SARS-CoV-2 Antibodies in Response to COVID-19 Vaccination in Underserved Racial/Ethnic Minority People Living with HIV
Yongjun Huang, Haley R. Fonseca, Leonardo Acuna, Wensong Wu, Xuexia Wang, Samantha Gonzales, Manuel Barbieri, David R. Brown, Marianna K. Baum

TL;DR
This study found that people with HIV and lower CD4+ T cell counts had weaker immune responses to the COVID-19 vaccine, highlighting the need for targeted care in underserved populations.
Contribution
The study identifies CD4+ T cell count and HIV viral load as key factors affecting vaccine response in racial/ethnic minority people living with HIV.
Findings
PLWH with lower CD4+ T cell counts had reduced SARS-CoV-2 antibody titers after vaccination.
Higher HIV viral load was associated with diminished immune response to the vaccine.
Vaccinated PLWH were more likely to be virally suppressed and have higher CD4+ T cell counts.
Abstract
Background: Understanding immune response is essential for preparing for public health crises. COVID-19 vaccination provides robust immunity against SARS-CoV-2, but immunocompromised populations may have weaker immune responses. We assessed SARS-CoV-2 spike (trimer) total IgG/IgM/IgA (total Ig) to investigate immune response to COVID-19 vaccination in people living with HIV (PLWH), considering CD4+ T cell count, viral load, substance use, and comorbidities. Methods: This cross-sectional study was conducted in Miami, Florida, between May 2021 and December 2021 as part of the NIH Rapid Acceleration of Diagnostics-Underserved Populations (RADx-UP) initiative (3U01DA040381-05S1) and the Miami Adult Studies on HIV (MASH) cohort (U01DA040381). Blood samples were collected and SARS-CoV-2 spike (trimer) total Ig was quantified. HIV serostatus, viral load, CD4+ T cell count, and COVID-19…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
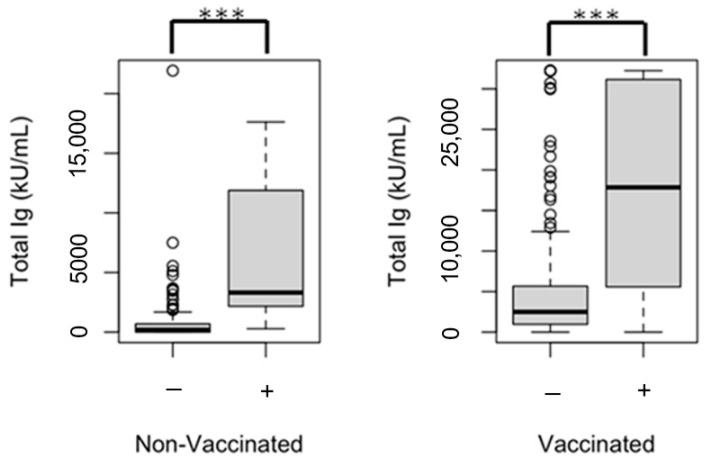 Figure 1
Figure 1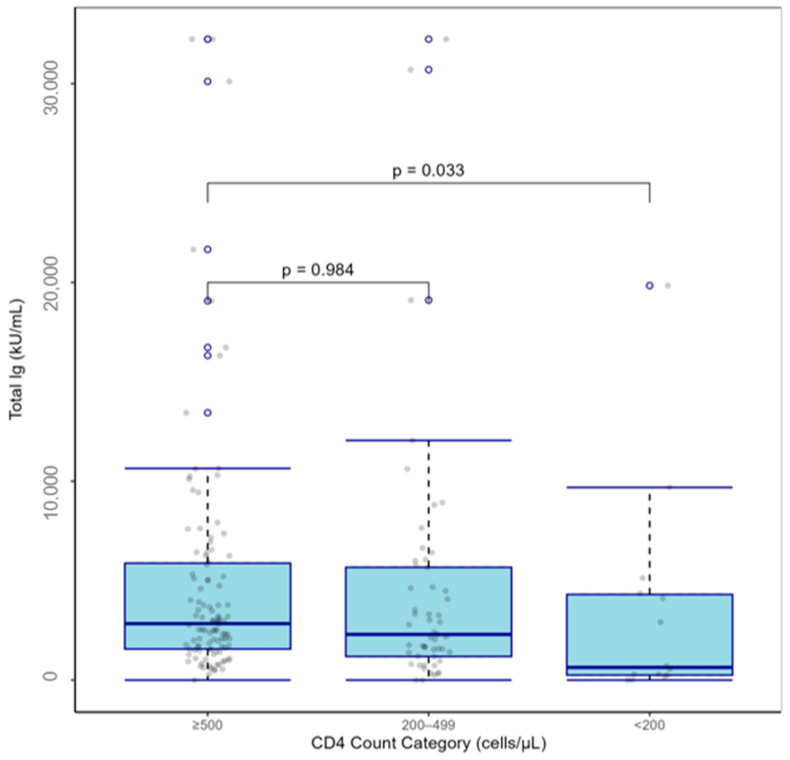 Figure 2
Figure 2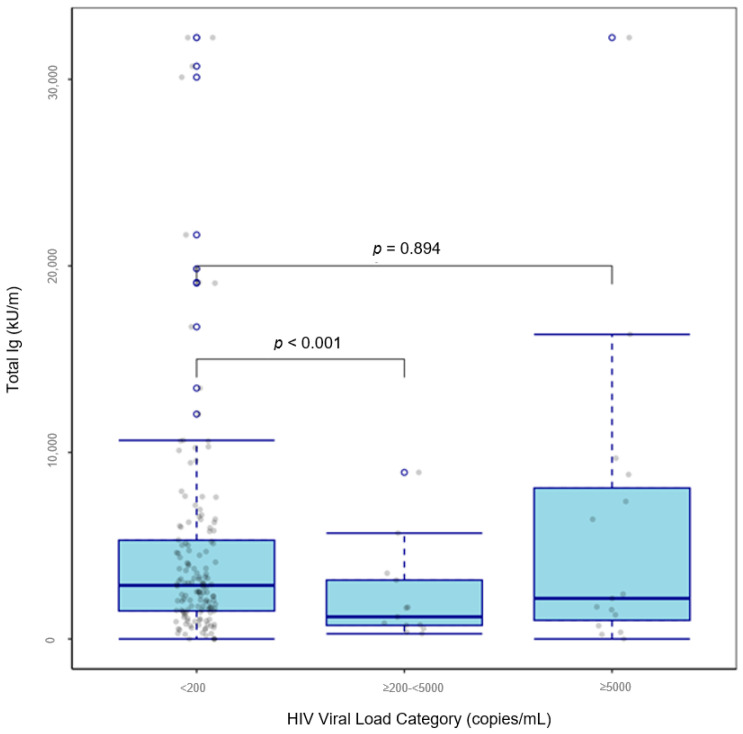 Figure 3
Figure 3- —National Institutes of Health, the National Institute on Drug Abuse
- —National Institute on Minority Health and Health Disparities
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research · Vaccine Coverage and Hesitancy · COVID-19 Impact on Reproduction
1. Introduction
People living with HIV (PLWH) have a greater risk of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and the development of severe Coronavirus disease-2019 (COVID-19) [1,2,3]. The degree of risk is, in part, dependent on the management of HIV viremia, which negatively impacts host immune response [3,4]. A successful immune response results from the coordinated efforts of white blood cells such as B cells, T cells, and antibodies (immunoglobulins [Ig]) [5,6]. These components work together in a highly orchestrated manner to recognize, neutralize, and eliminate pathogens, and provide long-term protection through the generation of memory B cells [5,6]. In PLWH, these elements, particularly CD4^+^ T cells, are diminished [7,8]. The depletion of CD4^+^ T cells weakens the ability to mount an effective immune response, making individuals more susceptible to opportunistic infections [8]. A progressive decline in CD4^+^ T cell count is a hallmark of untreated HIV infection and is a key factor in the progression to acquired immunodeficiency syndrome (AIDS) [8].
Antiretroviral therapy (ART) suppresses HIV replication and restores CD4^+^ T cell count in PLWH [8]. Despite advancements in ART, the immune system of PLWH may not experience complete restoration and is characterized by residual inflammation and immune system dysregulation [9], culminating in a diminished response to immunization [10]. Seroconversion rates following vaccination for various diseases (e.g., pneumococcal disease, hepatitis B, measles, mumps, rubella [MMR], and yellow fever) in PLWH are lower compared to uninfected controls, and PLWH experience a more rapid decline in immunity [11,12,13,14,15]. Thus, the Centers for Disease Control and Prevention (CDC) developed vaccination guidelines specific to PLWH for a range of diseases, which include additional doses and more frequent boosters [16].
COVID-19 vaccination is effective in providing robust immunity against SARS-CoV-2, reducing severe illness in immunocompetent recipients [17,18,19,20,21,22]. COVID-19 vaccination has been reported to be just as effective in PLWH on ART with normal CD4^+^ T cell counts and a suppressed viral load, compared to uninfected controls, in countries outside of the US [23,24,25,26] and in small US samples [27]. However, other studies reported that PLWH present with a diminished immune response compared to uninfected controls [23], particularly in PLWH with lower CD4^+^ T cell counts [24], suggesting vaccine response varies based on immunosuppression level. However, COVID-19 vaccine trials included only small samples of virally suppressed PLWH on ART with normal CD4^+^ T cell counts [25], and did not consistently publish information on immunogenicity in PLWH [23,28]. Additionally, vaccine research, including COVID-19 vaccines, underrepresent racial/ethnic minorities, with most studies overrepresenting White non-Hispanic populations [23,25,26].
In addition to HIV, cardiometabolic comorbidities and substance abuse negatively impact immune function [29,30,31,32,33,34]. This suggests that PLWH and comorbidities may face a dual disadvantage, particularly in matters requiring carefully orchestrated immune functions, such as responding to vaccination. In fact, many comorbidities have already been associated with fewer neutralizing antibody titers against SARS-CoV-2 and poorer prognosis upon infection [35,36,37]. We aimed to investigate COVID-19 vaccine response in underserved, racial/ethnic minority PLWH by examining neutralizing antibody titers following two-dose SARS-CoV-2 vaccination and examining factors associated with SARS-CoV-2 immunogenicity, considering CD4^+^ T cell count, HIV viral load, comorbidities, and substance abuse.
2. Materials and Methods
2.1. Study Population
This cross-sectional study was conducted as part of the National Institutes of Health (NIH) Rapid Acceleration of Diagnostics-Underserved Populations (RADx-UP) initiative: a consortium of 144 projects studying COVID-19 testing patterns in underserved communities [38]. We analyzed data from an individual RADx-UP Phase I project site (3U01DA040381-05S1) located in an underserved urban sector of Miami, Florida; data for this analysis were collected between May 2021 and December 2021. Recruitment included participants in the Miami Adult Studies on HIV (MASH) cohort (U01DA040381) funded by the National Institutes on Drug Abuse (NIDA), which follows 1500 underserved Black and Hispanic adults living with and without HIV and high rates of comorbidities and substance use [39]. Detailed information about the methodology of this RADx-UP project site is provided elsewhere [40]. Briefly, the inclusion criteria for this RADx-UP project were being ≥18 years of age, and exclusion criteria included pregnancy. Eligible participants completed a survey that included validated measures of substance use, comorbidities, and health disparities, among other measures. At our research clinic, participants then underwent a blood draw and nasopharyngeal swab, which was tested for SARS-CoV-2 with real-time reverse transcription-polymerase chain reaction (rt-PCR). For this analysis, we included RADx-UP participants with complete data on HIV serostatus, COVID-19 vaccination, and SAR-CoV-2 antibodies. For the main analysis, since the sample size of participants who received only one dose of a COVID-19 vaccine was small (n = 33), we included PLWH who received two doses of a COVID-19 vaccine and excluded PLWH who received mixed vaccines (n = 6), PLWH who received two doses of the Ad26.COV2.S or BIBP-CorV inactivated COVID-19 vaccine (n = 4) [41,42], PLWH who underwent serology collection less than 14 days or more than 180 days after the second COVID-19 vaccine dose (n = 47) [43,44], nucleocapsid IgG seropositive cases (IgG ≥ 20 U/mL; indicates a prior natural SARS-CoV-2 infection; n = 22) [23,24], and those missing CD4^+^ T cell count or HIV viral load data (n = 22) (Supplementary Figure S1). The protocol for this study was approved by the Institutional Review Board at Florida International University; all participants provided informed consent to participate and to the release of their medical records.
2.2. Exposures: HIV Serostatus and COVID-19 Vaccination Status
HIV serostatus, HIV viral load, CD4^+^ T cell counts, ART, and COVID-19 vaccination information, including vaccination doses, dates, and brands, were abstracted from medical records.
2.3. Outcomes: SARS-CoV-2 Antibodies
Participants underwent a blood draw at our clinic; samples were drawn by a trained phlebotomist or registered nurse. Serum was isolated from whole blood via centrifugation. Two commercial assays were then used to test the serum samples for (1) SARS-CoV-2 nucleocapsid immunoglobulin G (IgG) to assess prior natural infection and (2) spike (trimer) total IgG/IgM/IgA (total Ig) to assess immune response to COVID-19 vaccination. The EDI™ COVID-19 Nucleocapsid IgG Quantitative ELISA Kit (Epitope Diagnostics, Inc., San Diego, CA, USA, Cat. # KTR-1034) was used to quantify the full-length SARS-CoV-2 nucleocapsid IgG. The Human SARS-CoV-2 Spike (trimer) Ig Total ELISA Kit (Invitrogen, Inc., Waltham, MA, USA, Cat. # BMS2323) was used to quantify spike (trimer) total IgG/IgM/IgA (total Ig).
2.4. Covariates: Sociodemographic Characteristics, Substance Use, and Comorbidities
Sociodemographic characteristics, including sex assigned at birth and race/ethnicity, were self-reported via standardized measures from RADx-UP common data elements (CDEs), which included items from the NIH CDE Repository, Disaster Research Response guidelines, and the PhenX Toolkit [45]. Age was confirmed via government-issued identification. Substance use, including tobacco (past 30 days), drug (past 12 months), and alcohol use (typical drinking habits), was determined via RADx-UP CDEs, which utilized the PhenX Toolkit [45]. Drug use included marijuana, cocaine/crack, heroin, fentanyl, methamphetamines, hallucinogens, ecstasy, or misuse of prescription drugs. For participants simultaneously enrolled in the MASH cohort, marijuana, cocaine, opioids, methamphetamine, amphetamine, and fentanyl use were verified via urine toxicology. Herein, drug use is defined as the use of marijuana, cocaine/crack, heroin, fentanyl, methamphetamines, amphetamines, hallucinogens, or ecstasy, or the misuse of prescription drugs, while substance use denotes the use of alcohol, tobacco, and/or drugs. Hazardous alcohol use was defined as >14 drinks/week for men (or >4 drinks/occasion), >7 drinks/week for women (or >3 drinks/occasion), and >7 drinks/week for adults ≥65 years [46]. Chronic conditions were assessed with the Johns Hopkins University C4-Ward Module Five: Comorbidities and Care Engagement, and included hypertension, diabetes, autoimmune diseases, chronic kidney disease (CKD), and substance use disorders [47]. Height and weight were measured to obtain body mass index (BMI).
2.5. Statistical Analyses
Descriptive statistics are presented as counts (percent, %) for categorical variables and median (interquartile range) for continuous variables. For categorical variables, between-group differences were tested using the chi-square test; Fisher’s exact test was utilized in cases of small cell counts. Due to the non-normality of continuous variables, the Wilcoxon rank-sum test was used to assess between-group differences. Boxplots were also generated and examined to compare median values of spike (trimer) total Ig by CD4^+^ T cell count and HIV viral load category. The main exposures of interest were HIV serostatus, HIV viral load, CD4^+^ T cell count, and COVID-19 vaccination. The primary outcome was spike (trimer) total Ig (indicates immune response to COVID-19 vaccination). The main linear regression analysis consisted of PLWH who received two doses of a COVID-19 vaccine, further divided by CD4^+^ T cell counts: <200, ≥200–<500, and ≥500 cells/µL [24,28]. Box–Cox transformations of the continuous outcome variable (spike [trimer] total Ig) were performed to bring residuals closer to normal distributions [23,24]. We also explored different BMI cut-offs in an exploratory analysis to find a suitable cut-off value with a potential association with SARS-CoV-2 spike (trimer) total Ig titer in this unique sample for use as a covariate representing BMI in multivariable models. A reduced model was developed with forward and backward stepwise variable selection. Missing data were treated as missing at random (MAR) and excluded from primary multivariable linear regression analysis [48]. A supplementary sensitivity analysis in which we compared the findings from the overall dataset of PLWH who received two doses of a COVID-19 vaccine with the subset used in the regression model was also conducted to evaluate the assumption that the data were in fact, MAR. Results were considered statistically significant at two-tailed p < 0.05. All statistical analyses were performed with R version 4.0.3.
3. Results
The sample (n = 1317) had a median age of 57.8 years (50.7–63.4); 49.8% were male, 50% were Black, non-Hispanic, 29.6% were living with HIV, 66.2% received at least one dose of a COVID-19 vaccine, and 75.5% of vaccinated participants underwent serology collection 14–179 days after their second vaccination dose (Table 1). Most PLWH were on ART (93.3%), virally suppressed (viral load < 200 copies/mL; 71.3%), and had a median CD4^+^ T cell count > 500 cells. PLWH, compared to participants without HIV, were more likely to have received at least one dose of a COVID-19 vaccine (76.2% vs. 62.0%, p < 0.001), have a lower BMI (27.3 kg/m^2^ vs. 28.2 kg/m^2^, p = 0.004), present with substance use (77.2% vs. 42.9%, p < 0.001), and present with comorbidities (such as hypertension, diabetes, autoimmune disease, obesity, and/or CKD) (72.8% vs. 48.2%, p < 0.001).
Participants without HIV who had not received a COVID-19 vaccine, compared to vaccinated participants without HIV, were more likely to be younger (53.6 [41.5–60.5] vs. 59.5 [51.1–64.8], p < 0.001), Black, non-Hispanic (52.0% vs. 37.9%, p < 0.001), and use substances including marijuana (29.8% vs. 15.3%, p < 0.001), cocaine (10.2% vs. 4.5%, p < 0.001), and tobacco (42.3% vs. 28.1%, p < 0.001) (Table 1). Additionally, unvaccinated participants without HIV were more likely to have been diagnosed with a substance use disorder (9.4% vs. 4.7%, p = 0.005), but less likely to have been diagnosed with comorbidities including hypertension (33.5% vs. 43.7%, p = 0.002) and diabetes (12.8% vs. 21.4%, p = 0.001).
PLWH who had not received a COVID-19 vaccine, compared to vaccinated PLWH, were more likely to be Black, non-Hispanic (80.6% vs. 61.6%, p = 0.004), and to engage in hazardous drinking (26.7% vs. 14.5%, p = 0.006), marijuana use (31.2% vs. 26.6%, p = 0.004), and cocaine use (16.1% vs. 10.1%, p = 0.004) (Table 1). Additionally, unvaccinated PLWH were less likely to have been diagnosed with comorbidities including diabetes (14.0% vs. 24.6%, p = 0.045) and CKD (1.1% vs. 7.1%, p = 0.036). However, vaccinated PLWH, compared to unvaccinated PLWH, had a higher median CD4^+^ T cell count (577.5 [416.8–876.8] vs. 517.5 [244.5–722.0], p = 0.011) and were more likely to be virally suppressed (76.4% vs. 54.8%, p < 0.001).
COVID-19-vaccinated PLWH, compared to vaccinated participants without HIV, were more likely to be male (56.6% vs. 46.0%, p < 0.001), Black, non-Hispanic (61.6% vs. 37.9%, p < 0.001), have a lower BMI (27.4 [24.0–31.7] vs. 28.3 [25.0–32.9], p = 0.04), and use substances, including hazardous alcohol use (14.5% vs. 4.9%, p < 0.001), marijuana (26.6% vs. 15.3%, p < 0.001), cocaine (10.1% vs. 4.5%, p < 0.001), and tobacco (34.7% vs. 28.1%, p = 0.047) (Table 1). Vaccinated PLWH were also more likely to have been diagnosed with a substance use disorder (9.4% vs. 4.7%, p = 0.006) and comorbidities including hypertension (54.5% vs. 43.7%, p = 0.002) and CKD (7.1% vs. 2.3%, p < 0.001).
COVID-19-vaccinated PLWH, compared to vaccinated participants without HIV, were more likely to be SARS-CoV-2 nucleocapsid IgG seropositive (nucleocapsid IgG titer ≥ 20 U/m; 8.1% vs. 3.8%, p = 0.008), suggesting prior natural SARS-CoV-2 infection (Table 1). The median SARS-CoV-2 spike (trimer) total Ig titer of PLWH with a prior natural SARS-CoV-2 infection was significantly higher than that in non-exposed PLWH (14,115 [3314–30,704] kU/mL vs. 1740 [395–4590] kU/mL, p < 0.001), regardless of vaccination status (Figure 1).
Among COVID-19-vaccinated PLWH, 88.9% received two doses (Table 2). The SARS-CoV-2 spike (trimer) total Ig seropositive rate (Ig ≥ 1000 U/mL; indicates a strong humoral immune response to COVID-19 vaccination) was significantly lower in PLWH who had received only one dose of a COVID-19 vaccine, compared with PLWH who had received two doses (33.3% vs. 81.1%, p < 0.001).
After applying the exclusion criteria for the main analysis, the regression analysis consisted of 174 PLWH who received two doses of a COVID-19 vaccine (Supplementary Figure S1 and Table S1). SARS-CoV-2 spike (trimer) total Ig seropositive rates among PLWH who received two doses of a COVID-19 vaccine were 42.9% in those with CD4^+^ T cell counts < 200 cells/µL, 77.4% in those with ≥200–<500 cells/µL, and 86.0% in those with ≥500 cells/µL (p < 0.001). We also found that median SARS-CoV-2 spike (trimer) total Ig titers were lowest in PLWH with CD4^+^ T cell counts < 200 (p = 0.033; Figure 2) and in PLWH with HIV viral loads ≥200–<5000 (p < 0.001; Figure 3). There were no differences in SARS-CoV-2 spike (trimer) total Ig titer between obese and non-obese PLWH who received two doses of a COVID-19 vaccine when using the established cut-off of ≥30 kg/m^2^. However, those with a BMI < 27 kg/m^2^ presented with lower SARS-CoV-2 spike (trimer) total Ig titer than those with a BMI ≥ 27 kg/m^2^ (2186 vs. 3007, p = 0.057). The adjusted regression model showed that CD4^+^ T cell count (<200 vs. ≥500, β = −0.279, p = 0.018), HIV viral load (≥200–<5000 vs. <200, β = −0.35, p = 0.002), and days between second vaccination dose date and serology sample collection date (β = −0.003, p < 0.001) predicted Box–Cox-transformed SARS-CoV-2 spike (trimer) total Ig titers in PLWH who received two doses of a COVID-19 vaccine (Table 3). A reduced model containing variables associated (p ≤ 0.05) with SARS-CoV-2 spike (trimer) total Ig titers in univariate or multivariable regression confirmed that CD4^+^ T cell count (<200 vs. ≥500, β = −0.400, p = 0.033), HIV viral load (≥200–<5000 vs. <200, β = −0.275, p < 0.001), and days between second vaccination date and serology sample collection date (β = −0.003, p < 0.001) significantly predicted SARS-CoV-2 spike (trimer) total Ig titers in PLWH who received two doses of a COVID-19 vaccine (Table 4). A supplementary sensitivity analysis in which we compared the findings from the overall dataset of PLWH who received two doses of a COVID-19 vaccine (n = 264) with the subset used in the regression model (n = 174), was also conducted and we found that the results from the two analyses were consistent in terms of the direction and significance of key associations (Supplementary Table S2).
4. Discussion
Understanding immune response is essential for preparing for public health crises. COVID-19 vaccination effectively provides robust immunity against multiple SARS-CoV-2 variants and reduces severe illness, hospitalization, and mortality [17,18,19,20,21,22]. However, immunocompromised populations may have weaker immune responses to vaccination [24]. Investigations into the immunogenicity of various vaccines in PLWH have reported diminished immune responses [10,11,12,13,14,15,30,31]. At the same time, COVID-19 vaccination has been reported to be just as effective in PLWH on ART with normal CD4^+^ T cell counts and a suppressed viral load, compared to uninfected controls [23,24,25,26,27]. However, other studies have reported diminished responses to COVID-19 vaccination in PLWH with lower CD4^+^ T cell counts [24]. Additionally, vaccine response research, including COVID-19 vaccines, is lacking in racial/ethnic minorities such as Black and Hispanic communities [23,25,26]. This lack of consensus and the scarcity of research in minority populations led us to investigate the immunogenicity of SARS-CoV-2 vaccination in a cohort of underserved Black and Hispanic adults living with and without HIV and high rates of substance use and comorbidities [39], a demographic historically underrepresented in vaccine research [49]. We found that PLWH were more likely to have received a COVID-19 vaccine and present with substance use and comorbidities. Vaccinated PLWH had higher CD4^+^ T cell counts and were more likely to be virally suppressed. A lower CD4^+^ T cell count and higher HIV viral load were associated with lower spike (trimer) total Ig titers in vaccinated PLWH, indicating a diminished response to COVID-19 vaccination.
Compared to participants without HIV, PLWH were more likely to have received a COVID-19 vaccine and present with substance use and comorbidities. Our vaccination rate of 76.2% among PLWH exceeded the national average of 73% in December 2021 [50]. It is possible that PLWH in our cohort were more likely to receive a COVID-19 vaccine due to engagement in care and long-standing rapport with infectious disease care providers. Indeed, we previously reported that MASH cohort PLWH were more likely to engage in preventive measures and healthcare during the COVID-19 pandemic compared to uninfected peers [51].
Compared to COVID-19-vaccinated PLWH, unvaccinated PLWH were more likely to be Black non-Hispanic, and engage in hazardous drinking, marijuana use, and cocaine use, but less likely to have been diagnosed with comorbidities including diabetes and CKD. These findings concur with previous research that reported lower COVID-19 vaccine rates and greater vaccine hesitancy in Black non-Hispanic populations, likely due to socioeconomic disparities and other challenges [52,53,54]. We also previously reported on the relationship between substance use and lower odds of COVID-19 vaccination and greater vaccine hesitancy in the MASH and RADx-UP cohorts [40]. Our findings regarding unvaccinated PLWH being less likely to present with comorbidities concur with previous work reporting increased vaccine acceptance among those with a higher risk of severe outcomes [55]. Thus, PLWH with better health and fewer comorbidities may have not received a COVID-19 vaccine due to a lower perceived need or susceptibility.
CD4^+^ T cell counts are heavily influenced by ART initiation and adherence [56,57,58]. While we found similar ART prescription rates between COVID-19-vaccinated PLWH and unvaccinated PLWH, vaccinated PLWH had higher CD4^+^ T cell counts and were more likely to be virally suppressed. This suggests that vaccine acceptance may correlate with better ART adherence, despite the similar rates of ART prescription. Given that participants were recruited through HIV care settings, the lower viral suppression rates among unvaccinated PLWH, particularly those with fewer comorbidities and more substance use disorders, likely reflects poorer engagement with care and medication adherence, resulting in both suboptimal HIV control and lower vaccine uptake.
Among vaccinated PLWH, SARS-CoV-2 spike (trimer) total Ig seropositive rates increased along with CD4^+^ T cell count and were the highest among PLWH with ≥500 cells. A lower CD4^+^ T cell count and higher HIV viral load were associated with lower total SARS-CoV-2 spike (trimer) total Ig titers, indicating a diminished response to COVID-19 vaccination. A similar study conducted in 2021 reported significantly lower SARS-CoV-2 anti-spike antibody titers among PLWH with CD4^+^ T cell counts of <500 cells, and, notably, <200 cells, following two-dose COVID-19 vaccination [28]. Nault et al. also reported a significant relationship between CD4^+^ T cell count and anti-receptor-binding domain (RBD) IgG response, which was lowest in PLWH with CD4^+^ T cell counts < 250 cells [24]. Thus, our work confirms a positive association between CD4^+^ T cell count and COVID-19 vaccine immune response, but in a sample of Black and Hispanic adults, a population lacking in COVID-19 vaccine research [23,25,26]. Our findings are also novel in that in addition to lower CD4^+^ T cell count, we also demonstrated a relationship between higher HIV viral load and diminished COVID-19 vaccination response, which was not previously reported [59].
Our findings could be explained by the notion that CD4^+^ T cells, the target of HIV [24], play a crucial role in orchestrating immune response through coordinating and regulating B cells involved in antibody (Ig) production [24,60,61,62]. Although the improvements in and increased access to ART has made immune recovery possible, subtle defects in inflammation and immune function persist, which may impair vaccine response [24]. Thus, in the future, it may be recommended that vaccination strategies in PLWH be tailored to CD4^+^ T cell count, as the functionality of B cells, and consequently, antibody (Ig) production, relies on CD4^+^ T cells [63]. In PLWH with low CD4^+^ T cell counts, additional vaccination doses may be advised to produce antibody titers sufficient to promote long-lasting immunity. Indeed, the SARS-CoV-2 spike (trimer) total Ig seropositive rate was significantly lower in PLWH who had received only one dose of a COVID-19 vaccine compared with PLWH who had received two doses, reinforcing CDC guidelines that include additional doses and more frequent boosters [16,26].
This work is strengthened by the use of a large sample of underserved minority adults from Miami, Florida, which experiences a high level of social vulnerability [64], the inclusion of similar proportions of men and women living with and without HIV and COVID-19 vaccination, the representation of Black and Hispanic adults, a population historically underrepresented in vaccine research [23,25,26,49], and the adequate distribution of CD4^+^ T cell counts ranging from <200 to >500, allowing for proper stratification and regression analyses. We also conducted a sensitivity analysis in which we compared the findings from the overall dataset of PLWH who received two doses of a COVID-19 vaccine (n = 264) with the subset used in the regression model (n = 174) and found that the results from the two analyses were consistent in terms of the direction and significance of key associations. Limitations include the cross-sectional design, there being no information on nadir CD4^+^ T cell counts, and the fact that a comparison between different types of COVID-19 vaccines was not performed due to the small sample size of participants who did not receive the mRNA-1273 or BNT162b2 mRNA COVID-19 vaccines. Additionally, because data were collected during a time when CDC COVID-19 vaccination guidelines were changing rapidly, complete booster and additional dose data were not yet available. The majority of the cohort, both PLWH and HIV-uninfected participants, received a COVID-19 vaccine, which limits our ability to draw conclusions regarding unvaccinated participants. Further, although we excluded nucleocapsid IgG seropositive cases from regression analysis to rule out prior natural infection, the half-life of nucleocapsid antibodies is relatively short [65]. Thus, it is possible some cases of prior natural SARS-CoV-2 infection were not identified. Finally, the final reduced model had an adjusted R^2^ = 0.156, which suggests modest explanatory power. However, we emphasize that our primary goal was to identify statistically significant associations rather than to maximize the explained variance. Considering this, we caution readers to consider these aspects when interpreting the scope and generalizability of our conclusions.
In conclusion, PLWH were more likely to receive a COVID-19 vaccine, and vaccinated PLWH had higher CD4^+^ T cell counts and were more likely to be virally suppressed. A lower CD4^+^ T cell count and higher HIV viral load were associated with a lower SARS-CoV-2 spike (trimer) total Ig titers in COVID-19-vaccinated PLWH. Thus, we provide evidence of a relationship between lower CD4^+^ T cell count and higher HIV viremia with reduced SARS-CoV-2 immunogenicity in racial/ethnic minority men and women living with HIV. HIV care providers should target efforts to maintain viral suppression to optimize immune responses to COVID-19 vaccination and may consider booster doses or modified dosing in PLWH [24], depending on immunosuppression level.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dong Y. Li Z. Ding S. Liu S. Tang Z. Jia L. Liu J. Liu Y. HIV infection and risk of COVID-19 mortality: A meta-analysis Medicine 2021100 e 2657310.1097/MD.000000000002657334190201 PMC 8257842 · doi ↗ · pubmed ↗
- 2Hoffmann C. Casado J.L. Härter G. Vizcarra P. Moreno A. Cattaneo D. Meraviglia P. Spinner C.D. Schabaz F. Grunwald S. Immune deficiency is a risk factor for severe COVID-19 in people living with HIVHIV Med.20212237237810.1111/hiv.1303733368966 · doi ↗ · pubmed ↗
- 3Ssentongo P. Heilbrunn E.S. Ssentongo A.E. Advani S. Chinchilli V.M. Nunez J.J. Du P. Epidemiology and outcomes of COVID-19 in HIV-infected individuals: A systematic review and meta-analysis Sci. Rep.202111628310.1038/s 41598-021-85359-333737527 PMC 7973415 · doi ↗ · pubmed ↗
- 4Guo W. Ming F. Dong Y. Zhang Q. Liu L. Gao M. Zhang X. Mo P. Feng Y. Tang W. Driving Force of COVID-19 Among People Living with HIV/AIDS in Wuhan, China Res. Sq.2020341364137110.21203/rs.3.rs-53351/v 135319336 · doi ↗ · pubmed ↗
- 5Goodnow C.C. Vinuesa C.G. Randall K.L. Mackay F. Brink R. Control systems and decision making for antibody production Nat. Immunol.20101168168810.1038/ni.190020644574 · doi ↗ · pubmed ↗
- 6Uhl L.F.K. Gérard A. Modes of Communication Between T Cells and Relevance for Immune Responses Int. J. Mol. Sci.202021267410.3390/ijms 2108267432290500 PMC 7215318 · doi ↗ · pubmed ↗
- 7Fenwick C. Joo V. Jacquier P. Noto A. Banga R. Perreau M. Pantaleo G. T-cell exhaustion in HIV infection Immunol. Rev.201929214916310.1111/imr.1282331883174 PMC 7003858 · doi ↗ · pubmed ↗
- 8Le Hingrat Q. Sereti I. Landay A.L. Pandrea I. Apetrei C. The Hitchhiker Guide to CD 4+ T-Cell Depletion in Lentiviral Infection. A Critical Review of the Dynamics of the CD 4+ T Cells in SIV and HIV Infection Front. Immunol.20211269567410.3389/fimmu.2021.69567434367156 PMC 8336601 · doi ↗ · pubmed ↗