Hyperleukocytosis, leukemoid reaction caused by malignant peritoneal mesothelioma: a case report and review of literature
Kaibo Zhu, Dan Zhou, Kang Liu, Lingzhen Wu, Juan Jin, Zimian Luo

TL;DR
A rare case of a non-hematological cancer causing high white blood cell count highlights the need for broader diagnostic considerations.
Contribution
The case introduces a novel association between malignant peritoneal mesothelioma and paraneoplastic leukemoid reaction.
Findings
Malignant peritoneal mesothelioma can present with hyperleukocytosis mimicking hematological malignancies.
Glucocorticoids may be a potential treatment for paraneoplastic leukemoid reactions.
Early recognition of PLR is crucial to avoid misdiagnosis as leukemia or myeloproliferative neoplasms.
Abstract
Paraneoplastic leukemoid reaction (PLR)-induced hyperleukocytosis remains a critical diagnostic challenge. Malignant peritoneal mesothelioma, known for its nonspecific clinical presentation, often evades early detection. We report a 75-year-old male with cirrhosis presenting with fever (38.2°C), progressive ascites, leukocytosis (109.9×109/L), and elevated CRP (247.41 mg/L). Initial diagnosis of spontaneous peritonitis failed to explain the leukocytosis, prompting bone marrow examination, including cytomorphology and genetic analysis, which turned out do not support a diagnosis of leukemia or myeloproliferative neoplasms. Subsequent peritoneal biopsy confirmed diffuse malignant peritoneal mesothelioma. Despite prompt diagnosis, the patient developed progressive multi-organ dysfunction and died on day 14. This case underscores the imperative to consider PLR as a potential cause of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
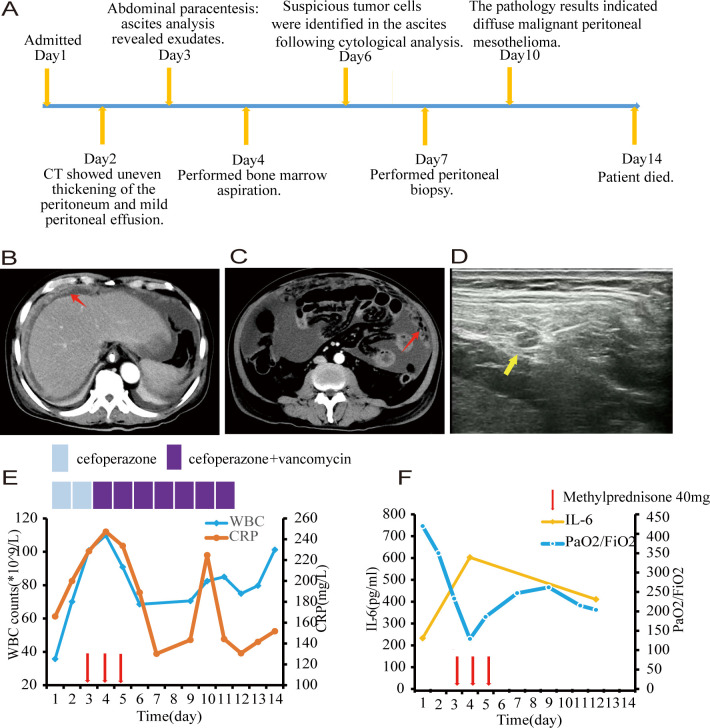 Figure 1
Figure 1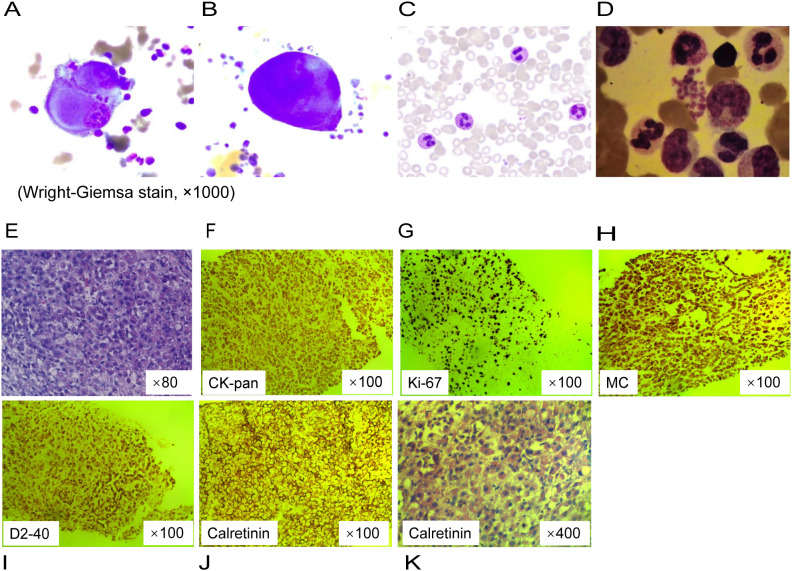 Figure 2
Figure 2| Test item | Test result | Reference range |
|---|---|---|
| White Blood Cell Count | 35.74 | 3.9∼9.1 (×10 9/L) |
| Hemoglobin | 135 | 120∼160 (g/L) |
| Platelet Count | 333 | 85∼303 (×10 9/L) |
| C-reactive Protein | 166 | 0∼ 3 (mg/L) |
| Procalcitonin | 5.2 | 0∼ 0.5 (ng/mL) |
| Lactic Acid | 15.22 | 0∼ 2 (mmol/L) |
| Interleukin-6 | 260 | 0∼ 5.4 (pg/ml) |
| Aspartate Aminotransferase | 67.8 | 0∼ 40 (IU/L) |
| Alanine Aminotransferase | 76.1 | 0∼ 45 (IU/L) |
| Total Protein Level | 73.1 | 60∼85 (g/L) |
| Albumin | 29.9 | 35∼55 (g/L) |
| Lactate Dehydrogenase | 423 | 114∼ 240 (IU/L) |
| Creatinine | 104 | 53∼115 (umol/L) |
| Authors | Publication year | Patient age(y) | Patient gender | Patient country | Primary site | WBC counts (× 109/L) | Survival |
|---|---|---|---|---|---|---|---|
| Ohbayashi H,et al. ( | 1999 | 61 | Male | Japan | pleura | 85.1 | 7 months |
| Kasuga I, et al. ( | 2001 | 48 | Male | Japan | pleura | 64,7 | 7 months |
| Kimura N, et al. ( | 2005 | 70 | Male | Japan | peritoneum | 46.3 | 2 weeks |
| Nishimura M,et al. ( | 2006 | 59 | Male | Japan | pleura | 147.0 | 4 weeks |
| Thakral B,et al. ( | 2020 | 58 | Female | USA | peritoneum | 284 | Unreported |
| Altshuler PC, et al. ( | 2024 | 35 | Female | USA | peritoneum | 52 | 6 months |
- —Natural Science Foundation of Hunan Province 10.13039/501100004735
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOccupational and environmental lung diseases · Acute Myeloid Leukemia Research · Acute Lymphoblastic Leukemia research
Introduction
Paraneoplastic leukemoid reaction (PLR), an infrequent clinical occurrence, is marked by a significant increase in white blood cell(WBC) counts, often surpassing 50×10^9/L, and is typically correlated with carcinomas of the lung, pancreas, stomach, colorectal region, and renal cell carcinomas (1). Diagnosing PLR is a challenge since leukocytosis is most often associated with bacterial infection (2, 3). However when the leukocyte count exceeds 100×10^9/L, which also known as hyperleukocytosis, there is a high potential for misdiagnosis as a hematological malignancy, such as leukemias or myeloproliferative neoplasms, thereby overshadowing the presence of an underlying solid tumor (4). Malignant peritoneal mesothelioma is an uncommon and highly aggressive form of cancer, with a reported one-year survival rate of around 46% (5). Hyperleukocytosis, when caused by malignant peritoneal mesothelioma, is prone to misdiagnosis or may be overlooked, and is rarely documented in medical literature. In this case report, we present an elderly Chinese male patient exhibiting hyperleukocytosis, which was initially suspected to be spontaneous peritonitis or a hematological malignancy, but was ultimately attributed to a PLR associated with diffuse malignant peritoneal mesothelioma. Our goal is to enhance the understanding of rare conditions among clinical physicians and emphasize the importance of accurate and timely diagnosis to prevent diagnostic delays. The study has been approved by the Medical Ethics Committee (IRB No. 2021-10-002) and informed consent has been obtained from the patients.
Case report
A 75-year-old Chinese man was admitted to the hospital for worsening fatigue and poor appetite in the last 10 days. He also complained of fever (max temperature was 38.2°C), slight pain in his right lower abdomen, and weight loss of more than 5 kilograms. He had a history of chronic hepatitis B and was diagnosed with liver cirrhosis one year ago. He had never smoked or abused alcohol, and there was no known family history of cancer.
On physical examination, he appeared well with a blood pressure of 116/72 mm Hg. He had mild tenderness in the right lower quadrant without rebound pain. His laboratory blood tests, as detailed in Table 1, revealed leukocytosis, with a peripheral blood smear indicating 27% band neutrophils and 60% segmented neutrophils in the absence of blasts. The neutrophil alkaline phosphatase score was 245. Computed tomography showed the liver volume decreased, the spleen was slightly enlarged with uneven thickening of the peritoneum and mild peritoneal effusion (Figures 1A-C). Abdominal paracentesis was performed on day 3, and the analysis of his ascites revealed exudates with a gross appearance of yellow. The total nucleated cell count within the fluid was 16×10^9/L, with 60% being polymorphonuclear neutrophils. Biochemical tests of the ascitic fluid indicated a total protein level of 37.2 g/L and a lactate dehydrogenase level of 510 IU/L.
(A) Timeline of key clinical events. (B, C) Computed tomography scans revealed uneven thickening of the peritoneum, as highlighted by the red arrow. (D) Ultrasonographic imaging demonstrated a hypoechoic nodule measuring 1.5 centimeters in diameter with a distinct boundary within the peritoneum, as indicated by the yellow arrow. (E) White blood cell counts and C-reactive protein with time. (F) Interleukin-6 and PaO2/FiO2 with time. Each red arrow indicates 40 milligram of methylprednisone. Note: PaO2/FiO2: ratio of partial pressure of O2 in arterial blood to fraction of inspired oxygen.
Based on the symptoms of fever and abdominal pain, along with leukocytosis and a left shift in the differential count, elevated C-reactive protein(CRP) and procalcitonin as markers of infection, thickening of the peritoneum, and exudative ascites, a diagnosis of post-hepatitis cirrhosis complicated with spontaneous bacteria peritonitis was made and the patient received cefoperazone monotherapy for 48 hours followed by combined with vancomycin to fight against bacterial infection. However, both blood and ascites bacterial cultures were sterile. A metagenomic next-generation sequencing analysis targeting pathogens using a peritoneal fluid sample was performed, which turned out to be negative also. Despite the use of broad-spectrum antibiotics, his symptoms were not alleviated and the WBC count and CRP were getting higher and higher (109.9×10^9^/L and 247.41mg/L, respectively) (Figure 1E).
During his leukocytosis, at its peak, the patient experienced respiratory distress. Given concerns regarding leukostasis and potential pulmonary damage from elevated cytokines, he was administered 40mg of methylprednisolone daily for three days. The patient reported significant improvement in his mental state, appetite, and dyspnea, with overall symptom relief. Both the WBC count and CRP levels decreased significantly, however, the improvement was short-lived. Simultaneously, his ascitic fluid volume increased significantly (Figure 1F).
Through cytological examinations of the ascites, suspicious tumor cells were identified (Figures 2A, B). Subsequently, an ultrasound-guided peritoneal biopsy was performed (Figure 1D), and microscopic examination revealed diffuse malignant mesothelioma, the immunohistochemical results showed Vim(+),CK-pan(+),S-100(-),EMA(dim+),CK5/6(+),CR(-),MC6(+),Desmin(focal+),Myogenin(-),Mum-1(-),HMB45(-),CEA(-),D2-40(+),Wt-1(focal,dim+),Villin(-),CDX-2(-), Ki-67(+) (Figures 2E-K).
Cytological analysis and pathological findings of peritoneal biopsy tissue. (A, B) Clustered giant and abnormally shaped cells with malformed nuclei, and prominant nucleoli on ascites cell smear. (C) Segmented neutrophils containing multiple cytoplasmic granules on the peripheral blood smear. (D) Bone marrow examination showed left-shifted granulocytic hyperplasia without morphologic dysplasia. (E) Diffuse epithelioid cells with pink cytoplasm and nucleolus, focal tumor necrosis on pathology slide of a peritoneal nodule (hematoxylin and eosin stain). (F–J) Immunohistochemistry. (K) Prominent atypical hyperplastic epithelioid cells, diffusely distributed and arranged, with abundant eosinophilic cytoplasm and displaced nuclei.
Given the hyperleukocytosis, a bone marrow aspiration was conducted to exclude a hematological malignancy. The morphological analysis revealed a markedly hypercellular marrow without evidence of dysplasia or increased blast cells; the granulocyte-to-erythrocyte ratio was noted to be 4:1 (Figure 2C, D). Molecular studies, including polymerase chain reaction for colony stimulating factor 3 receptor (CSF3R) mutation and fluorescence in situ hybridization for the BCR::ABL1 fusion gene, were negative, effectively ruling out chronic neutrophilic leukemia and chronic myeloid leukemia, respectively. The bone marrow karyotype was normal at 46, XY [20]. Thus, these findings do not support a diagnosis of leukemia or myeloproliferative neoplasms.
When the patient was first admitted, he believed that his condition was a routine peritonitis and that he would recover quickly after treatment. Unfortunately, he was later diagnosed with a rare malignant neoplasm, and his condition deteriorated day by day. His confidence in treatment was shattered. Ultimately, he chose to receive palliative care. On the 14th day of hospitalization, the patient died of multiple organ failure.
Discussion
Malignant peritoneal mesothelioma is a rare and highly aggressive disease, accounting for approximately 10-15% of all malignant mesothelioma cases. Its clinical presentation and imaging characteristics can often mimic other intra-abdominal pathologies, such as spontaneous bacterial peritonitis, particularly in patients with liver cirrhosis (6). In this case, the patient presented with leukocytosis and clinical symptoms suggestive of an infection. The cefoperazone administered to the patient is a β-lactam antibiotic, which is primarily used to treat infections caused by susceptible Gram-negative bacteria. Vancomycin, on the other hand, is a broad-spectrum antibiotic that targets resistant Gram-positive bacteria, particularly vancomycin-resistant enterococci. Together, these two antibiotics provide comprehensive coverage against the common bacterial pathogens responsible for peritonitis. However, the lack of improvement in symptoms despite antimicrobial therapy raised the possibility of a different underlying cause. Cytological examination of the ascites and immunohistochemical staining were pivotal in confirming the diagnosis of malignant peritoneal mesothelioma. The positive expression of Vimentin (Vim), Cytokeratin pan (CK-pan), D2-40, and Weighted-100 (Wt-1) provided critical diagnostic evidence. Additionally, bone marrow morphological evaluation, along with clonality assessments through cytogenetic and molecular analyses, ruled out leukemia or myeloproliferative neoplasms. These findings were consistent with the diagnosis of PLR as a response to the diffuse malignant peritoneal mesothelioma.
Literature review has identified 179 cases of PLR, with the esophagus, gallbladder, lung, liver, and pancreas being the most common primary sites. In 22% of cases, the white blood cell count exceeded 100×10^9/L (7). However, the absence of malignant mesothelioma cases in this study suggests that PLR secondary to mesothelioma are infrequently noted and documented. We have summarized 6 cases of malignant mesothelioma as shown in Table 2 (8–13). In these cases, the longest survival duration was only seven months, suggesting that patients with PLR may have a worse prognosis. Consistent with our findings, a cohort study of 142 pleural mesothelioma cases identified a WBC count exceeding 8.3×10^9/L as a poor prognostic factor (14). Similarly, in other types of tumors, PLR is associated with an aggressive disease course and poor prognosis, and a strong correlation between worsening of tumor burden and aggravation of neutrophilia was observed (15, 16). A cohort study of 17 PLR patients with a WBC count greater than 50×10^9/L reported a very high mortality rate of 76% within the first 30 days, with most patients having disseminated neoplasm (1). In a previous study, clinical outcomes of patients with PLR were poor, with 78%(60/77) patients either discharged to hospice or dying within 12 weeks (17). Patients with a WBC count >100 ×10^9^/L were twice as likely to die as those with the count from 11×10^9^/L to 40 ×10^9^/L (7). Consistent with the reported data, our case rapidly deteriorated and resulted in death within 14 days.
The pathogenesis of PLR is not well understood, it is a complex and multifactorial process involving the dysregulated release of various cytokines. A retrospective, single-center study observed a strong correlation between the worsening of tumor burden and the aggravation of neutrophilia during PLR in patients with advanced melanoma. In this study, cytokine measurements revealed an increase in proinflammatory cytokines, including interleukin-6(IL-6) and interferon-γ, as well as granulocyte colony-stimulating factor (G-CSF). Additionally, immunohistochemistry confirmed the infiltration of neutrophils into tumor tissue (18). Through cellular experiments, it has been demonstrated that mutations in ras proto-oncogenes may lead to alterations in the expression of various cytokine genes, including G-CSF, granulocyte-macrophage colony-stimulating factor, IL-1, and IL-6, through both transcriptional and post-transcriptional mechanisms (19). Furthermore, G-CSF production has been confirmed through the detection of G-CSF mRNA in the extracts of primary pericardial mesothelioma and elevated serum G-CSF levels in patients (8, 20). The first case of a malignant mesothelioma expressing both G-CSF and its receptor was reported by Motohiro Nishimura (11). However, there is no absolute correlation between white WBC count and serum G-CSF levels. Thakral reported a similar case in which WBC count peaked at 284×10^9/L while serum G-CSF levels remained normal, reflecting the complexity of the PLR mechanism (7, 12). In our case presentation, due to the lack of test reagents, we did not test for G-CSF, but increased serum IL-6 levels were detected (Figure 1F), and the therapeutic response to glucocorticoids was notable underscoring the significant role of cytokines in the pathogenesis of PLR. Glucocorticoids effectively alleviate cytokine storm by inhibiting the production of inflammatory cytokines and the cytokine cascade through multiple mechanisms, including the suppression of key pro-inflammatory transcription factors, modulation of immune cell functions, and blockade of cytokine cascades. This observation necessitates further investigation. In addition to the observed elevation in IL-6 levels, the accumulation of additional data supports the potential emerging role of IL-6 as a therapeutic target for the treatment of PLR.
Hyperleukocytosis, defined by a WBC count exceeding 100×10^9/L, represents a medical emergency. In leukemia, high WBC count and leukocyte aggregates result in leukostasis, disseminated intravascular coagulation, and tumor lysis syndrome, which needs emergent cytoreduction therapy with/without leukopheresis (4, 21, 22). However, hyperleukocytosis in PLR is very rarely reported and marginally analyzed in therapeutic strategies. Few experiences advocated emergent leukapheresis or exchange transfusion for hyperleukocytosis accompanied by respiratory distress or cardiovascular instability in children (23–26). It is much less explored whether glucocorticoid may be needed in leukemoid reaction complicating hyperleukocytosis. In our case, we gave the patient methylprednisone to reduce the leukostasis and damage of cytokines to the lungs, which seemed to have an ephemeral effect, this implies anti-inflammatory therapy may play a role in PLR patients with severe inflammatory response, especially before cancer treatment can be started. Nevertheless, this case report has its limitations, primarily due to its retrospective nature and the lack of a large patient cohort for analysis.
In conclusion, this case highlights the rapid progression and early mortality associated with PLR secondary to malignant peritoneal mesothelioma, underscoring that hyperleukocytosis is not necessarily indicative of a hematological malignancy and warrants vigilance for underlying malignancies to prevent delayed diagnosis and treatment. Additionally, histopathological examination is crucial in cases of unexplained ascites and peritoneal thickening.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Portich JP Faulhaber GAM. Leukemoid reaction: A 21st-century cohort study. Int J Lab Hematol. (2020) 42:134–9. doi: 10.1111/ijlh.13127 31765058 · doi ↗ · pubmed ↗
- 2Riley LK Rupert J. Evaluation of patients with leukocytosis. Am Family Physician. (2015) 92:1004–11.26760415 · pubmed ↗
- 3Potasman I Grupper M. Leukemoid reaction: spectrum and prognosis of 173 adult patients. Clin Infect Dis. (2013) 57:e 177–e 81. doi: 10.1093/cid/cit 562 23994818 · doi ↗ · pubmed ↗
- 4Ganzel C Becker J Mintz PD Lazarus HM Rowe JM. Hyperleukocytosis, leukostasis and leukapheresis: practice management. Blood Rev. (2012) 26:117–22. doi: 10.1016/j.blre.2012.01.003 22364832 · doi ↗ · pubmed ↗
- 5Ullah A Waheed A Khan J Mishra A Tareen B Nama N. Incidence, survival analysis and future perspective of primary peritoneal mesothelioma (PPM): A population-based study from SEER database. Cancers (Basel). (2022) 14:942–52. doi: 10.3390/cancers 14040942 PMC 886982935205689 · doi ↗ · pubmed ↗
- 6Chun C-P Song L-X Zhang H-P Guo D-D Xu G-X Li Y. Malignant peritoneal mesothelioma. Am J Med Sci. (2022) 365(1):99–103. doi: 10.1016/j.amjms.2022.07.008 35940275 · doi ↗ · pubmed ↗
- 7Abukhiran I Mott SL Bellizzi AM Boukhar SA. Paraneoplastic leukemoid reaction: Case report and review of the literature. Pathol Res Practice. (2021) 217:153295. doi: 10.1016/j.prp.2020.153295 33341546 · doi ↗ · pubmed ↗
- 8Ohbayashi H Nosaka H Hirose K Yamase H Yamaki K Ito M. Granulocyte colony stimulating factor-producing diffuse Malignant mesothelioma of pleura. Intern Med. (1999) 38:668–70. doi: 10.2169/internalmedicine.38.668 10440505 · doi ↗ · pubmed ↗