Staphylococcus cohnii Causing a Latent Endophthalmitis: A Case Report
Hassan Javed Ahmed, Christos Christakopoulos, Steffen Heegaard

TL;DR
A 72-year-old woman developed a delayed eye infection caused by Staphylococcus cohnii after cataract surgery, requiring multiple treatments and lens removal.
Contribution
This case report highlights Staphylococcus cohnii as a rare but important cause of latent postoperative endophthalmitis.
Findings
Staphylococcus cohnii was identified as the causative agent in a case of delayed endophthalmitis.
The infection was associated with biofilm formation, complicating treatment and leading to implant failure.
Multiple surgical interventions were required to manage the persistent intraocular infection.
Abstract
Objective: We report a case of latent postoperative endophthalmitis caused by Staphylococcus cohnii in a 72-year-old woman. Observation: The patient was referred to the department of ophthalmology with blurry vision in her right eye 12 days after phacoemulsification. The clinical examination showed signs of endophthalmitis. A vitreous tap, with intraocular injection of ceftazidime, was performed, and topical dexamethasone and tobramycin were initiated. The postoperative follow-up showed reduction in the intraocular reaction, and the patient was afterwards discharged. After 6 months, her private ophthalmologist referred the patient again with signs of uveitis and macular edema. The clinical examination showed hypopyon and infiltrates on the posterior lens capsule which led to a vitrectomy with the removal of the posterior lens capsule infiltrate. With no signs of improvement at the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
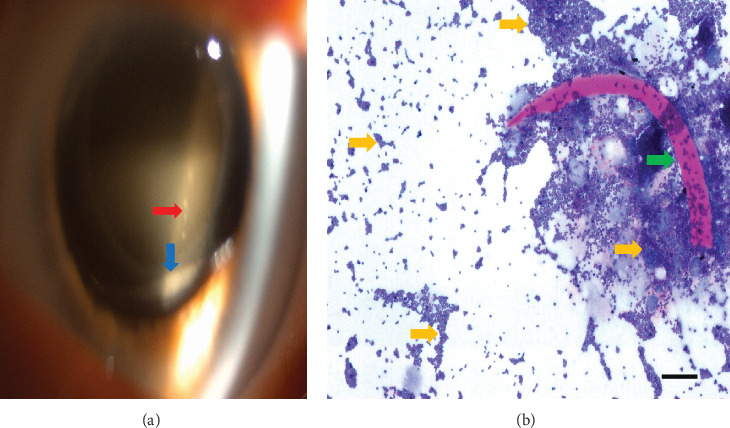 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Infections and Treatments · Ocular Diseases and Behçet’s Syndrome · Bacterial biofilms and quorum sensing
1. Introduction
Endophthalmitis can occur as a sequela of intraocular procedures, trauma, or an endogenous source [1]. It is a rare but dreaded complication after intraocular surgery, with an estimated incidence rate of 0.05%–1.8% [1, 2], but with potentially devastating outcome. Early diagnosis and prompt treatment are crucial for outcome. Infection is the most common cause, with Staphylococcus epidermidis (70%) [3] being the most common pathogen. Here, we describe a case of latent endophthalmitis caused by Staphylococcus cohnii.
2. Case Presentation
A 72-year-old woman was referred to our department with blurry vision on the right eye (RE) 12 days after phacoemulsification. Her best corrected visual acuity (BCVA) was 0.4 on the RE. The clinical examination showed ciliary injection, intraocular reaction (IOR) (10 cells/field, 1+), and vitritis without retinal hemorrhages. A vitreous tap was performed with intraocular injection of ceftazidime and vancomycin, and topical dexamethasone and tobramycin (Tobradex) were initiated. The postoperative follow-up showed reduction in the IOR in the anterior chamber and no vitritis. The microbiological analysis showed polymorphonuclear and mononuclear leucocytes. The patient was discharged with BCVA 0.5 on Tobradex. Six months later, she was referred again with uveitis and macular edema on the RE. She had been treated for 3 weeks with ketorolac (Acular) and dexamethasone (Maxidex) by her private ophthalmologist with no signs of improvement. BCVA on the RE was 0.5. Findings included IOR+2 and vitritis. Treatment with Acular and Maxidex was intensified to four times daily. After 6 weeks, fluorescein angiography was performed, suggesting inflammatory macular edema. The patient was treated with one peribulbar triamcinolone (40 mg) injection. Worsening of symptoms was recorded after 1 month, and biomicroscopy showed hypopyon in the capsular bag, fluffy posterior lens capsule infiltrates (Figure 1a), and dense IOR (> 20 cells/field 3+). Vitrectomy, with the removal of the posterior lens capsule infiltrate and intraocular injection of ceftazidime and vancomycin, was performed on suspicion of recurrence of endophthalmitis. Bacterial cultures returned negative, but pathologic examination and microscopy with H&E, Gram, and Periodic Acid Schiff staining showed gram-positive cocci in direct contact to the lens capsule (Figure 1b). Polymerase chain reaction (PCR) was then performed on the vitreous and lens capsule sample, detecting DNA of Staphylococcus cohnii. Subsequent intraocular injection with vancomycin was given 2 months later due to recurrence. Due to lack of improvement, the intraocular lens (IOL) and lens capsule were removed. Four months later, an anterior chamber IOL implant was inserted in the RE. Finally, after obtaining quiescence, the patient was discharged 3 months later with BCVA of 0.5 on RE.
3. Discussion
Staphylococcus cohnii is a gram-positive coagulase-negative member of the bacterial genus Staphylococcus. It is commonly found on human skin and mucous membranes [4]. It has rarely been described as an opportunistic pathogen, causing urinary tract infections, endocarditis, and bacteremia [5]. The increasing frequency of its detection as an opportunistic pathogen has been attributed to the bacteria's production of biofilm [6], thus promoting adherence to medical devices. Biofilm may protect bacteria against immunological host defence mechanisms and antimicrobial chemotherapy [7].
This case documents endophthalmitis due to Staphylococcus cohnii, which was confirmed with PCR and bacterial cultures of the IOL. Contrary to the typical course of acute endophthalmitis, this case did not manifest rapid exacerbation or permanent retinal damage. Bacterial culture of the microorganism was not possible on vitreous gel biopsy, probably because of biofilm coating. Microbiological diagnosis became possible with PCR examination of the vitreous gel samples, and cure was achieved only after IOL removal.
4. Conclusion
In conclusion, Staphylococcus cohnii is a rare causative agent in cases of latent endophthalmitis [8] and should be considered in cases not responding to intravitreal antibiotics. Hypopyon in the capsular bag is a rare manifestation of postoperative endophthalmitis [9], which in our case was assumed caused by biofilm producing bacteria. In such cases, removal of the implant should be considered.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kresloff M. S. Castellarin A. A. Zarbin M. A. Endophthalmitis Survey of Ophthalmology 199843319322410.1016/s 0039-6257(98)00036-82-s 2.0-00317371909862309 · doi ↗ · pubmed ↗
- 2Callegan M. C. Engelbert M. Parke D. W.2nd Jett B. D. Gilmore M. S. Bacterial Endophthalmitis: Epidemiology, Therapeutics, and Bacterium-Host Interactions Clinical Microbiology Reviews 200215111112410.1128/CMR.15.1.111-124.20022-s 2.0-003614298011781270 PMC 118063 · doi ↗ · pubmed ↗
- 3Durand M. L. Bacterial and Fungal Endophthalmitis Clinical Microbiology Reviews 201730359761310.1128/CMR.00113-162-s 2.0-8501660553228356323 PMC 5475221 · doi ↗ · pubmed ↗
- 4Garza-González E. Morfin-Otero R. Martínez-Vázquez M. A. Gonzalez-Diaz E. González-Santiago O. Rodríguez-Noriega E. Microbiological and Molecular Characterization of Human Clinical Isolates of Staphylococcus cohnii, Staphylococcus hominis, and Staphylococcus sciuri Scandinavian Journal of Infectious Diseases 20114311-1293093610.3109/00365548.2011.5988732-s 2.0-8075513017321851333 · doi ↗ · pubmed ↗
- 5Stefano M. Del Rosso A. Saldutto P. Paradiso Galatioto G. Vicentini C. Intrascrotal Abscess, Propionibacterium acnes and Staphylococcus cohnii ssp. cohnii: A Case Report and Review of the Literature Case Reports in Urology 2012201231369410.1155/2012/31369423227417 PMC 3514819 · doi ↗ · pubmed ↗
- 6Mendoza-Olazarán S. Garcia-Mazcorro J. F. Morfín-Otero R. Draft Genome Sequences of Two Opportunistic Pathogenic Strains of Staphylococcus cohnii Isolated From Human Patients Standards in Genomic Sciences 2017121 p. 4910.1186/s 40793-017-0263-12-s 2.0-8502860683428878860 PMC 5580220 · doi ↗ · pubmed ↗
- 7Arciola C. R. Campoccia D. Montanaro L. Implant Infections: Adhesion, Biofilm Formation and Immune Evasion Nature Reviews. Microbiology 201816739740910.1038/s 41579-018-0019-y 2-s 2.0-8504633871529720707 · doi ↗ · pubmed ↗
- 8Zhang Y. Endophthalmitis Associated With Staphylococcus cohnii After Vitrectomy and Silicone Oil Insertion: A Case Report Medicine (Baltimore) 202310250 e 3657410.1097/MD.000000000003657438115335 PMC 10727602 · doi ↗ · pubmed ↗