Case Report: Moderate-to-severe paravalvular leak regurgitation after recurrent prosthetic valve endocarditis in a patient with a double-chambered right ventricle associated with a restricted membranous ventricular septal defect
Cosimo Sacra, Antonio Totaro, Giuseppe Triggiani, Andrea Romano, Pasquale Astore, Chiara Galluccio, Eustaquio Maria Onorato

TL;DR
A patient with multiple heart valve surgeries and a rare heart defect successfully had a leak repaired using a less invasive catheter procedure.
Contribution
Demonstrates the feasibility of transcatheter closure for paravalvular leak in patients with complex cardiac histories and multiple prior surgeries.
Findings
Transcatheter PVL closure was successfully performed in a high-risk patient with multiple prior aortic valve replacements.
Advanced imaging and a multidisciplinary approach ensured precise device placement and effective leak closure.
Post-procedural imaging showed trace-mild residual leak, indicating a successful outcome.
Abstract
Managing aortic paravalvular leak (PVL) regurgitation following multiple surgical aortic valve replacements (SAVRs) due to recurrent infective endocarditis (IE) presents significant clinical challenges. A 46-year-old woman with a history of severe aortic regurgitation and an asymptomatic membranous ventricular septal defect underwent SAVR with a bioprosthetic aortic valve (Perimount 23 mm) in 2005. Concomitantly, a double-chambered right ventricle was diagnosed. Ten years later, due to recurrent IE, another bioprosthetic valve replaced the previous valve (Magna Ease #25). In 2018, she developed sepsis from Bordetella hinzii endocarditis, leading to a third SAVR in 2019, this time with a mechanical aortic valve (On-X® #23). In 2024, two-dimensional transesophageal echocardiography (TEE) revealed moderate-to-severe PVL regurgitation near the right coronary cusp. After a multidisciplinary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
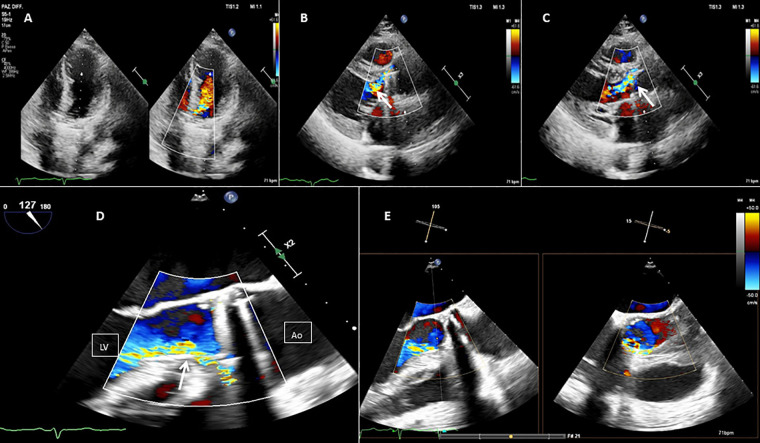 Figure 1
Figure 1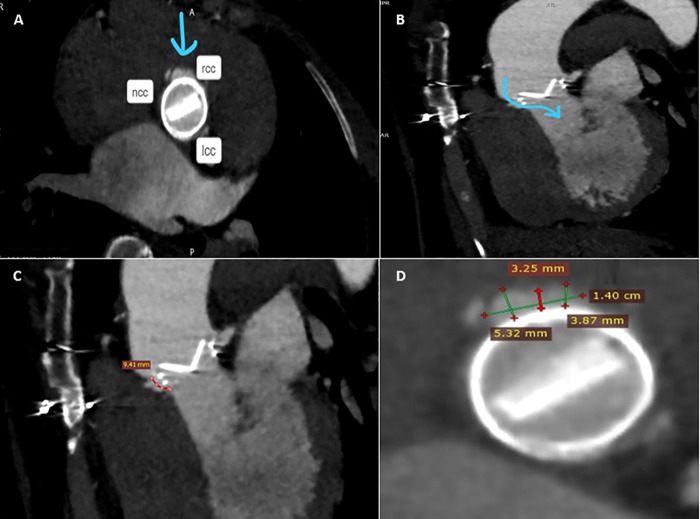 Figure 2
Figure 2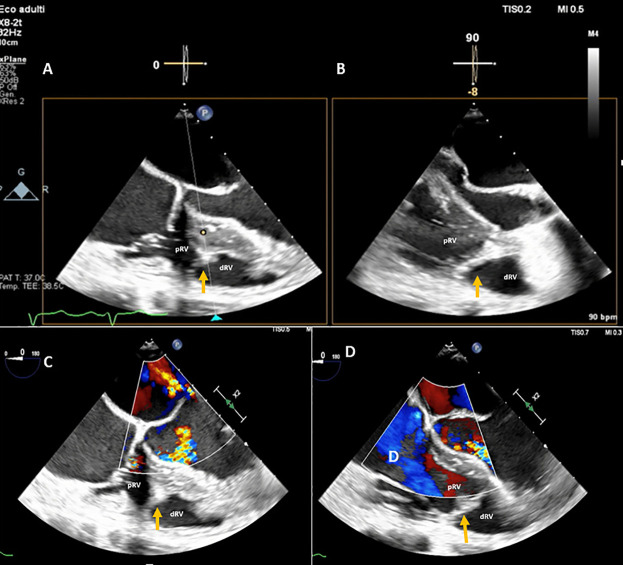 Figure 3
Figure 3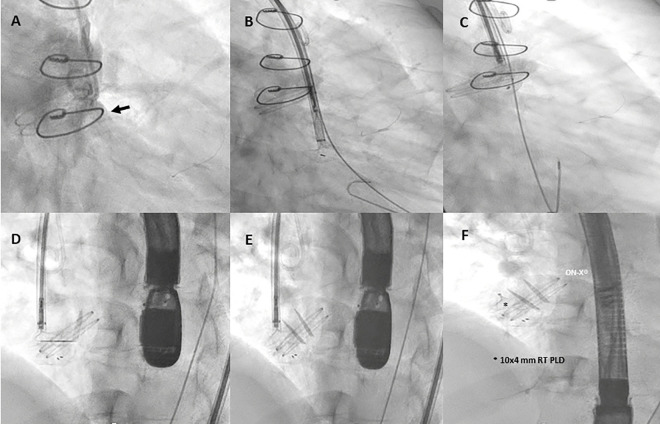 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Cardiac Valve Diseases and Treatments · Cardiac Structural Anomalies and Repair
Introduction
Paravalvular leaks (PVLs) are a known complication following surgical aortic (SAVR) and mitral (SMVR) valve replacements, as well as transcatheter aortic valve implantation (TAVI). They result from an incomplete seal between the prosthetic valve and native annulus due to tissue friability from infection (1) or calcification. PVLs are more common after SMVR (17%) than SAVR (10%) (2–5) and may appear intraoperatively or during follow-up. Late PVLs often stem from suture dehiscence due to prosthetic valve endocarditis (PVE) or residual annular calcifications (6). While 1%–5% of cases lead to heart failure (HF), hemolytic anemia (HA), or left ventricular enlargement (7), transcatheter PVL closure has become a less invasive alternative for high-risk surgical patients (8).
A double-chambered right ventricle (DCRV) is a rare congenital abnormality where hypertrophied muscle bundles divide the right ventricle into high- and low-pressure chambers. Typically diagnosed in childhood, a DCRV may persist into adulthood, often asymptomatically or mimicking other cardiovascular conditions, leading to misdiagnosis (9, 10).
Case summary
A 46-year-old woman with hypertension and dyslipidemia was admitted with congestive heart failure [New York Heart Association (NYHA) class III] in late March 2005. Her history included a silent membranous ventricular septal defect (pmVSD) and severe symptomatic aortic regurgitation. In April 2005, she underwent bioprosthetic aortic valve replacement (Perimount #23, Edwards Lifesciences, USA), with concurrent pmVSD closure using 2-0 Ti-Cron™ polyester sutures. She showed significant clinical improvement with optimal medical therapy and regular follow-up.
Ten years later, the aortic valve prosthesis was replaced with a second bioprosthetic valve (Magna Ease #25, Edwards Lifesciences, USA) due to degeneration. In December 2018, she was hospitalized for sepsis caused by Bordetella hinzii and Propionibacterium granulosum infective endocarditis. A 45-day antibiotic regimen led to the normalization of inflammatory markers. Persistent infection suggested an antibiotic-resistant biofilm on the prosthetic valve (11).
In January 2019, she underwent a third SAVR with a mechanical aortic valve (On-X® #23, Life Technologies, Inc.). Surgical inspection revealed significant paravalvular leakage at the right coronary cusp and fibrous tissue (pannus) extending into the prosthesis orifice. Cultures confirmed Acremonium species infection.
Subsequent imaging (2019–2021) showed mild residual PVL regurgitation with normal valve function. However, by 2024, two-dimensional transesophageal echocardiography (2D TEE) and multidetector computed tomography angiography (MDCTA) confirmed moderate-severe PVL regurgitation (vena contracta width 0.6 cm) near the right coronary cusp (Figures 1, 2). A coincidental DCRV was also identified (Figure 3, Supplementary Video 1). Given the prohibitive surgical risk, transcatheter PVL closure was planned.
Baseline 2D TEE color Doppler at the apical five chamber view (A), at the parasternal long axis view (B,C), at the mid-esophageal (ME) long axis view (D), and at the ME long axis view with Xplane (E), showing an On-X® prosthetic aortic valve with moderate-to-severe regurgitation (orange arrow) through a long paravalvular leakage. Red line, PVL; LV, left ventricle; Ao, aortic valve.
Pre-procedure MDCTA scans with acquired frames confirming the presence of the paravalvular leak, located in close proximity to the right coronary cusp (A), and its channel configuration and length (B,C). Short axis view of the aortic mechanical prosthetic valve showing multiple measurements of the long crescent-shaped PVL (D). rcc, right coronary cusp; lcc, left coronary cusp; ncc, non-coronary cusp.
A DCRV created by an anomalous muscle band (orange arrow) diagnosed with TEE by the presence of a proximal high-pressure region under the tricuspid valve and a low-pressure distal region near the pulmonary valve outflow tract. (A,B) TEE transgastric RV inflow-outflow view (double orifice). (C,D) TEE color Doppler mid-esophageal four-chamber view focused on the RV. pRV, proximal right ventricle; dRV, distal right ventricle.
The procedure was performed in March 2024 under general anesthesia with TEE and angio-fluoroscopic guidance. A hydrophilic guidewire crossed the PVL and was replaced with an Amplatz Super Stiff™ wire. An 8-Fr delivery sheath was advanced, and a 10 mm × 4 mm Occlutech paravalvular leak device (PLD) was successfully deployed, achieving significant leak reduction without prosthetic interference (Figure 4, Supplementary Figure 1). Post-procedure imaging confirmed device stability with a trace-mild residual leak (Supplementary Figure 2). The patient was discharged on postoperative day 3 in better clinical conditions.
Fluoro-angiography procedural steps. (A) Right anterior oblique aortography by pigtail 6-Fr showing PVL regurgitation (black arrow). (B,C) The left disc of a 10 mm × 4 mm rectangular twist (RT) PLD (Occlutech, Helsingborg, Sweden) is opened into the left ventricle through an 8-Fr dedicated delivery sheath (Occlutech ODS III) across the leakage, with a buddy wire (black arrowhead) at its site; (D–F) 10 mm × 4 mm RT PLD successfully deployed and released within the leak without interfering with normal leaflet movement of the On-X® prosthetic aortic valve.
Finally, 3- and 12-month follow-ups confirmed clinical improvement, enhanced quality of life, and device stability with a persistent trace-mild residual leak.
Discussion
PVE accounts for 20% of infective endocarditis cases, leading to valve dysfunction, heart failure, and increased mortality (12, 13). PVE is more frequent in bioprosthetic valves, particularly porcine, due to susceptibility to bacterial colonization (14–16). Our case of B. hinzii and P. granulosum endocarditis is rare. B. hinzii, an emerging Gram-negative pathogen, is often resistant to antibiotics, while P. granulosum requires prolonged culture incubation for detection (17, 18).
These device-related microorganisms can be difficult to eradicate by antibiotic therapy alone. Bacterial biofilms are communities of various microorganisms that adhere to any surface and are enveloped within extracellular polymeric substances (19). Disruption of the bacterial biofilm plays an essential role in recovering the causative agent in the culture. Certain culture and nucleic acid amplification techniques are more accurate in guiding directed treatment regimens. It is clear that diagnostic testing will need to evolve beyond the standard current microbiological procedures to include nucleic acid detection, enhanced culture techniques, novel microbe imaging, and local immune response (20).
Transcatheter PVL closure is a minimally invasive alternative for high-risk patients who are often ineligible for redo surgery (21). PVLs are very heterogeneous in their location, size, and shape, and their track can be tortuous, serpiginous, or heavily calcified.
Undoubtedly, aortic PVL closure is a complex and challenging procedure with several periprocedural complications, such as device malposition or embolization and residual regurgitation, requiring optimal patient selection and comprehensive intraprocedural imaging guidance. Furthermore, a successful PVL reduction results in acute and long-lasting symptomatic improvements in clinical parameters and NYHA class, reducing the need for repeat cardiac surgeries and blood transfusions (22).
PVL closure has been performed in the past with multiple off-label devices that were not specifically designed for the purpose, which had inappropriate designs, shapes, and sizes. In previous studies with off-label devices, technical success rates varied between 62% (23) and 87% (5).
Notably, the Occlutech PLD, designed specifically for PVL closure, offers improved stability and sealing, achieving procedural success in over 90% of aortic PVL cases (24).
DCRV, a rare congenital defect (0.5%–2% of congenital heart disease), typically presents in childhood but can persist asymptomatically in adults (25–29). It results from hypertrophic muscle bands dividing the right ventricle into high- and low-pressure chambers. Though often misdiagnosed, our patient remained asymptomatic with a low-pressure gradient, requiring only medical follow-up.
Conclusion
This case highlights the effectiveness of transcatheter aortic PVL closure as a safe and less invasive alternative for high-risk patients with recurrent infections. The concomitant asymptomatic DCRV required no intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fowler VG Durack DT Selton-Suty C Athan E Bayer AS Chamis AL The 2023 Duke–international society for cardiovascular infectious diseases criteria for infective endocarditis: updating the modified Duke criteria. Clin Infect Dis. (2023) 77:518–26. 10.1093/cid/ciad 27137138445 PMC 10681650 · doi ↗ · pubmed ↗
- 2Kliger C Eiros R Isasti G Einhorn B Kliger C Eiros R Review of surgical prosthetic paravalvular leaks: diagnosis and catheter-based closure. Eur Heart J (2013) 34:638–49. 10.1093/eurheartj/ehs 34723117162 · doi ↗ · pubmed ↗
- 3Cruz-Gonzalez I Rama-Merchan JC Rodríguez-Collado J Martin-Moreiras J Diego-Nieto A Barreiro-Perez M Transcatheter closure of paravalvular leaks: state of the art. Neth Heart J. (2017) 25:116–24. 10.1007/s 12471-016-0918-327878547 PMC 5260617 · doi ↗ · pubmed ↗
- 4Ruiz CE Cohen H Valle-Fernandez RD Jelnin V Perk G Kronzon I. Closure of prosthetic paravalvular leaks: a long way to go. Eur Heart J Suppl. (2010) 12:E 52–62. 10.1093/eurheartj/suq 009 · doi ↗
- 5García E Arzamendi D Jimenez-Quevedo P Sarnago F Marti G Sanchez-Recalde A Outcomes and predictors of success and complications for paravalvular leak closure: an analysis of the Spanis H realw Orld paravalvular L Eaks closure (HOLE) registry. Euro Intervention. (2017) 12:1962–8. 10.4244/EIJ-D-16-0058127973334 · doi ↗ · pubmed ↗
- 6Blackstone EH Kirklin JW Kouchoukos NT Dhasmana JP. Factors associated with periprosthetic leakage following primary mitral valve replacement: with special consideration of the suture technique. Ann Thorac Surg. (1983) 35:170–8. 10.1016/S 0003-4975(10)61456-76337570 · doi ↗ · pubmed ↗
- 7Mc Cullough PA Barnard D Clare R Ellis SJ Fleg JL Fonarow GF Anemia and associated clinical outcomes in patients with heart failure due to reduced left ventricular systolic function. Clin Cardiol. (2013) 36(10):611–20. 10.1002/clc.2218123929781 PMC 4008125 · doi ↗ · pubmed ↗
- 8Otto CM Nishimura RA Bonow RO Carabello BA Erwin JP Gentile F 2020 ACC/AHA guideline for the management of patients with valvular heart disease. J Am Coll Cardiol. (2020) 77(4):e 25–19. 10.1016/j.jacc.2020.11.01833342587 · doi ↗ · pubmed ↗