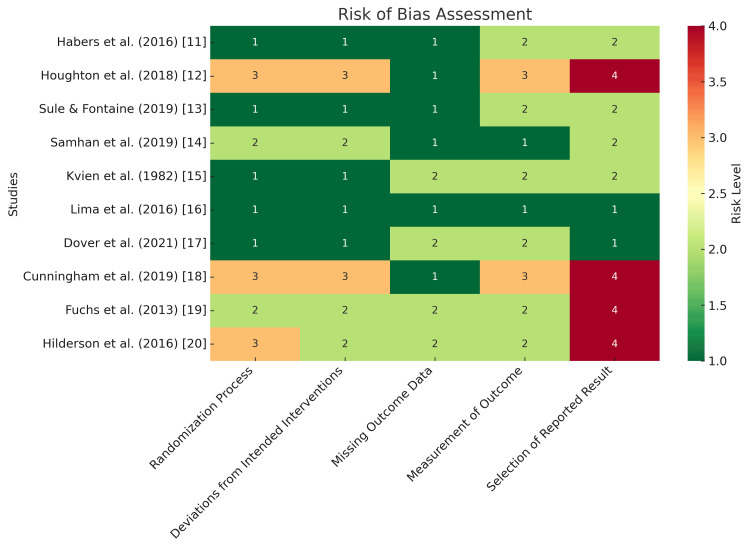 Figure 2
Figure 2| Search Engine | Search Strategy |
| PubMed | ("Fatigue"(MeSH) OR fatigue) AND (pediatric OR children OR adolescents) AND ("Rheumatic Diseases"(MeSH) OR "Juvenile Idiopathic Arthritis" OR "Systemic Lupus Erythematosus") AND (intervention OR therapy OR treatment OR rehabilitation) AND (effectiveness OR outcome). |
| Web of Science | TS=(fatigue AND (pediatric OR children OR adolescents) AND ("rheumatic diseases" OR "juvenile idiopathic arthritis" OR "systemic lupus erythematosus") AND (intervention OR therapy OR treatment) AND (effectiveness OR outcome)). |
| Scopus | TITLE-ABS-KEY(fatigue AND (pediatric OR children OR adolescents) AND ("rheumatic diseases" OR "juvenile idiopathic arthritis" OR "systemic lupus erythematosus") AND (intervention OR treatment OR therapy) AND (effectiveness OR outcome)). |
| Google Scholar | "Fatigue reduction" AND (pediatric OR children OR adolescents) AND ("rheumatic diseases" OR "juvenile idiopathic arthritis" OR "systemic lupus erythematosus") AND (intervention OR therapy OR treatment) AND (effectiveness OR outcome). |
| Author and Publishing Year | Country | Study Design | Sample Size | Participants | Intervention | Controls | Fatigue Measure | Timing of Fatigue Measurement | Results Mean (95% CI) Mean±SD | Key Findings |
| Habers et al., (2016) [ | Netherlands | Multicenter RCT | 26 | Adolescents with JDM | Individually tailored home-based training (resistance & strength exercises) | Usual care | PedsQL-MFS | Immediately post-intervention | Total score follow-up: IG = 75 (71-79), WCG = 74 (69-78) Δ (95% CI): 1 (-5-7) P=0.8 | No statistical difference in fatigue scores |
| Houghton et al., (2018) [ | Canada | Pre-post intervention | 24 | Adolescents with JDM | 6-month home-based program (aerobic & resistance exercises) | No control group | PedsQL-MFS | During & after intervention | Total fatigue scores: Baseline = 57.9 ± 18.2, 3 months = 66.0 ± 18.0, 6 months = 69.9 ± 8.9, 12 months = 67.3 ± 17.2, P = 0.034 | Fatigue decreased, but not statistically significant at 12 months |
| Sule and Fontaine, (2019) [ | United States | Single-center RCT | 33 | Adolescents with JDM | Resistance exercise training (2 sessions/week for 12 weeks) | The control group performed normal activities | K-FSS | After intervention | Baseline: IG = 5.3 ± 0.8, CG = 4.8 ± 1.4; after intervention: IG = ?, CG = ? No statistical differences between IG and CG | No significant difference between groups |
| Samhan et al., (2019) [ | Egypt | Crossover trial | 14 | JDM patients | AGIE + LBE for 4 weeks, followed by LBE alone | AGIE 45 min, 2x per week | PedsQL-MFS | After intervention | Baseline similar in AQBE and LBE: ±35; AQBE improved to 61.9 ± 3.9; LBE improved to 44.2 ± 2.3 | AGIE decreases fatigue |
| Kvien et al., (1982) [ | Norway | Parallel blinded RCT | Not reported | Children with JRA | Prednisolone 0.4 mg/kg for 7 days | Placebo tablets | 10cm fatigue scale | At 7 and 77 days | Mean (ranges): Prednisolone = 0 (-4-4), Placebo = -1 (-6-0), p = 0.03 | Significant reduction in fatigue in the prednisolone group |
| Lima et al., (2016) [ | Brazil | RCT | 40 | Adolescents with SLE | Vitamin D supplementation (50,000 IU/week for 6 months) | Identical placebo tablets | PedsQL-MFS | After intervention | Global score after intervention: VITD = 3.15 ± 1.44, Placebo = 4.30 ± 1.33 | Vitamin D supplementation improves disease activity |
| Dover et al., (2021) [ | Canada | RCT | 13 | Children with JDM | Calcium & vitamin D supplementation | Placebo tablets | PedsQL-MFS | 7 weeks, post-intervention | Mean difference when on creatine compared to placebo = 3.6, P = 0.982 | No effect on fatigue |
| Cunningham et al., (2019) [ | United States | Pre-post intervention | 14 | Adolescents with SLE & JDM | Cognitive-behavioral intervention (TEACH, 6 sessions with caregivers) | No control group | PROMIS fatigue subscale | After intervention | ≤17 years (n = 10): Mean T1 = 20.00, Mean T2 = 14.60, Average decrease = 5.40; ≥18 years (n = 4): Mean T1 = 30.00, Mean T2 = 16.25, Average decrease = 13.75 | Significant improvement in fatigue |
| Fuchs et al., (2013) [ | Netherlands | Controlled trial | 42 | Adolescents with JIA | Self-confrontation psychological intervention | Usual care | CIS-20 | After 11 sessions | No differences in fatigue between the 2 intervention groups | Psychological intervention reduces fatigue |
| Hilderson et al., (2016) [ | Belgium | Quasi-experimental group design | Not reported | Adolescents with JIA | Transition program for transfer to adult rheumatology | Usual care | MFI-20 | After transition | Small positive effects: Reduction in mental fatigue (ES = 0.28), general fatigue (ES = 0.27), and physical fatigue (ES = 0.22); Increased activity (ES = 0.27) and motivation (ES = 0.23) | The transition program reduces fatigue |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune and Inflammatory Disorders Research · Childhood Cancer Survivors' Quality of Life · Pediatric Pain Management Techniques
Introduction and background
Fatigue is one of the most prevalent and debilitating symptoms experienced by children and adolescents with pediatric rheumatic diseases (PRDs), significantly affecting their daily functioning, quality of life, and overall well-being [1]. PRDs, including juvenile idiopathic arthritis (JIA), systemic lupus erythematosus (SLE), juvenile dermatomyositis (JDM), and other inflammatory conditions, are characterized by chronic inflammation, pain, and disability, which contribute to persistent fatigue [2]. Unlike transient tiredness, fatigue in PRDs is often severe, unrelieved by rest, and multifactorial in origin, arising from a combination of disease activity, inflammation, medication side effects, sleep disturbances, and psychosocial factors [3]. However, fatigue is particularly challenging to treat and measure due to its subjective nature, fluctuating intensity, and the lack of standardized assessment tools. Despite its widespread impact, fatigue remains an underrecognized and undertreated symptom in pediatric rheumatology, necessitating a systematic evaluation of interventions aimed at its management [4].
Various interventions have been proposed to reduce fatigue in pediatric patients with PRDs, ranging from pharmacological treatments to non-pharmacological approaches such as physical activity programs, cognitive-behavioral therapy (CBT), sleep hygiene strategies, and dietary modifications [5]. Currently available treatments are limited in number and effectiveness; pharmacological interventions often aim to reduce disease activity, while non-pharmacological approaches focus on improving physical conditioning, mental health, and sleep quality. Pharmacological interventions often include anti-inflammatory or immunosuppressive therapies, which may indirectly alleviate fatigue by controlling disease activity. However, concerns regarding long-term medication use, potential side effects, and variable patient responses highlight the importance of non-pharmacological strategies. Exercise programs, including aerobic training and strength-building exercises, have been shown to improve endurance, reduce pain, and enhance overall energy levels [6]. Similarly, psychological interventions, such as CBT, aim to address maladaptive coping mechanisms, depression, and anxiety, which are frequently associated with fatigue in PRDs. Given the multifactorial nature of fatigue, a multidisciplinary approach incorporating medical, psychological, and lifestyle interventions may offer the most effective management strategy [7].
Despite increasing research on fatigue-reducing interventions in pediatric rheumatology, the effectiveness of various strategies remains uncertain due to heterogeneous study designs, small sample sizes, and variations in outcome measures. This inconsistency further complicates the development of clear treatment protocols and standardized clinical recommendations. Current clinical guidelines provide limited recommendations on fatigue management, emphasizing the need for a comprehensive synthesis of available evidence to inform clinical practice [8]. This systematic review aims to critically evaluate and synthesize the existing literature on the effectiveness of interventions targeting fatigue in pediatric patients with PRDs. By identifying the most effective strategies, highlighting gaps in knowledge, and providing evidence-based recommendations, this review seeks to support healthcare providers in optimizing fatigue management and improving the quality of life for children and adolescents with PRDs.
Review
Methodology
Study Design
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to ensure methodological rigor and transparency [9]. A predefined protocol guided the identification, selection, data extraction, and synthesis of relevant studies examining the effectiveness of fatigue-reducing interventions in PRDs.
Eligibility Criteria
Studies were included if they investigated fatigue-reducing interventions in pediatric patients (aged 18 years or younger) diagnosed with JIA, SLE, JDM, or other inflammatory conditions. Only studies that assessed the effectiveness of interventions using validated fatigue measurement tools and were published in peer-reviewed journals in English were considered. Studies involving adult populations, those without clear fatigue assessment as an outcome, and review articles, case reports, editorials, or conference abstracts without full-text availability were excluded.
Search Strategy
A comprehensive literature search was conducted across PubMed, Web of Science, Scopus, and Google Scholar to identify relevant studies published from inception to the present. The search strategy incorporated Medical Subject Headings (MeSH) terms and free-text keywords related to PRDs, fatigue, and interventions, using Boolean operators to refine search results. The detailed search strategy is provided in Table 1.
Study Selection
All identified records were imported into a reference management software, EndNote X9 (Clarivate Analytics, Philadelphia, Pennsylvania), and duplicates were removed. Two independent reviewers screened the titles and abstracts of identified studies to determine eligibility. Full texts of potentially relevant studies were retrieved and assessed against the inclusion and exclusion criteria. Any disagreements between reviewers were resolved through discussion, with a third reviewer consulted when necessary. A PRISMA flow diagram was used to document the study selection process.
Data Extraction
Data extraction was conducted using a standardized form to ensure consistency and completeness. The extracted data included study characteristics (author, year, country, and study design), participant details (age, gender, disease type, and disease duration), and specifics of the intervention (type, duration, frequency, and intensity). Comparator details were also recorded where applicable. Fatigue outcome measures were collected, including the assessment tools used and reported fatigue levels before and after the intervention. Key findings from each study were systematically documented. Two independent reviewers carried out the data extraction, and any discrepancies were resolved through discussion to maintain accuracy and reliability.
Quality Assessment
The methodological quality and risk of bias of the included studies were assessed using the Cochrane Risk of Bias 2 (RoB 2) tool [10]. Each study was evaluated based on criteria such as randomization process, deviations from the intended intervention, missing outcome data, measurement of the outcome, and selective reporting. The assessment was conducted independently by two reviewers, with disagreements resolved through consensus.
Results
Search Results
A total of 493 records were identified through database searches, including PubMed (n = 88), Web of Science (n = 68), Scopus (n = 103), and Google Scholar (n = 234). After removing 196 duplicate records, 297 unique studies remained for title screening. Following the initial title screening, 213 records were excluded, leaving 84 reports for further assessment. Among these, 29 reports could not be retrieved, reducing the number of studies assessed for eligibility to 55. After a detailed review, 45 studies were excluded for various reasons: 16 were review articles or editorial letters, three were conference abstracts, 14 did not focus on fatigue-reducing interventions, and 12 did not involve a pediatric population. Ultimately, 10 studies met the inclusion criteria and were included in this systematic review (Figure 1).
PRISMA FlowchartPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Characteristics of Included Studies
The systematic review included 10 studies investigating fatigue-reducing interventions in PRDs. These studies were conducted across various countries, including the Netherlands, Canada, the United States, Egypt, Norway, Brazil, and Belgium. The study designs encompassed randomized controlled trials (RCTs), pre-post intervention studies, crossover trials, controlled trials, and quasi-experimental designs. The sample populations primarily consisted of adolescents and children diagnosed with JDM, JIA, JRA, and SLE (Table 2).
Interventions varied across studies and included exercise-based programs such as resistance and aerobic training, aquatic-based exercises, and cognitive-behavioral interventions. Additionally, pharmacological and nutritional interventions, including prednisolone treatment, vitamin D supplementation, and calcium supplementation, were examined. The comparators included usual care, placebo, or no control group, depending on the study design.
Fatigue assessment tools used across studies included the Pediatric Quality of Life Multidimensional Fatigue Scale (PedsQL-MFS) [11,12,14,16,17], Fatigue Severity Scale (K-FSS) [13], 10 cm Fatigue Scale [15], PROMIS (Patient-Reported Outcomes Measurement Information System) Fatigue Subscale [18], Checklist Individual Strength (CIS-20) [19], and Multidimensional Fatigue Inventory (MFI-20) [20]. The timing of outcome assessments varied, with some studies measuring fatigue immediately post-intervention and others conducting follow-ups ranging from weeks to months.
The findings across studies indicated mixed results. Some interventions, such as aquatic-based exercises, CBT, and transition programs, demonstrated significant fatigue reduction, while others, including resistance training and calcium supplementation, did not show statistically significant effects. The overall effectiveness of fatigue-reducing interventions varied depending on the intervention type, duration, and study design.
Results of Risk of Bias Assessment
Among the 10 included studies, five were RCTs, while the remaining studies followed controlled or quasi-experimental designs. The risk of bias was generally low in the randomization process, but increased in areas related to measurement and selective reporting. Studies utilizing subjective fatigue scales showed some concerns in outcome measurement due to potential reporting bias. Additionally, trials without robust blinding methods exhibited a higher risk of bias in deviation from intended interventions. Overall, the assessment highlighted methodological limitations that could impact the reliability of reported fatigue outcomes (Figure 2).
Risk of Bias Assessment of the Included Studies Using the Cochrane Risk of Bias 2 (RoB 2) ToolThe five evaluated domains are represented along the x-axis, while the studies are listed on the y-axis. Color coding indicates the level of bias: green (low risk), yellow (some concerns), orange (moderate risk), and red (high risk). Higher bias levels in measurement and reporting domains suggest potential methodological limitations affecting study reliability.
Discussion
In children and adolescents with PRCs, fatigue is a common unpleasant condition that can significantly affect the patient's and his or her family's engagement in everyday life and general well-being [11-13]. By keeping fatigue from becoming chronic, early and appropriate assessment, treatment, and reduction of its intensity can enhance both their present and future well-being and engagement in day-to-day activities [18].
Although fatigue has a significant impact and long-term effects on patients with PRC, there are currently few available treatment alternatives [19]. Although the data syntheses show insufficient evidence to support the effectiveness of current interventions to reduce the extent of fatigue in PRCs, the remarkably small number of studies with regard to the effectiveness of interventions aimed at minimizing fatigue among individuals with PRCs suggested a minor yet important impact in the individual studies [11,18]. Fatigue was not the main outcome in the majority of the trials, and none of them reported that the research group was well-controlled with generally low disease activity or adjusted for illness activity. The inconclusive results of the included studies, the risk of bias, variation in diagnostic groups, ages and disease phases, the heterogeneity in the variety of interventions, and the small number of studies all combine to offer a general assessment of the effectiveness of the used interventions, particularly with regard to the potential superiority of one form of therapy [21]. Our findings highlight the need for more multifaceted intervention research primarily focused on treating fatigue in adolescents and children with PRCs, as well as the need for greater understanding of how to measure fatigue in this patient population precisely and consistently throughout treatment and follow-up [22].
The most promising therapeutic modalities for lowering fatigue in individuals with rheumatoid arthritis are physical and psychological therapy [13]. Based on a systematic review of six studies (388 participants) examining physical therapy (such as yoga, strength training, aerobics, and pool-based therapy) and 13 studies (1579 participants) examining psychological approaches (such as self-management, CBT, mindfulness, and group education), Kim et al. [23] concluded that both psychological interventions and physical activity had a marginally significant impact on reducing fatigue in adults with RA. Hewlett et al. [24] recently reported that group CBT had a positive influence on lowering the impact of fatigue in rheumatoid arthritis patients when compared to just obtaining fatigue information. Although further research is necessary, CBT may potentially be useful for people with PRCs.
Similar to this study, all of the previously stated reviews note that the studies that were included had heterogeneous interventions, small sample numbers, and varying outcome measures and intervention protocols, which means they do not produce definitive proof [25,26].
This review's strength is its emphasis on strategies to address fatigue in PRC patients. However, the data presented by the studies that satisfied the inclusion criteria did not allow for meta-analysis. Few, varied, and inconclusive studies constitute the small number of included studies. Moreover, stratified assessment was not feasible due to the small number of papers available for synthesis and the significant variety in intervention techniques, study designs, and outcome-measuring tools among the individual research. As a result, it is impossible to offer suggestions for incorporating successful interventions into children with PRCs' everyday routines [27].
In addition to being a medical (side) effect of PRCs and their treatment, fatigue is most likely the complicated outcome of the psychological and physical difficulties associated with having a chronic illness growing up [16]. Thus, it may be necessary to look for a multifaceted cause and a dynamic interaction between the body and mind to find the solution. All of the demonstrated therapies targeted distinct (single) potential reasons why adolescents and children with various PRC types might feel exhausted [17]. The conceptual model of fatigue in JIA put forth by Kim et al. [23] shows that fatigue appears to be multifactorial and ought to be handled as such. The model depicts a potential interaction between "personal," "disease-related," "environmental," and "generic" elements that may be involved in the development and persistence of fatigue in PRCs. As a result, we recommend that treatments, including CBT, address both the psychological and physical components of weariness [17]. It has been demonstrated that CBT helps fatigued adults with a variety of chronic illnesses, including RA, as well as adolescents with chronic fatigue disorders [14]. Additional promising therapies include calm, healing touch, exercise, and education. Through lowering inflammation, boosting muscular growth or strength, and enhancing mental and functional abilities, physical activity may help reduce weariness.
Limitations
This review is subject to several limitations. The small number of included studies (n=10) and the heterogeneity of the interventions (e.g., CBT, physical therapy), outcome measures, and patient populations (e.g., varying diagnoses and age groups) prevented the conduct of a meta-analysis and stratified assessments, as discussed. Additionally, most studies had methodological flaws, including a high risk of bias in randomization and attrition (Figure 2), and fatigue was often assessed as a secondary outcome, which resulted in underpowered analyses. The use of inconsistent fatigue measurement tools, the absence of long-term follow-up (e.g., Lima et al. [16]), and the potential for publication bias further limit the strength of the conclusions. While these limitations reflect the early stage of fatigue intervention research in PRDs, as discussed, they emphasize the urgent need for larger, well-designed, and standardized trials that prioritize fatigue as a primary endpoint.
Conclusions
More intervention studies focusing only on treating fatigue in adolescents and children with PRCs are desperately needed. Potential underlying biological and psychological pathways must be identified as potential therapy targets to lessen fatigue symptoms in kids and teenagers with PRCs. Future research should look into interventions that use a multifaceted approach to fatigue. This means that they should focus on the psychological and physical aspects of fatigue in addition to an evaluation that determines how fatigue relates to environmental, personal, and physical outcome parameters.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical features and disease course of patients with juvenile dermatomyositis Int J Rheum Dis Gowdie PJ Allen RC Kornberg AJ Akikusa JD 5615671620132416484410.1111/1756-185X.12107 · doi ↗ · pubmed ↗
- 2Fatigue in patients with juvenile idiopathic arthritis: a systematic review of the literature Semin Arthritis Rheum Armbrust W Siers NE Lelieveld OT Mouton LJ Tuinstra J Sauer P 5875954520162665603110.1016/j.semarthrit.2015.10.008 · doi ↗ · pubmed ↗
- 3Making the diagnosis of systemic lupus erythematosus in children and adolescents Lupus Tucker LB 5465491620071771188610.1177/0961203307078068 · doi ↗ · pubmed ↗
- 4Prevalence of severe fatigue among adolescents with pediatric rheumatic diseases Arthritis Care Res (Hoboken) Nijhof LN van de Putte EM Wulffraat NM Nijhof SL 1081146820162631439010.1002/acr.22710 · doi ↗ · pubmed ↗
- 5Physical activity for paediatric rheumatic diseases: standing up against old paradigms Nat Rev Rheumatol Gualano B Bonfa E Pereira RM Silva CA 3683791320172853355210.1038/nrrheum.2017.75 · doi ↗ · pubmed ↗
- 6Fatigue in childhood chronic disease Arch Dis Child Nap-van der Vlist MM Dalmeijer GW Grootenhuis MA 1090109510420193117512410.1136/archdischild-2019-316782 · doi ↗ · pubmed ↗
- 7Is fatigue a disease-specific or generic symptom in chronic medical conditions?Health Psychol Menting J Tack CJ Bleijenberg G 5305433720182978165410.1037/hea 0000598 · doi ↗ · pubmed ↗
- 82019 American College of Rheumatology/Arthritis Foundation guideline for the treatment of juvenile idiopathic arthritis: therapeutic approaches for non-systemic polyarthritis, sacroiliitis, and enthesitis Arthritis Care Res (Hoboken) Ringold S Angeles-Han ST Beukelman T 7177347120193102151610.1002/acr.23870 PMC 6561125 · doi ↗ · pubmed ↗