A Community-Based Cross-Sectional Study to Assess the Prevalence of Undiagnosed Diabetes Mellitus in Vijayapura City
Sanketh C M, Vijaykumar G Warad, Anuja M Kadagud, Rahul Biradar

TL;DR
This study found that 5.61% of people aged 35 and above in Vijayapura, India, had undiagnosed diabetes, highlighting the need for better screening and education.
Contribution
The study provides a novel prevalence estimate of undiagnosed diabetes in an urban Indian population aged 35 and above.
Findings
A 5.61% prevalence of undiagnosed diabetes was identified in Vijayapura's urban population.
67 new diabetes cases were detected among 1195 screened participants.
The findings emphasize the need for targeted public health interventions.
Abstract
Background Undiagnosed diabetes mellitus (UDM), a chronic hyperglycemic disorder, presents a growing global health challenge with significant morbidity and mortality risks stemming from delayed diagnosis and subsequent complications. Limited awareness, slow disease progression, and healthcare system limitations contribute to a substantial proportion of UDM, particularly in India, where the high economic burden of managing diabetes complications underscores the need for accurate UDM estimation to inform effective public health policies. Objective The primary objective of this community-based cross-sectional epidemiological study was to ascertain the prevalence of UDM within the urban populace aged 35 years and above in Vijayapura, Karnataka, India. Methods Conducted from May 2023 to December 2024 in urban Vijayapura, a sample of 1195 participants, stratified equally across six…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
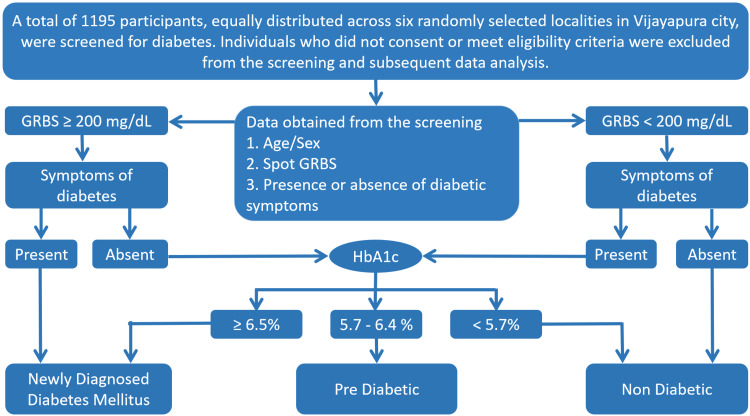 Figure 1
Figure 1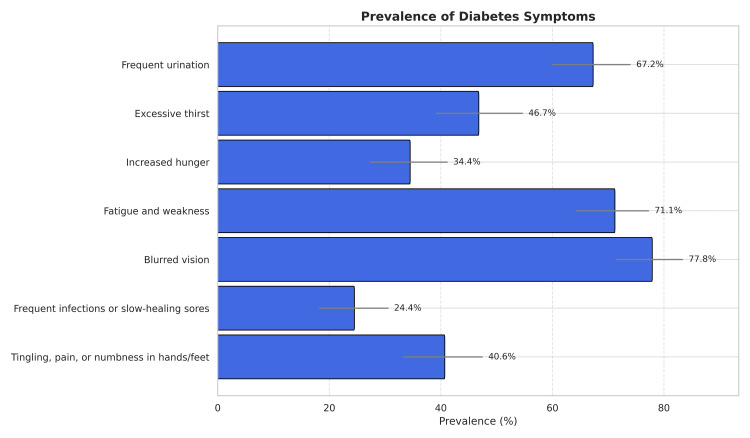 Figure 2
Figure 2| RBS (mg/dL) | Symptoms of diabetes | HbA1c (%) | Inference |
| ≥ 200 | Present | - | UDM |
| Absent | ≥ 6.5 | UDM | |
| 6.4-5.7 | Pre-diabetic | ||
| < 5.7 | Non-diabetic | ||
| < 200 | Absent | - | Non-diabetic |
| Present | ≥ 6.5 | UDM | |
| 6.4-5.7 | Pre-diabetic | ||
| < 5.7 | Non-diabetic |
| Category | N | Prevalence % | 95% CI |
| UDM | 67 | 5.61% | (4.3%, 6.9%) |
| Pre-diabetic | 24 | 2.01% | (1.2%, 2.8%) |
| Non-diabetics | 1104 | 92.38% | (91%, 94%) |
| Total participants screened | 1195 | ||
| Gender | Participants screened | UDM | Prevalence % | 95% CI |
| Female | 599 | 35 | 2.93% | (2%, 3.9%) |
| Male | 596 | 32 | 2.68% | (1.8%, 3.6%) |
| Total | 1195 | 67 | 5.61% | (4.3%, 6.9%) |
| Age group | Participants screened (N) | UDM (n) | Prevalence % | 95% CI |
| 35-44 years | 202 | 5 | 2.48% | (0.8%, 5.7%) |
| 45-54 years | 287 | 11 | 3.83% | (1.9%, 6.9%) |
| 55-64 years | 287 | 20 | 6.97% | (4.3%, 10.4%) |
| 65-74 years | 239 | 17 | 7.11% | (4.3%, 11.2%) |
| 75-85 years | 120 | 11 | 9.17% | (4.6%, 16.3%) |
| >85 years | 60 | 3 | 5.00% | (1.0%, 14.0%) |
| Symptoms of diabetes | N | Prevalence % | 95% CI |
| Frequent urination | 121 | 67.2% | (60%, 74%) |
| Excessive thirst | 84 | 46.7% | (39.1%, 54.7%) |
| Increased hunger | 62 | 34.4% | (27.3%, 41.2%) |
| Fatigue and weakness | 128 | 71.1% | (64.1%, 77.3%) |
| Blurred vision | 140 | 77.8% | (71.3%, 83.4%) |
| Frequent infections or slow-healing sores | 44 | 24.4% | (18.1%, 30.6%) |
| Tingling, pain, or numbness in hands/feet | 73 | 40.6% | (33.2%, 47.5%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes, Cardiovascular Risks, and Lipoproteins · Diabetes Management and Research · Diabetes Management and Education
Introduction
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by hyperglycemia resulting from absolute or relative deficiencies in insulin secretion and/or action. The global prevalence of diabetes in adults over 18 years of age rose from 180 million (4.7%) to 451 million (8.8%) between 1980 and 2017 [1-3]. DM was the direct cause of 4.0 million deaths in 2015, with half of them occurring in individuals under the age of 70 [1]. The World Health Organization (WHO) projects DM to be the seventh leading cause of mortality by 2030. Global estimates suggest that approximately 628.6 million individuals will be living with diabetes by the year 2045 [4].
Delayed diagnosis of DM is frequently a consequence of limitations within healthcare systems, inadequate public and professional awareness regarding the condition, and the often insidious onset or gradual progression of the disease. This protracted period of undiagnosed diabetes mellitus (UDM) exposes individuals to sustained hyperglycemia, leading to the development of significant and irreversible micro-vascular (peripheral vascular disease, neuropathy, nephropathy, retinopathy) and macro-vascular (coronary artery disease, stroke) sequelae [5,6]. UDM is associated with a significantly elevated mortality risk, ranging from 1.5 to 3.0 times that of individuals with normoglycemia. Notably, the mortality risk associated with UDM has been observed to be comparable to that of individuals with diagnosed DM [7,8].
The prevalence of DM is rising at a higher rate in low and lower-middle-income countries. According to International Diabetes Federation (IDF) global estimates of the prevalence of diabetes for 2011 and 2030, the greatest increase is expected in low-income countries (92%), followed by lower-middle-income countries like India (57%), upper-middle-income countries (46%), and finally, higher-income countries (25%) [9]. There are 77 million diabetics in India, and 43.9 million (57%) of them remain undiagnosed [10]. According to the India state-level disease burden initiative diabetes study collaborators, India's diabetes cases rose from 26 million in 1990 to 65 million in 2016, with adult prevalence increasing from 5.5% to 7.7%. State-level prevalence was highest in Tamil Nadu, followed by Karnataka, Kerala, Delhi, Punjab, and Goa [11].
Diabetes-related medical expenses have a significant financial impact on people, health systems, and governments in addition to the health burden; in 2013, it was projected that global health expenditures totaled at least 548.5 billion USD [12]. This estimate may be significantly impacted by the expense of UDM. The expense of diagnosing and treating DM is high, but it is greatly surpassed by the expense of treating complications from diabetes that may be avoided [12,13]. To comprehend the global and regional burden of UDM, its causes, and possible ramifications for practice and policy, it is critical to generate regional and global estimations of UDM.
Primary prevention of DM begins with targeted screening to identify high-risk individuals, including those with asymptomatic and undiagnosed disease. However, disparities in the availability and accessibility of diagnostic testing for diabetes contribute to its underdiagnosis. Therefore, this community-based cross-sectional study was conducted in urban Vijayapura, Karnataka, India, to assess the prevalence of UDM among adults aged 35 years and above and to highlight the need for enhanced screening strategies in this population.
Materials and methods
Study design
This community-based cross-sectional study assessed the prevalence of UDM in individuals aged 35 years and above residing in urban Vijayapura between May 2023 and December 2024. Ethical approval was obtained from Shri B. M. Patil Medical College Hospital and Research Centre, Bijapur Lingayat District Education (BLDE) (Deemed to be University), and all participants provided written informed consent.
Study participants
The inclusion criteria were as follows: individuals residing in Vijayapura, aged 35 years or older, with no prior diagnosis of diabetes. Exclusion criteria included pregnant or lactating women and individuals taking medications known to induce hyperglycemia (e.g., corticosteroids).
Sampling method and data collection
A multi-stage sampling method was used. Six wards were randomly selected from Vijayapura's administrative units. Within each ward, households were systematically approached, and all eligible individuals were invited to participate, with up to two repeat visits for non-responders. A total of 1195 participants were screened, ensuring proportional representation across the selected wards.
Data collected included age, sex, random blood sugar (RBS) levels (using a regularly calibrated Accu-Chek Active Glucometer, Roche Diagnostics, Mannheim, Germany), and self-reported symptoms of hyperglycemia and diabetes (blurred vision, fatigue, frequent urination, excessive thirst, tingling/numbness, increased hunger, slow-healing sores/infections).
Data interpretation
Data interpretation followed the American Diabetes Association (ADA) guidelines [14]. Symptomatic individuals with RBS ≥ 200 mg/dL were classified as UDM. Asymptomatic individuals with RBS < 200 mg/dL were classified as non-diabetic initially. Symptomatic individuals with RBS < 200 mg/dL and asymptomatic individuals with RBS ≥ 200 mg/dL underwent HbA1c testing (at Central Research Laboratory, Shri B. M. Patil Medical College Hospital and Research Centre, BLDE (Deemed to be University) using high-performance liquid chromatography (HPLC)). Participants were categorized as UDM (HbA1c > 6.5%), pre-diabetic (HbA1c 5.7-6.4%), or non-diabetic (HbA1c < 5.7%) (Table 1 and Figure 1).
Flowchart representing methodology and data collection
Sample size
Based on a previous study indicating a 7.6% diabetes prevalence [15], a sample size was determined to estimate the prevalence of UDM in the urban population aged 35 years and above in Vijayapura with a 95% confidence level and a precision of 1.65%. A target sample size of 1195 participants was set to ensure adequate statistical power and account for potential non-response and ineligibility.
Statistical analysis
Data were entered in Microsoft Excel (Microsoft® Corp., Redmond, WA) and analyzed using SPSS (IBM SPSS Statistics for Windows, IBM Corp., Version 20, Armonk, NY). Descriptive statistics summarized participant characteristics and UDM prevalence. Group differences were assessed using t-tests (for normally distributed continuous data), Mann-Whitney U tests (for non-normal continuous data), and chi-square or Fisher's exact tests (for categorical data). ANOVA or Kruskal-Wallis H tests were used to compare more than two groups. A 95% confidence interval was used for all two-tailed statistical tests.
Results
We screened 1195 participants aged 35 years and above from six randomly selected geographical areas in Vijayapura for UDM. Initial screening based on symptomatic presentation and an RBS level ≥ 200 mg/dL identified 60 participants with UDM. Subsequently, 120 additional symptomatic participants with RBS levels < 200 mg/dL underwent hemoglobin A1c (HbA1c) testing, revealing seven further cases of UDM and 24 individuals with pre-diabetes. Consequently, the overall study results showed 67 participants (5.61%) had UDM, 24 (2.01%) were pre-diabetic, and 1104 (92.38%) were non-diabetic (Table 2).
Among the 1195 participants screened for diabetes (599 females and 596 males), 35 females and 32 males had UDM. The gender-specific prevalence of UDM was slightly higher in females (2.93%; 95% CI: 2%, 3.9%) than in males (2.68%; 95% CI: 1.8%, 3.6%) (Table 3).
The age-specific prevalence of UDM is stratified into six age groups: 35-44, 45-54, 55-64, 65-74, 75-85, and >85 years, and the number of participants screened varied across age groups (Table 4). The 45-54 year and 55-64 year age groups had the largest sample sizes (n = 287 each), and the >85 years age group the smallest (n = 60). The prevalence of UDM increased with age, reaching a peak of 6.97% (20 cases out of 287) in the 55-64 year age group, followed by a decline in older age groups, reaching 5% (three cases out of 60) in the >85 year age group. However, the decline in prevalence in the older age groups suggests a non-linear relationship across the entire age spectrum (Table 4).
Among 1195 participants screened, 180 (15.1%) reported having one or more symptoms of diabetes. The most common symptoms were blurred vision (77.8%, 95% CI: 71.3%, 83.4%), fatigue and weakness (71.1%, 95% CI: 64.1%, 77.3%), and frequent urination (67.2%, 95% CI: 60%, 74%). Other frequently reported symptoms included excessive thirst (46.7%, 95% CI: 39.1%, 54.7%), tingling, pain, or numbness in hands/feet (40.6%, 95% CI: 33.2%, 47.5%), and increased hunger (34.4%, 95% CI: 27.3%, 41.2%). Frequent infections or slow-healing sores were observed in 24.4% (95% CI: 18.1%, 30.6%) of individuals (Table 5 and Figure 2).
Distribution of symptoms of diabetes mellitus
Discussion
The high rate of UDM in Vijayapura is a serious concern, particularly because a significant portion of these individuals presented with diabetic symptoms, yet remained unaware of their condition, likely due to limited knowledge about the disease. These findings are consistent with previous studies conducted in India and other countries.
For instance, a study by Pradeepa and Mohan estimated that 57% of adults with diabetes in India remain undiagnosed, corresponding to approximately 43.9 million individuals. The authors emphasized that many individuals are unaware of their diabetic status due to a lack of screening and asymptomatic progression in early stages [10]. International studies have also reported a high prevalence of UDM. A study in Northwest Ethiopia found a UDM prevalence of 10.2%, with risk factors including a lack of knowledge of symptoms of diabetes and family history [16]. This is higher than the 5.61% prevalence observed in the current study, likely due to differences in lifestyle, genetic predisposition, and access to healthcare.
In contrast, the national diabetes statistics report of the United States reported a 3.4% prevalence rate of UDM in the country [17]. Similarly, a study in China also reported a lower prevalence of UDM (4.4%) [18]. This lower prevalence is likely due to widespread access to healthcare services and early detection programs in these countries.
Our study showed that UDM prevalence in urban Vijayapura followed a non-linear trend with age, increasing to a peak in middle age and then decreasing in both younger and older age groups, with the highest proportion of UDM observed in the 55-64 year age group, followed by the 65-74 year age group. These findings align with previous studies indicating that diabetes prevalence increases with age. For instance, the National Non-communicable Disease Monitoring Survey conducted in India between 2017 and 2018 found that diabetes prevalence sharply rises after 30-49 years of age, with individuals aged 50-69 years having the highest burden of diabetes in India [19].
However, in contrast to our study, Sahadevan et al.'s analysis of National Family Health Survey (NFHS)-5 (2019-2021) data in individuals under 50 years yielded a 1.22% prevalence of UDM. This disparity is likely explained by the substantial age difference between their younger population and our older cohort [20].
Our study's results align with the community-based cross-sectional study conducted in Bahir Dar city of northwest Ethiopia, which found the highest prevalence of UDM in the 55-64 age group, at 21.9% [16]. On the other hand, in China, a national diabetes screening program identified a more even age distribution across younger and older adults, suggesting that earlier detection strategies may help mitigate age-related diabetes progression [21].
The results of our study underscore the urgent need for the adoption of widespread diabetes screening and comprehensive public awareness and health education strategies in India, particularly targeting both urban and rural regions with limited healthcare resources. Given the increasing burden of DM in India, the successful implementation of these interventions, alongside improved healthcare accessibility, is critical for decreasing the prevalence of UDM.
This study possesses notable strengths in its methodology, employing a large, representative sample achieved through stratified random sampling and community-based screening. The implementation of symptom-driven HbA1c follow-up for symptomatic individuals exhibiting normal RBS values enhanced the precision of diabetes detection by minimizing false negatives. Nevertheless, several limitations warrant consideration. The exclusion of participants under 35 years of age, the reliance on symptom-based HbA1c testing, and the absence of fasting blood sugar (FBS) screening suggest that the estimated prevalence of UDM within Vijayapura may not fully reflect the true prevalence. These limitations, arising from pragmatic considerations of cost and participant compliance, potentially resulted in reduced sensitivity for identifying UDM cases, a possible underestimation of overall prevalence, particularly concerning asymptomatic presentations, and a likely under-representation of type 1 diabetes within the study population.
Conclusions
Our study reveals a substantial prevalence of UDM among individuals aged 35 years and above in Vijayapura. The persistence of UDM, even in participants with overt symptoms, highlights a critical knowledge deficit. Middle age represents a period of peak prevalence, underscoring the necessity for early detection through targeted community screening and public health education to mitigate diabetes-related morbidity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045 Diabetes Res Clin Pract Cho NH Shaw JE Karuranga S Huang Y da Rocha Fernandes JD Ohlrogge AW Malanda B 27128113820182949650710.1016/j.diabres.2018.02.023 · doi ↗ · pubmed ↗
- 2WHO global report on diabetes: a summary Int J Noncommunicable Dis Gojka R 3812016
- 3Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants Lancet Zhou B Lu Y Hajifathalian K 1513153038720162706167710.1016/S 0140-6736(16)00618-8PMC 5081106 · doi ↗ · pubmed ↗
- 4Projections of global mortality and burden of disease from 2002 to 2030 P Lo S Med Mathers CD Loncar D 03200610.1371/journal.pmed.0030442 PMC 166460117132052 · doi ↗ · pubmed ↗
- 5Microvascular and macrovascular complications of diabetes Clin Diabetes Fowler MJ 116122292011
- 6Diabetes and macrovascular disease J Diabetes Complicat Vinik A Flemmer M 23524516200210.1016/s 1056-8727(01)00212-412015194 · doi ↗ · pubmed ↗
- 7Criteria for previously undiagnosed diabetes and risk of mortality: 15-year follow-up of the Edinburgh Artery Study cohort Diabet Med Wild SH Smith FB Lee AJ Fowkes FG 4904962220051578767810.1111/j.1464-5491.2004.01433.x · doi ↗ · pubmed ↗
- 8Mortality risk in Spanish adults with diagnosed diabetes, undiagnosed diabetes or pre-diabetes. The Asturias study 1998-2004 Rev Esp Cardiol Valdés S Botas P Delgado E Díaz Cadórniga F 5285346200910.1016/s 1885-5857(09)71835-319406067 · doi ↗ · pubmed ↗