Sociodemographic and clinical factors related to high rates of unmet supportive care needs among Polish cancer patients
Karolina Osowiecka, Marek Szwiec, Jacek J. Nowakowski, Marcin Kurowicki, Anna Dolińska, Anna Gwara, Eliza Działach, Jarosław Kołb-Sielecki, Weronika Radecka, Sergiusz Nawrocki, Monika Rucińska

TL;DR
Polish cancer patients have high unmet needs in areas like information and material support, especially younger patients and those with digestive or lung cancer.
Contribution
Identifies specific patient groups with high unmet supportive care needs using a validated questionnaire in a large multicenter study.
Findings
The highest unmet needs were in informative and material support areas.
Younger patients, those living with a partner, and those with digestive or lung cancer had higher unmet needs.
Unmet needs are linked to dissatisfaction and poor quality of life in cancer patients.
Abstract
Cancer patients experience a wide range of unmet supportive care needs, which may lead to dissatisfaction with the health care system and poor quality of life. The aims of this study were to assess unmet supportive care needs in five areas: informative needs, psycho-emotional needs, relational needs, material needs and needs related to assistance/care, and to identify groups of cancer patients expressing high rates of unmet needs. The multicenter study was carried out among 1,062 cancer patients between June 2022 and May 2023. The study was performed using the validated Polish version of Needs Evaluation Questionnaire (NEQ). The total and subtotal NEQ scores were calculated. The mean total NEQ score was 0.44 ± 0.27. The highest subtotal NEQ scores were noted in the cases of informative needs and material needs. Predictive factors for a higher total NEQ score were younger age, living…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
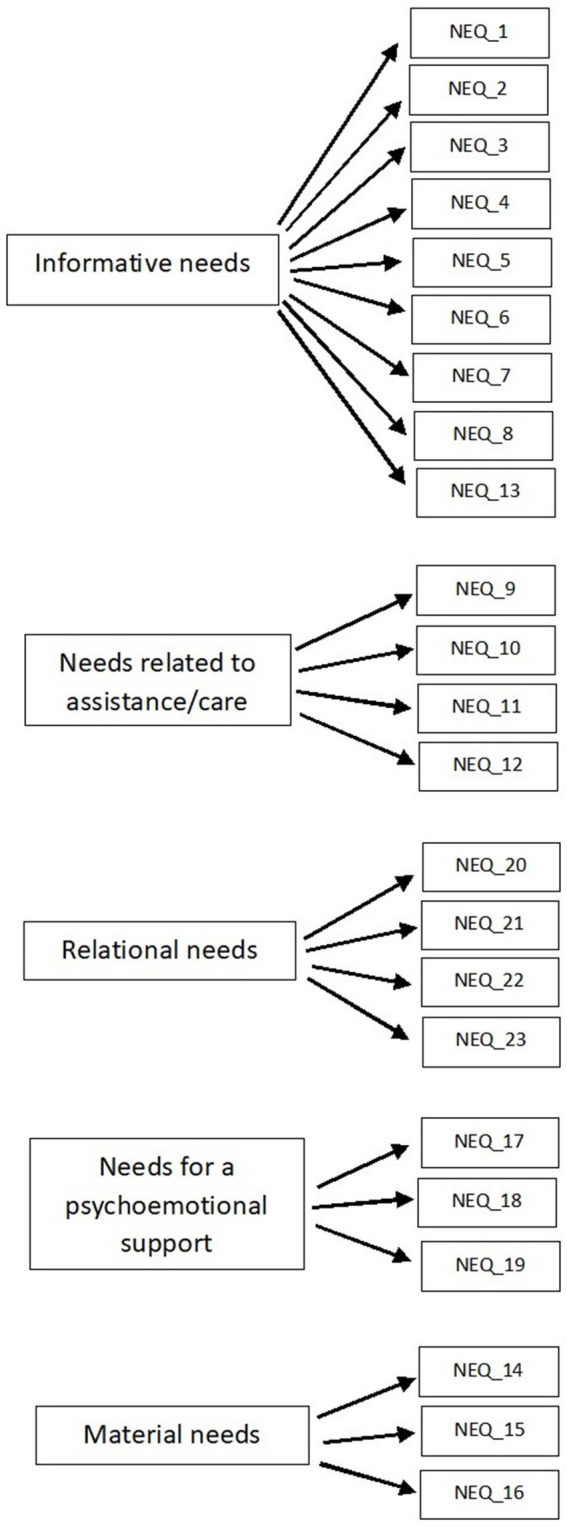 Figure 1
Figure 1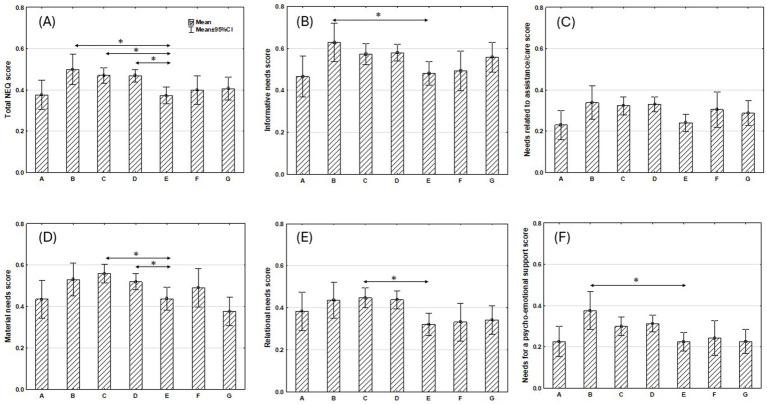 Figure 2
Figure 2| Variables |
| % |
|---|---|---|
| Age: median 66 years (range 22–89 years) | ||
| Gender | ||
| Female | 507 | 47.7 |
| Male | 553 | 52.1 |
| No data | 2 | 0.2 |
| Place of residence | ||
| City | 676 | 63.6 |
| Village | 383 | 36.1 |
| No data | 3 | 0.3 |
| Marital status | ||
| Married | 720 | 67.8 |
| Relationship broken down during disease or in relation to disease | 5 | 0.5 |
| Single | 332 | 31.2 |
| No data | 5 | 0.5 |
| Household | ||
| With partner | 706 | 66.5 |
| With child/children and/or another family member | 166 | 15.6 |
| Alone | 171 | 16.1 |
| No data | 19 | 1.8 |
| Educational level | ||
| Primary | 180 | 17.0 |
| Secondary | 723 | 68.1 |
| High | 147 | 13.8 |
| No data | 12 | 1.1 |
| Employment | ||
| Employed | 236 | 22.2 |
| Unemployed | 41 | 3.9 |
| Pensioner | 780 | 73.4 |
| No data | 5 | 0.5 |
| Physician as a member of family or friends | ||
| Yes | 160 | 15.1 |
| No | 893 | 84.1 |
| No data | 9 | 0.8 |
| Localization of cancer | ||
| Head and neck | 62 | 5.9 |
| Upper digestive system | 71 | 6.7 |
| Lower digestive system | 207 | 19.5 |
| Lung | 300 | 28.2 |
| Breast | 166 | 15.6 |
| Gynecological | 55 | 5.2 |
| Prostate | 109 | 10.3 |
| Brain | 15 | 1.4 |
| Urinary system | 30 | 2.8 |
| Other | 31 | 2.9 |
| No data | 16 | 1.5 |
| Dimension | Informative needs | Needs related to assistance/care | Relational needs | Needs for a psychoemotional support | Material needs |
|---|---|---|---|---|---|
| Informative needs | – | ||||
| Needs related to assistance/care | 0.418* | – | |||
| Relational needs | 0.207* | 0.235* | – | ||
| Needs for a psycho-emotional support | 0.004 | 0.157* | 0.297* | – | |
| Material needs | 0.172* | 0.182* | 0.080 | 0.201* | – |
| Dimension | Item number | Yes | No | No data | ||||
|---|---|---|---|---|---|---|---|---|
|
| % |
| % |
| % | |||
| Informative needs | Q1 | I need more information about my diagnosis | 531 | 50.0 | 525 | 49.4 | 6 | 0.6 |
| Q2 | I need more information about my future condition | 729 | 68.7 | 321 | 30.2 | 12 | 1.1 | |
| Q3 | I need more information about the exams I am undergoing | 580 | 54.6 | 463 | 43.6 | 19 | 1.8 | |
| Q4 | I need more explanations of treatments | 636 | 59.9 | 405 | 38.1 | 21 | 2.0 | |
| Q5 | I need to be more involved in the therapeutic choices | 496 | 46.7 | 532 | 50.1 | 34 | 3.2 | |
| Q6 | I need clinicians and nurses to give me more comprehensible information | 555 | 52.3 | 489 | 46.0 | 18 | 1.7 | |
| Q7 | I need clinicians to be more sincere with me | 608 | 57.3 | 437 | 41.1 | 17 | 1.6 | |
| Q8 | I need to have a better dialogue with clinicians | 508 | 47.8 | 535 | 50.4 | 19 | 1.8 | |
| Q13 | I need to be more reassured by the clinicians | 614 | 57.8 | 422 | 39.7 | 26 | 2.5 | |
| Needs related to assistance/care | Q9 | I need my symptoms (pain, nausea, insomnia, etc.) to be better controlled | 545 | 51.3 | 500 | 47.1 | 17 | 1.6 |
| Q10 | I need more help with eating, dressing, and going to the bathroom | 132 | 12.4 | 914 | 86.1 | 16 | 1.5 | |
| Q11 | I need better respect for my intimacy | 296 | 27.9 | 746 | 70.2 | 20 | 1.9 | |
| Q12 | I need better attention from nurses | 311 | 29.3 | 728 | 68.5 | 23 | 2.2 | |
| Material needs | Q14 | I need better services from the hospital (bathrooms, meals, cleaning) | 590 | 55.6 | 438 | 41.2 | 34 | 3.2 |
| Q15 | I need to have more economic insurance information (tickets, invalidity, etc.) in relation to my illness | 644 | 60.7 | 390 | 36.7 | 28 | 2.6 | |
| Q16 | I need economic help | 330 | 31.1 | 702 | 66.1 | 30 | 2.8 | |
| Needs for a psycho-emotional support | Q17 | I need to speak with a psychologist | 254 | 23.9 | 774 | 72.9 | 34 | 3.2 |
| Q18 | I need to speak with a spiritual advisor | 216 | 20.3 | 813 | 76.6 | 33 | 3.1 | |
| Q19 | I need to speak with people who have this same experience | 426 | 40.1 | 609 | 57.3 | 27 | 2.6 | |
| Relational needs | Q20 | I need to be more reassured by my relatives | 389 | 36.6 | 640 | 60.3 | 33 | 3.1 |
| Q21 | I need to feel more useful within my family | 567 | 53.4 | 468 | 44.1 | 27 | 2.5 | |
| Q22 | I need to feel less abandoned | 364 | 34.3 | 664 | 62.5 | 34 | 3.2 | |
| Q23 | I need to receive less commiseration from other people | 377 | 35.5 | 663 | 62.4 | 22 | 2.1 | |
| Effect | Level of effect | Parameter | 95% CI of parameter | Wald function |
|
|---|---|---|---|---|---|
| Age | −0.002 | −0.004 – −0.001 | 6.739 | 0.009 | |
| Household (Ref.: alone) | With partner | 0.029 | 0.004–0.054 | 5.016 | 0.025 |
| With child/children and/or another family member | 0.004 | −0.029 – 0.037 | 0.051 | 0.822 | |
| Localization of cancer (Ref.: breast) | Head and neck | −0.061 | −0.122 – 0.001 | 3.762 | 0.052 |
| Upper digestive system | 0.072 | 0.013–0.130 | 5.754 | 0.016 | |
| Lower digestive system | 0.049 | 0.011–0.087 | 6.510 | 0.011 | |
| Lung | 0.046 | 0.012–0.080 | 7.185 | 0.007 | |
| Gynecological | −0.040 | −0.105 – 0.024 | 1.493 | 0.222 | |
| Prostate | −0.005 | −0.054 – 0.044 | 0.044 | 0.834 |
| Effect | Level of effect | Parameter | 95% CI of parameter | Wald function |
|
|---|---|---|---|---|---|
| Age | −0.003 | −0.005 – −0.001 | 4.525 | 0.033 | |
| Marital status (Ref.: single) | Married | 0.038 | 0.013–0.064 | 8.716 | 0.003 |
| Physician as a member of family or friends (Ref.: yes) | No | 0.024 | −0.008 – 0.057 | 2.136 | 0.144 |
| Localization of cancer (Ref.: breast) | Head and neck | −0.083 | −0.166 – − 0.001 | 3.906 | 0.048 |
| Upper digestive system | 0.092 | 0.013–0.170 | 5.176 | 0.023 | |
| Lower digestive system | 0.044 | −0.007 – 0.094 | 2.812 | 0.094 | |
| Lung | 0.044 | −0.002 – 0.089 | 3.576 | 0.059 | |
| Gynecological | −0.060 | −0.147 – 0.028 | 1.803 | 0.179 | |
| Prostate | 0.024 | −0.043 – 0.090 | 0.494 | 0.482 |
| Effect | Level of effect | Parameter | 95% CI of parameter | Wald function |
|
|---|---|---|---|---|---|
| Age | −0.004 | −0.007 - − 0.002 | 10.639 | 0.001 | |
| Gender (Ref.: male) | Female | −0.028 | −0.049 - − 0.008 | 7.608 | 0.006 |
| Educational level (Ref.: high) | Primary | 0.038 | 0.001–0.076 | 3.912 | 0.048 |
| Secondary | −0.024 | −0.052 – 0.004 | 2.735 | 0.098 | |
| Employment (Ref.: pensioner) | Employed | −0.009 | −0.055 – 0.037 | 0.148 | 0.701 |
| Unemployed | −0.050 | −0.121 – 0.020 | 1.936 | 0.164 |
| Effect | Level of effect | Parameter | 95% CI of parameter | Wald function | p |
|---|---|---|---|---|---|
| Age | −0.007 | −0.010 – −0.004 | 20.296 | <0.001 | |
| Gender (Ref.: male) | Female | 0.021 | −0.006 – 0.049 | 2.323 | 0.128 |
| Place of residence (Ref.: village) | City | −0.021 | −0.043 – 0.002 | 3.150 | 0.076 |
| Employment (Ref.: pensioner) | Employed | −0.065 | −0.116 – 0.014 | 6.263 | 0.012 |
| Unemployed | 0.070 | −0.008 – 0.148 | 3.066 | 0.080 | |
| Localization of cancer (Ref.: breast) | Head and neck | −0.05 | −0.125 – 0.031 | 1.418 | 0.234 |
| Upper digestive system | 0.064 | −0.011 – 0.138 | 2.830 | 0.093 | |
| Lower digestive system | 0.091 | 0.043–0.138 | 13.742 | <0.001 | |
| Lung | 0.053 | 0.011–0.095 | 6.069 | 0.014 | |
| Gynecological | −0.051 | −0.137 – 0.035 | 1.361 | 0.244 | |
| prostate | −0.035 | −0.102 – 0.031 | 1.075 | 0.299 |
| Effect | Level of effect | Parameter | 95% CI of parameter | Wald function |
|
|---|---|---|---|---|---|
| Age | −0.002 | −0.005 – − 0.001 | 3.107 | 0.078 | |
| Educational level (Ref.: high) | Primary | 0.068 | 0.022–0.113 | 8.367 | 0.004 |
| Secondary | −0.019 | −0.053 – 0.014 | 1.277 | 0.258 | |
| Household (Ref.: alone) | With partner | 0.030 | −0.004 – 0.063 | 2.948 | 0.086 |
| with child/children and/or another family member | 0.013 | −0.032 – 0.057 | 0.306 | 0.580 | |
| Physician as a member of family or friends (Ref.: yes) | No | 0.025 | −0.008 – 0.057 | 2.271 | 0.132 |
| Localization of cancer (Ref.: breast) | Head and neck | −0.018 | −0.099 – 0.063 | 0.194 | 0.660 |
| Upper digestive system | 0.054 | −0.024 – 0.131 | 1.850 | 0.174 | |
| Lower digestive system | 0.070 | 0.020–0.120 | 7.549 | 0.006 | |
| Lung | 0.040 | −0.005 – 0.084 | 3.017 | 0.082 | |
| Gynecological | −0.060 | −0.146 – 0.026 | 1.891 | 0.169 | |
| Prostate | −0.029 | −0.094 – 0.036 | 0.772 | 0.380 |
| Effect | Level of effect | Parameter | 95% CI of parameter | Wald function |
|
|---|---|---|---|---|---|
| Age | −0.002 | −0.005 – 0.001 | 2.073 | 0.150 | |
| Educational level (Ref.: high) | Primary | 0.017 | −0.025 – 0.059 | 0.643 | 0.423 |
| Secondary | −0.052 | −0.082 – − 0.021 | 11.006 | <0.001 | |
| Place of residence (Ref.: village) | City | −0.016 | −0.039 – 0.006 | 2.044 | 0.153 |
| Employment (Ref.: pensioner) | Employed | −0.011 | −0.061 – 0.038 | 0.190 | 0.663 |
| Unemployed | −0.060 | −0.135 – 0.016 | 2.371 | 0.124 | |
| Marital status (Ref.: single) | Married | 0.019 | −0.004 – 0.042 | 2.649 | 0.104 |
| Localization of cancer (Ref.: breast) | Head and neck | −0.046 | −0.121 – 0.028 | 1.474 | 0.225 |
| Upper digestive system | 0.090 | 0.019–0.161 | 6.192 | 0.013 | |
| Lower digestive system | 0.032 | −0.014 – 0.078 | 1.874 | 0.171 | |
| Lung | 0.039 | −0.002 – 0.079 | 3.419 | 0.064 | |
| Gynecological | −0.025 | −0.104 – 0.054 | 0.396 | 0.529 | |
| Prostate | −0.045 | −0.104 – 0.014 | 2.201 | 0.138 |
- —National Science Centre, Poland10.13039/501100004281
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFamily Support in Illness · Cancer survivorship and care · Palliative Care and End-of-Life Issues
Introduction
1
Cancer is a worldwide problem, not only medically, but also socio-psychologically, as it is a particularly destructive disease for patients. Cancer patients experience a broad variety of problems including difficulties with physical functioning, an inability to work, loss of previous social role, marital distress, breakdown of social relationships, sexual dysfunction, daily living functioning (Sanson-Fisher et al., 2000; Malone et al., 1994; Graf et al., 2020; Harrison et al., 2009). Cancer diagnosis can lead to disease-related distress, anxiety, hopelessness, various psychological morbidities (Ahmad et al., 2015; Mehnert et al., 2014; Mielcarek et al., 2016; Zabora et al., 2001), and decreased quality of life (Lewandowska et al., 2020a; Alam et al., 2020; Okediji et al., 2017). There is a potential gap between patients’ psycho-social expectations and oncological health care system service. Deficiencies in non-medical supportive care may lead to cancer patients’ dissatisfaction with treatment (Okediji et al., 2017). Cancer patients experience a wide range of unmet non-medical/supportive care needs (Okediji et al., 2017; Tamburini et al., 2003; Sutherland et al., 2009; Davis et al., 2003; Nixon and Narayanasamy, 2010). Fitch (2000) defined unmet supportive care needs as a lack of support that an individual perceives as necessary to reach the best possible well-being. Unmet needs have been categorized into specific areas: informational, emotional, psycho-social, spiritual, physical and practical (Graf et al., 2020; Evans Webb et al., 2021; Annunziata et al., 2009). Unmet supportive care needs may lead to an inability to cope effectively with distress related to illness and a poorer quality of life (Hack et al., 2010; Fitch and Maamoun, 2016; Park and Hwang, 2012; Cochrane et al., 2022). Bonacchi et al. (2019) showed a positive association between psychological distress and a higher level of unmet needs across all need areas. Uslu-Sahan and Gulcan (2023) observed that the acceptance of cancer was negatively correlated with unmet supportive care needs. It was noted that unmet non-medical needs of cancer patients were negatively correlated with a sense of hope (Ripamonti et al., 2016). Anxiety and depression were also associated with patients’ unmet needs (Erdoğan Yüce et al., 2021; Bunston et al., 1998; Boyes et al., 2012; Akechi et al., 2011; Chambers et al., 2012; Dyson et al., 2012).
There are a variety of supportive care needs related to cancer. Each individual patients will have their own specific needs. Supportive care needs may be influenced by type of cancer, clinical stage, treatment modality and some sociodemographic factors (for example age, sex, marital status, financial status) (Sanson-Fisher et al., 2000; Okediji et al., 2017; Bonacchi et al., 2019; Puts et al., 2012). In Poland, there is a lack of studies on assessing the unmet non-medical needs among cancer patients. To identify supportive care needs some instruments have been designed (Rimmer et al., 2022; Wen and Gustafson, 2004; Richardson et al., 2007; Cassileth et al., 1980). The use of surveys to self-report may help patients to express their expectations. On the other hand, medical staff could more easily identify and meet these needs. Among the instruments available to assess patients’ unmet needs, the Needs Evaluation Questionnaire (NEQ) (Tamburini et al., 2003; Tamburini et al., 2000) seems to be an effective tool. The NEQ is simple, consists of 23 dichotomous questions and takes about 10 min to complete (Tamburini et al., 2000; Bonacchi et al., 2016; Osowiecka et al., 2024). The NEQ is the first validated questionnaire to assess non-medical needs among Polish cancer patients (Osowiecka et al., 2024). The identification of unmet supportive care needs should be a part of cancer policy. It is crucial to identify the individual patients’ real needs and to recognize groups of patients with a higher probability of unmet supportive care needs. Awareness about patients’ unmet needs and concerns is important for planning some interventions which may reduce stress among cancer patients (Bonacchi et al., 2010) and improve patients’ quality of life (Cochrane et al., 2022).
NEQ addresses needs in five domains: informative needs, psycho-emotional needs, relational needs, material needs and needs related to assistance/care (Annunziata et al., 2009). Information needs seems to be the most frequently unmet among cancer patients undergoing oncological therapy (Okediji et al., 2017; Evans Webb et al., 2021). Patients have expressed a need for different types of information related to their disease, examination, treatment options, side effects of treatment and prognosis (Cassileth et al., 1980; Neumann et al., 2011; Fallowfield et al., 1995). Evans Webb et al. (2021) conducted a review including 32 worldwide studies and proved that cancer patients were more likely to receive information about what treatment they would receive, why that treatment was proposed, how it would work, what the likelihood of a cure is, what they can expect from their disease and therapy, how long they would stay in hospital, and when they would return to “normal life” (Evans Webb et al., 2021). The awareness about what information related to disease and treatment patients would like to receive from their oncologists could improve patient-doctor communication (Ha and Longnecker, 2010). Effective identification of information needs seems to help improve a patient’s perception of the disease, treatment decision, understanding doctor’s instructions, compliance with treatment, perception of the future, quality of life, and even treatment outcomes (Sobczak et al., 2018; Zolnierek and Dimatteo, 2009; Mager and Andrykowski, 2002). Neumann et al. (2011) reported that a good patient-doctor relationship (patient’s perception of a high degree of physician empathy) was the most significant predictor of well-met information needs.
Cancer patients have expressed unmet psycho-emotional needs (Driessen et al., 2023; Amenu et al., 2023). Some studies (Tamburini et al., 2003; Bonacchi et al., 2016) reported that cancer patients had a need to speak with people who have had the same experience, to speak with a psychologist and to speak with spiritual assistant. Other study (Neumann et al., 2011) showed that cancer patients wanted information about psychological/psychotherapeutic support (31%) and self-help groups (20%). Giuliani et al. (2016) reported a relatively high level of psychological unmet needs among lung cancer patients. The most frequently indicated unmet needs were “fears of the cancer spreading” and “uncertainty about the future.” Among young adult cancer patients in Japan, psychological needs were the most reported unmet supportive care needs (“fears of spreading of cancer,” “feeling down or depressed” and “anxiety”) (Okamura et al., 2021). Our previous study (Osowiecka et al., 2020) showed that a lot of Polish cancer patients also had this kind of needs. However they received psychological support mainly from family/friends and only 21% of patients got support from psychologist and 4% of them from a priest (Osowiecka et al., 2020). The unmet psychological needs may have the impact on quality of life and higher psychological distress (Cochrane et al., 2022).
Unmet relational needs were also reported among cancer patients. Patients needed to feel more useful in their family, to be more reassured by their relatives and to feel less abandoned (Tamburini et al., 2003; Bonacchi et al., 2016). However, patients needed to be less commiserated by others (Tamburini et al., 2003; Bonacchi et al., 2016). The commiseration from other people was considered as “something negative” and “excessive pitying of someone” by most of previously investigated cancer patients (Osowiecka et al., 2024).
Oncological therapy causes some material needs and need for economic help (Tamburini et al., 2003; Bonacchi et al., 2016). Cancer patients were likely to receive more information regarding social issues how to solve employment legislation problems, health insurance problems, financial problems, etc. (Tamburini et al., 2003; Bonacchi et al., 2016; Neumann et al., 2011; Driessen et al., 2023). In previous study (Osowiecka et al., 2020) only 7% of cancer patients received a sufficient support from a social worker.
It seems that needs related to assistance/care were well met. However some patients needed more support in daily activities, more attention from nurses and more respect for their intimacy (Graf et al., 2020; Tamburini et al., 2003; Bonacchi et al., 2016; Giuliani et al., 2016; Sodergren et al., 2019).The aims of this study were to assess unmet supportive care needs in all those five areas: informative needs, psycho-emotional needs, relational needs, material needs and needs related to assistance/care, and to identify groups of cancer patients expressing high rates of unmet needs.
Materials and methods
2
The study group and design
2.1
Patients
2.1.1
The study was conducted between June 2022 and May 2023 on a group of 1,062 consecutive patients, who were treated for a variety of cancer types in seven oncological centers located in different regions of Poland (Hospital of the Ministry of Internal Affairs with Warmia and Mazury Oncology Center in Olsztyn, The Center for Pulmonary Diseases in Olsztyn, NU-MED Radiotherapy Center in Elblag, Hospital in Prabuty, Oncology Center in Opole, Zaglebiowskie Oncology Center in Dabrowa Gornicza, University Hospital in Zielona Gora).
Sample
2.1.2
The sample size was calculated to be representative for this cross-sectional study (Tabachnick and Fidell, 2007). One thousand hundred and eighty cancer patients met the inclusion criteria: 18 years or older, histopathological confirmation of cancer diagnosis, oncology treatment ongoing or patient having finished treatment no longer than 3 months previously, current hospitalization for at least 3 days or at least one hospitalization due to oncological treatment within the previous 3 months. One thousand sixty-two patients (90%) decided to participate in the study.
Questionnaire
2.2
The study was performed using the Needs Evaluation Questionnaire (NEQ). The NEQ is a self-administered, comprehensive questionnaire that consists of 23 items with responses on a dichotomous scale (yes/no). The NEQ was originally designed and validated among Italian cancer patients (Tamburini et al., 2003; Tamburini et al., 2000). Permission for use of the NEQ in a Polish population was obtained from the authors. According to Annunziata’s distinction (Annunziata et al., 2009) the NEQ was used to assess patients’ needs in five areas (Figure 1).
The five-factor model of the NEQ modified based on Annunziata et al., 2009.
Questionnaire validity and reliability
2.2.1
The psychometric properties of the questionnaire were investigated (Osowiecka et al., 2024). The questionnaire showed good reliability and internal factor structure validity. Confirmatory factor analysis of the selected model showed a good overall fit for the model (χ2 = 518.37; p < 0.001). The values of the estimated fit indices (CFI = 0.801; PNFI = 0.612; SRMR = 0.077) were very close to the values considered to be satisfactory for model fit. All estimated standardized factor loadings ranged from 0.52 to 0.84 and were significantly different from zero at p < 0.001, confirming good levels of internal factor structure validity. In general, inter-correlations between pairs of distinguished groups were very high (>0.7). Only the levels of inter-correlations between informative needs and relational needs and between informative needs and need for psycho-emotional support were close to 0.7. Cronbach’s α indexes for the five factors were ≥0.7. Test–retest reliability coefficients have ranged from 0.60 to 0.95 over a 2-week interval (Osowiecka et al., 2024).
The structure, length and font size of the NEQ were acceptable to respondents. The meanings of the questions were well understood (Osowiecka et al., 2024).
The NEQ was supplemented by questions concerning sociodemographic and clinical data (age, gender, educational level, place of residence, employment, marital status, household, having a physician among family/friends, type of cancer and approximate date of cancer diagnosis). Polish and English versions of the NEQ are presented in Supplementary materials.
Data collection
2.2.2
Patients undergoing oncological therapy (in-and out-patients) were proposed to taking part in the study. Data was collected using a paper questionnaire with eventual help from psychologist or nurse.
Ethical agreement
2.2.3
The study protocol was approved by the Ethics Committee of the University of Warmia and Mazury in Olsztyn (No. 30/2020). Participation in the study was voluntary. All study participants were informed about the aim of the study and gave their signed consent.
Statistical analysis
2.3
The total NEQ score was calculated by summing the total number of unmet needs divided by the number of 23 NEQ items for each patient. Scores for each area of needs were calculated by summing the number of unmet needs in each area divided by the number of needs in that area (informative needs: 9, assistance/care needs: 4, relational needs: 4, psycho-emotional support needs: 3 and material needs: 3). The score for all and each need ranges from 0 to 1. The mean total and subtotal NEQ scores were calculated. The differences between NEQ scores were determined using one-way ANOVA analysis with Tukey’s test of multiple comparisons. Intercorrelations were estimated using partial correlation coefficient. Partial correlations allow for the assessment of the linear degree of association between variables, taking into account the influence of one or more additional variables. The partial correlation coefficient then informs us about the independent influence of a given variable on the dependent variable (when the influence of other variables is eliminated). In contrast to interdependent equations models, recursive models impose constraints on the construction of the equations appearing in the model and if the model is recursive, then only one-way relationships exist between variables. Generalized linear models (GLZ), with the Akaike information criterion (AIC) for normal distribution and identity function, were used to determine the relationship between the supportive care needs and a set of independent variables (age, gender, educational level, place of residence, employment, marital status, household, having a physician among family/friends, type of cancer and time from cancer diagnosis). The best fit GLZ have been presented in this analysis. A p-value of < 0.05 was considered to be significant. The data analysis was conducted using Statistica (data analysis software), version 13. http://statistica.io TIBCO Software Inc., Krakow, Poland (2017) and IBM SPSS Statistics 29.0 software (IBM Corp, 2020).
Results
3
Characteristics of patients
3.1
The study was carried out on a group of 1,062 cancer patients: 52% men and 48% women. Respondents were 22–89 years old (median age 66 years). The majority of patients: lived in cities (63.6%), had graduated from secondary school (68.1%), were pensioners (73.4%), married (67.8%), and living with a partner (66.5%). 15.1% of respondents had a physician in their close family or among friends. Lung cancer, lower digestive system cancers and breast cancer were the most frequent (28.2, 19.5, 15.6%, respectively). The median time from cancer diagnosis was 6 months (Table 1).
Needs prevalence
3.2
The mean total NEQ score was 0.44 ± 0.27. The highest subtotal NEQ scores were noted in the cases of informative needs (mean 0.55 ± 0.37) and material needs (mean 0.49 ± 0.35). Lower subtotal NEQ scores were reported for relational needs (mean 0.40 ± 0.36), needs related to assistance/care (mean 0.30 ± 0.31) and needs for psycho-emotional support (mean 0.28 ± 0.33). The differences between all subtotal NEQ scores for unmet supportive care needs were significant (Tukey’s test: p < 0.001), except for a pair of needs for psycho-emotional support and needs related to assistance/care (p = 0.62). Significant positive correlations were estimated between some of the analyzed domains of all five domains of need (p < 0.05), with partial correlation coefficients indicating a weak association between the variables (Table 2). The frequency of needs in each domain was presented in Table 3.
Association between unmet supportive care needs and sociodemographic and clinical factors
3.3
In the multivariate model the total NEQ score was significantly associated with age, household and cancer localization. The total NEQ score decreased with age (p = 0.009). A higher total NEQ score was observed among patients living with a partner than those living alone (p = 0.03). The highest total NEQ scores were noted in patients diagnosed with upper digestive system cancers, lower digestive system cancers and lung cancer in comparison with the lowest total NEQ score noted among breast cancer patients (respectively, p = 0.016, p = 0.011 and p = 0.007) (Table 4 and Figure 2).
*Mean of total and subtotal NEQ scores due to cancer localization: (A) head and neck cancer, (B) upper digestive system cancer, (C) lower digestive system cancer, (D) lung cancer, (E) breast cancer, (F) gynecological cancer, (G) prostate cancer. Significant differences between subgroups based on GLZ were presented in Tables 4–9.
There was a negative correlation between informative needs score and age (p = 0.03). Higher informative needs scores were reported by married patients than those who were single (p = 0.003) and upper digestive system cancer patients in comparison with breast cancer patients (p = 0.02) (Table 5 and Figure 2).
With age, a significant decrease in the assistance/care needs score was observed (p = 0.001). Higher scores for needs related to assistance/care were noted among males than females (p = 0.006) and patients with a lower educational level compared to those with a higher education (p = 0.048) (Table 6 and Figure 2).
Younger age was a predictor for a higher score of material needs (p < 0.001). Higher material needs scores were reported by pensioners than professionally active patients (p = 0.01) and patients diagnosed with lower digestive system cancer and lung cancer in comparison with breast cancer patients (respectively, p < 0.001 and p = 0.01) (Table 7 and Figure 2).
Higher relational needs scores were expressed by patients with a lower education level in comparison with those who graduated with a higher level (p = 0.004) and lower digestive system cancer patients than breast cancer patients (p = 0.006) (Table 8 and Figure 2).
The need score for psycho-emotional support was significantly higher among patients with higher educational level than lower educational level (p < 0.001) and patients diagnosed with upper digestive system cancer in comparison with breast cancer patients (p = 0.01) (Table 9 and Figure 2).
Discussion
4
Cancer patients experience a wide range of unmet supportive care needs (Okediji et al., 2017; Evans Webb et al., 2021). Multiple areas of non-medical needs have been identified: informational, health care organizational, psychological, spiritual, relational, needs associated with daily living, sexuality, social and material (Okediji et al., 2017; Evans Webb et al., 2021; Bonacchi et al., 2016; Driessen et al., 2023; Wang et al., 2018; Hart et al., 2022). Identification of unmet non-medical needs, as well as characteristics of patients with the greatest unmet needs, is important to support patient wellbeing. Deficits in meeting cancer patients’ needs could lead to dissatisfaction with the health care system and reduce patients’ quality of life (Hack et al., 2010; Fitch and Maamoun, 2016; Park and Hwang, 2012; Cochrane et al., 2022; Jagatap et al., 2020). However, the assessment of supportive care needs is difficult because they are subjective and the importance of each need is different for each individual patient. Unmet needs of cancer patients have been measured using a wide variety of instruments, with different scales, and various psychometric properties (Rimmer et al., 2022; Wen and Gustafson, 2004). Some studies were focused on selected domains such as information needs (Neumann et al., 2011; Ha and Longnecker, 2010; Jenkins et al., 2001; Meredith et al., 1996; Alamanou et al., 2016; Leydon et al., 2000; Hsieh et al., 2018) or psychological and physical needs (Amenu et al., 2023).
Some socio-psycho-demographic factors could influence self-reported needs: age, sex, marital status, educational level, income, receiving relational/psychological support from family/friends, having a physician among close family/friend and clinical factors such as cancer localization, clinical stage of disease, intent for treat (Okediji et al., 2017; Puts et al., 2012; Hart et al., 2022; Gebresillassie et al., 2021). According to Granular Interaction Thinking Theory posits that macro-level order emerges from structured micro-level interactions (Nguyen et al., 2025). Small elements can affect the whole. Based on this theory many minor single factors could affect a patient’s whole well-being. It seems to be necessary to try finding those small things. Unmet needs may be among those elements. There are some studies concerning the unmet supportive care needs in patients diagnosed with only a particular type of cancer: breast and gynecological cancer (Graf et al., 2020; Uslu-Sahan and Gulcan, 2023; von Heymann-Horan et al., 2013), colorectal cancer (Sodergren et al., 2019), lung cancer (Giuliani et al., 2016; Hsieh et al., 2018; Sanders et al., 2010; Li and Girgis, 2006; Yang et al., 2023). Some studies only included patients in certain stage of disease: newly diagnosed (Puts et al., 2012), early stage (Harrison et al., 2009; Okediji et al., 2017), advanced stage (Rimmer et al., 2022; Driessen et al., 2023; Wang et al., 2018; Hart et al., 2022). Some studies were carried out among young patients (Okamura et al., 2021), others among older patients (Puts et al., 2012). It appears that type of cancer, stage of disease and patient’s age could have an impact on results of these studies. Moreover cultural background may have a potential impact on self-reporting of unmet needs by cancer patients. When interpreting the results of studies reported in particularly countries it is important to consider differences in population culture (or possibly mind-set), as well as the organization of the health care system, priorities in health care and economic disparities: Germany (Graf et al., 2020), Scotland (Meredith et al., 1996), UK (Evans Webb et al., 2021; Ha and Longnecker, 2010; Sodergren et al., 2019; Jenkins et al., 2001), US (Neumann et al., 2011), Greece (Alamanou et al., 2016), Nigeria (Okediji et al., 2017), Italy (Tamburini et al., 2003; Bonacchi et al., 2019; Bonacchi et al., 2016; Bonacchi et al., 2018; Chiesi et al., 2017), Denmark (Sodergren et al., 2019), Japan (Okamura et al., 2021), Netherland (Driessen et al., 2023), Turkey (Erdoğan Yüce et al., 2021), Ethiopia (Amenu et al., 2023; Gebresillassie et al., 2021; Amane et al., 2021), Taiwan (Hsieh et al., 2018), Canada (Puts et al., 2012; Giuliani et al., 2016), Australia (Sanson-Fisher et al., 2000; Hart et al., 2022), Hong Kong (Wang et al., 2018), China (Yang et al., 2023).
In Poland there is a lack of studies concerning supportive care needs among cancer patients. In the current study unmet non-medical needs were assessed in a large sample (n = 1,062) of cancer patients. The study included patients diagnosed with different types of cancers. In the analysis different socio-demographic factors were taken into account. The instrument which was chosen to determine the supportive care needs was the NEQ (Tamburini et al., 2003). The heterogeneity of survey methodology used in previous studies has made it difficult to position the results of this analysis in the broader context of published literature. Cancer patients in current study expressed some unmet supportive care needs – the mean total NEQ score was 0.44 (on scale 0–1). In general, higher levels of unmet needs were reported by younger patients, those living with a partner and patients diagnosed with digestive system cancers and lung cancer. Bonacchi et al. (2019), using the same instrument (NEQ) to assess unmet needs among Italian cancer patients, reported a lower total NEQ score than in current analysis (0.30 vs. 0.44). It was shown that Italian cancer patients more frequently reported perceived unmet needs if they had a lower education level and were treated at in-patient clinics (Bonacchi et al., 2019). However, there were no significant differences in self-reported unmet needs by patients associated with age, marital status or cancer localization. In a study among Ethiopian cancer patients, Gebresillassie et al. (2021) and Turkish cancer patients Uslu-Sahan and Gulcan (2023) determined that sex and residence were independent predicting factors for unmet supportive care needs.
In a Danish study (von Heymann-Horan et al., 2013) 41% of 261 breast cancer patients expressed unmet needs. Women, who were younger, single or had a higher level of education were more likely to have unmet supportive care needs (von Heymann-Horan et al., 2013). Giuliani et al. (2016) observed that age and tumor-related factors were associated with supportive care needs among lung cancer patients. Younger age was determined as a factor increasing the tendency to have more unmet needs (Abdollahzadeh et al., 2014).
In the current study the subtotal NEQ score was the highest for informative needs (mean score 0.55). Informative needs included seeking more information about diagnosis, examinations, treatments, future prognosis, and better dialogue with clinicians. The subtotal NEQ score for material needs was also relatively high (mean score 0.49). Material needs included the need for more information about economic insurance in relation to illness, economic help and better services from the hospital (bathrooms, meals, cleaning). Informative needs and material needs were also more frequently reported among Italian cancer patients (mean scores: 0.35–0.48 and 0.28–0.29, respectively) (Bonacchi et al., 2019; Bonacchi et al., 2016; Bonacchi et al., 2018). However, Italian cancer patients in general expressed lower levels of unmet needs in various domains than patients in current study conducted using the same tool. In some studies (Neumann et al., 2011; Ha and Longnecker, 2010; Jenkins et al., 2001; Meredith et al., 1996; Alamanou et al., 2016; Gebresillassie et al., 2021; von Heymann-Horan et al., 2013) cancer patients had the highest unmet supportive care needs in the domains financial and health system and information. Reviews (Okediji et al., 2017; Evans Webb et al., 2021) confirmed that the health system and information domain is the most reported by cancer patients. Patients wished to know what treatment they would receive, why it was chosen, how it worked, what they could expect from therapy, what the possible side effects could be and how they could be relieved. Patients needed more information about their diagnosis, prognosis and the chance of a relapse (Neumann et al., 2011; Ha and Longnecker, 2010; Jenkins et al., 2001; Meredith et al., 1996; Alamanou et al., 2016). In a small, single center Polish study conducted among cancer patients in a hospice showed that informative needs were most frequently expressed (Włostowska et al., 2018). According to a novel theory of information processing in the human mind – Mindsponge, the information cannot be absorbed, it cannot be processed and stored in the mind, and affect the person’s subsequent feeing, thoughts, and behaviors (Vuong, 2023). Cancer-related information could results in patients’ reaction on diagnosis, compliance with treatment and thinking about the future. Therefore, it is not surprising that patients pay special attention to information needs. Informative needs were most frequently expressed at the beginning of the disease and at the time of recurrence/progression (Akechi et al., 2011; Puts et al., 2012; Hsieh et al., 2018; Bonacchi et al., 2018). In the current study there was no significant correlation between time from cancer diagnosis and informative needs. In other studies, the need for more information about disease, treatment etc. were expressed predominantly by patients with breast cancer and hematologic cancer (Alamanou et al., 2016), younger patients (Sanson-Fisher et al., 2000; Evans Webb et al., 2021; Puts et al., 2012; Ha and Longnecker, 2010; Jenkins et al., 2001; Meredith et al., 1996; Alamanou et al., 2016), women (Puts et al., 2012; Meredith et al., 1996), and those with a higher education level (Alamanou et al., 2016). However, Bonacchi et al. (2019) using the same questionnaire (NEQ) did not show differences between informative needs due to age, sex, marital status and educational level. Giuliani et al. (2016) did not observed relationships between supportive care needs in the information domain and age, sex or level of education, marital status or number of household members among lung cancer patients. In the current study sex and education level have not been shown to have a statistically significant influence on informative needs. Whereas the informative needs score was significantly higher among patients who were younger, married or diagnosed with upper digestive system cancer.
The need least expressed by patients in the current analysis was for psycho-emotional support (contact with a psychologist, priest or patients with similar experiences). Some studies indicated that health system, information and psychologic domains of needs were reported at similar high levels to each other (Sanson-Fisher et al., 2000; Puts et al., 2012; Lewandowska et al., 2020b). Other studies indicated psychological needs as most frequently perceived by cancer patients (Driessen et al., 2023; Amenu et al., 2023; Giuliani et al., 2016; Okamura et al., 2021; Sodergren et al., 2019; Amane et al., 2021). Amane et al. (2021) reported that old age was significantly associated with unmet psychological needs among cancer patients. Whereas another study showed in contrast that younger patients were more frequently seeking psychological support (Sanson-Fisher et al., 2000). In the current study age was not reported as an independent predictor of unmet psycho-emotional needs. There were also no differences according to gender. However, in some studies females were more often seeking psychological support (Sanson-Fisher et al., 2000; Giuliani et al., 2016). In the current study there was a significant higher psycho-emotional needs score among patients with a higher education level and those diagnosed with upper digestive system cancer.
The type of cancer had a significant impact on both total and subtotal NEQ scores. Total NEQ score was the highest among patients with upper digestive system cancer and lowest among breast cancer patients. The highest subtotal NEQ score was noted in the case of informative needs for all types of cancers (except gynecological cancer patients: the NEQ score was equal for informative and material needs). Patients with upper digestive system cancer had especial supportive care needs in the information domain. Whereas head and neck, and breast cancer patients expressed the lowest informative needs scores. The same situation was observed in the case of needs related to assistance/care and needs for psycho-emotional support. However, these scores were twice lower than informative needs scores. Relational needs were especially important for patients with lower and upper digestive system cancers as well as lung cancer. Whereas breast cancer patients expressed the lowest relational needs score. Among all unmet non-medical needs, seeking material support was relatively frequently expressed. The highest material needs score was observed in the case of patients with lower digestive system cancer and the lowest in prostate cancer patients. Similar results of high NEQ scores among patients with upper digestive system cancer (pancreas and stomach) were presented by Bonacchi et al. (2019). The authors (Bonacchi et al., 2019) also observed high NEQ score among breast cancer patients but in the current study women with breast cancer did not express as much needs for supportive care. Other authors investigating patients with different cancers showed that breast cancer patients reported the lowest level of unmet supportive care needs (Sanson-Fisher et al., 2000). Some authors indicated the relatively high level of supportive care needs across a range of domains among lung cancer patients (Giuliani et al., 2016; Li and Girgis, 2006).
Breast cancer is a particularly well publicized type of cancer; there are a lot of brochures, information in media and instances where some breast cancer patients share their experiences, etc. This could explain why breast cancer patients have less unmet supportive care needs. Upper digestive system and lung cancer are diseases with a worse prognosis and that may cause more concerns; patients seldom share their experiences and they are under-represented in social media.
Study limitations
4.1
In the current study there were no analyses of anxiety, distress or quality of life among respondents and no mental health measurements were provided. Data on clinical stage or the intention of treatment, which may be potentially associated with the unmet needs of cancer patients, were not collected.
Study implications
4.2
Identification of cancer patients’ unmet non-medical needs should be a part of daily clinical practice. Therefore, an appropriate tool to recognize the patients’ needs should be used. It could help to provide appropriate support to each individual patient.
Conclusion
5
Cancer patients expressed some unmet supportive care needs. It is crucial for improve patient-medical staff communication to investigate what kind of non-medical needs are most important for cancer patients. It seems that meeting unmet informative needs is especially desirable. Identifying groups of patients with high rates of unmet supportive care needs will be useful to find a target for an adequate support. In the current study younger respondents, living with a partner and patients suffering from digestive system cancer or lung cancer seem to require special attention. Younger age was a predictor of unmet informative needs, needs related to assistance/care and material needs. Lower education had an impact on unmet assistance/care and relational needs whereas higher education was related with unmet psycho-emotional needs. Marriage patients desired more information, men - more assistance/care support, pensioners – more material support. Cancer type was a significant factor affecting different domains of needs. Further investigations concerning non-medical needs among cancer patients, especially informative needs are needed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abdollahzadeh F.Moradi N.Pakpour V.Rahmani A.Zamanzadeh V.Mohammadpoorasl A.. (2014). Un-met supportive care needs of Iranian breast cancer patients. Asian Pac. J. Cancer Prev. 15, 3933–3938. doi: 10.7314/apjcp.2014.15.9.3933, PMID: 24935576 · doi ↗ · pubmed ↗
- 2Ahmad S.Fergus K.Mc Carthy M. (2015). Psychosocial issues experienced by young women with breast cancer: the minority group with the majority of need. Curr. Opin. Support. Palliat. Care 9, 271–278. doi: 10.1097/SPC.0000000000000162, PMID: 26147915 · doi ↗ · pubmed ↗
- 3Akechi T.Okuyama T.Endo C.Sagawa R.Uchida M.Nakaguchi T.. (2011). Patient’s perceived need and psychological distress and/or quality of life in ambulatory breast cancer patients in Japan. Psychooncology 20, 497–505. doi: 10.1002/pon.1757, PMID: 20878850 · doi ↗ · pubmed ↗
- 4Alam M. M.Rahman T.Afroz Z.Chakraborty P. A.Wahab A.Zaman S.. (2020). Quality of life (Qo L) of cancer patients and its association with nutritional and performance status: a pilot study. Heliyon 6:e 05250. doi: 10.1016/j.heliyon.2020.e 05250, PMID: 33134577 PMC 7586095 · doi ↗ · pubmed ↗
- 5Alamanou G. D.Balokas A. S.Fotos V. N.Patiraki E.Brokalaki H. (2016). Information needs of cancer patients: validation of the Greek Cassileth's information styles questionnaire. Eur. J. Oncol. Nurs. 20, 49–57. doi: 10.1016/j.ejon.2015.11.002, PMID: 26700140 · doi ↗ · pubmed ↗
- 6Amane H. Y.Tessema A. M.Seid K. A.Hassen A. M.Assen H. E.Asfaw Z. A.. (2021). Factors associated with unmet supportive care needs of oncology patients at Dessie referral hospital, 2020. Ecancermedicalscience 15:1300. doi: 10.3332/ecancer.2021.1300, PMID: 34824623 PMC 8580717 · doi ↗ · pubmed ↗
- 7Amenu A.Aynalem A.Borie Y. A.Jemebere W.Molla E.Samuel B.. (2023). Determinants of unmet physical and psychological supportive care needs among adult cancer patients in southern Ethiopia. BMJ Support. Palliat. Care 14, e 2019–e 2027. doi: 10.1136/spcare-2023-004606, PMID: 37816593 PMC 11671935 · doi ↗ · pubmed ↗
- 8Annunziata M. A.Muzzatti B.AltoèG. (2009). A contribution to the validation of the needs evaluation questionnaire (NEQ): a study in the Italian context. Psychooncology 18, 549–553. doi: 10.1002/pon.1445, PMID: 19021128 · doi ↗ · pubmed ↗