Characterization of Load Components in Resistance Training Programs for Kidney Transplant Recipients: A Scoping Review
Jhonatan C. Peña, Lilibeth Sánchez-Guette, Camilo Lombo, Edith Pinto, Carlos Collazos, Blanca Tovar, Diego A. Bonilla, Luis A. Cardozo, Luis Andres Tellez

TL;DR
This review examines how resistance training is prescribed for kidney transplant recipients, finding significant variation in training parameters and no clear consensus.
Contribution
The study provides a comprehensive characterization of resistance training load components for kidney transplant recipients.
Findings
Most studies used %1RM for intensity control, with training zones between 30% and 80%.
Resistance training programs showed high heterogeneity in load periodization parameters.
Dumbbells, body weight, and elastic bands were the most commonly used resistance types.
Abstract
Resistance training (RT) has been shown to produce beneficial effects, including on quality of life, renal function, physical fitness, and survival rates in kidney transplant for 24 recipients. However, the optimal periodization of load components for this population remains unclear, as no consensus has been established. This study aimed to characterize the load components of RT programs in kidney transplant recipients. A scoping review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR). The literature search was performed up to October 2024 in MEDLINE/PubMed, the Web of Science Core Collection, SCOPUS, ScienceDirect, and SPORTDiscus. Only studies that included RT as part of the intervention were considered. The RT variables analyzed included intervention duration, weekly frequency, session duration,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
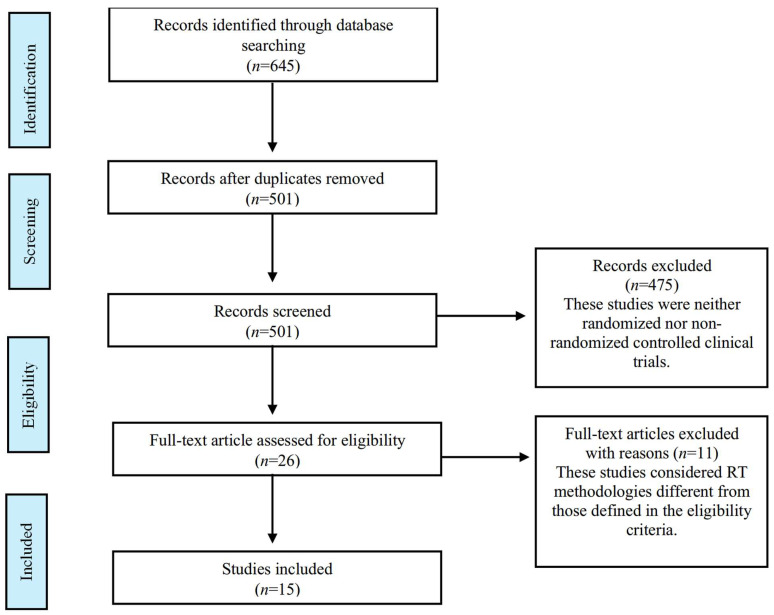 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7 Figure 8
Figure 8 Figure 9
Figure 9 Figure 10
Figure 10Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDialysis and Renal Disease Management · Cardiovascular and exercise physiology · Hemodynamic Monitoring and Therapy
1. Introduction
Kidney transplantation is the most effective strategy for treating individuals with end-stage renal disease, providing multiple benefits such as improved quality of life and increased survival rates [1,2]. However, as part of their post-surgical treatment, these patients receive immunosuppressive medications, which weaken the immune system and increase the risk of metabolic disturbances associated with the recurrence of non-communicable diseases [3,4,5]. Given this issue, it is essential for these individuals to adopt healthy lifestyle habits that counteract the adverse effects of these medications and contribute to better immune system function [6,7,8]. In this regard, previous research has established that obesity, metabolic syndrome development, physical inactivity, and poor dietary habits are among the risk factors associated with premature mortality, cardiac events, and graft loss [9,10].
One of the most effective strategies for improving specific health outcomes in this population, while simultaneously reducing the risk of metabolic diseases, is the incorporation of physical exercise into their daily routines [11,12,13,14,15]. A recent meta-analysis, including a total of sixteen randomized clinical trials with 827 patients, demonstrated that supervised physical exercise resulted in favorable changes in cardiorespiratory capacity, physical fitness, creatinine levels, quality of life, and high-density lipoprotein cholesterol (HDL-c) values [16]. However, the findings of this study suggest that due to variability in interventions, it is not possible to conclude which exercise modality is the most effective. It was only established that most successful studies proposed a frequency of three sessions per week, with a duration of 30 to 60 min per session, over a period of three to six months. Furthermore, it is suggested that the cardiorespiratory component should be programmed at 60% to 70% of maximum heart rate, while strength training should be performed twice a week [16]. Additionally, a recent clinical practice guideline on lifestyle in renal disease, specifically in transplant recipients, indicates that engaging in physical exercise improves survival rates in these patients [17]. However, regarding load periodization parameters, the guideline only generally mentions the importance of combining resistance and endurance training, without delving into specific components such as intensity, volume, recovery times, density, and execution velocity.
In the last decade, there has been a paradigm shift in how resistance training (RT) is programmed and dosed [18]. In this regard, various studies have aimed to standardize the correct methodology for periodizing all load components [19,20]. RT has been widely used as an intervention strategy for kidney transplant recipients, demonstrating positive effects on health. However, there is considerable heterogeneity in how these exercise programs are prescribed, making it difficult to establish an optimal model for load periodization and progression. Currently, no specific guidelines provide clear recommendations for structuring strength training programs in this population, posing a challenge for exercise professionals. Given the need for evidence-based guidelines to support the programming of strength training for kidney transplant recipients, this exploratory review aims to characterize the load components used in these training programs. By identifying patterns in exercise prescription and detecting gaps in the literature, this study seeks to provide valuable insights that can contribute to the development of more precise recommendations for professional practice.
2. Materials and Methods
2.1. Protocol and Registration
A scoping review was conducted following the reporting Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) [21]. The review protocol was registered on Open Science Framework https://osf.io/2bh9z/ (accessed on 2 May 2024)-The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist is presented in Supplementary Table S1.
2.2. Eligibility Criteria
This review included primary studies with clinical trial designs (randomized or non-randomized controlled studies) that evaluated the effect of RT programs, either supervised or unsupervised on any type of outcomes in kidney transplant recipients. RT programs featuring free weights (i.e., with or without external overload [weights, elastic band]) and machines were considered. Study interventions with other types of methodologies such as endurance training (in treadmill or bicycle and multi-component) were not included in the scope of this review.
2.3. Information Sources
The search for studies was carried out in the following databases: MEDLINE/PubMed, the Web of Science Core Collection, SCOPUS, Science Direct, and SPORTDiscus. The reference lists of the selected articles were also manually searched for additional literature (snowballing).
2.4. Search Strategy
The population, concept, and context (PCC) mnemonic was utilized for structuring our research question [22]: P (kidney transplant recipients), C (RT protocols), and C (detailed RT variables according to the National Strength and Conditioning Association [NSCA] recommendations: training methodology, exercise selection, sets, repetitions, intensity, load progression, rest interval between sets, execution velocity, weekly frequency, and duration of RT intervention [23,24,25]). The search strategy was composed of the keywords: (“resistance training” OR “resistance exercise” OR “strength training” OR “strength exercise” OR “weight exercise” OR “weight training” OR “exercise training”) AND (“kidney transplantation” OR “renal transplantation” OR “kidney transplant recipients” OR “kidney grafting”). The search strategy for each specific base is presented in Supplementary Table S2. The searches were carried out without applying restrictions by year of publications, but only articles written in the English language were included. Before submitting the manuscript, an updated bibliographic search was conducted to incorporate the most recent and relevant studies. As a result of this update, two additional studies were included in the analysis.
2.5. Method for Evidence Source Selection
Two research carried out the searches in the proposed databases and the identified studies were imported into EndNote^TM^ Basic to remove the duplicates. Subsequently, the authors (JP and CL) reviewed the full text to determine the inclusion of the study according to the eligibility criteria. A third reviewer (LC) analyzed disagreements and determined which studies were included in the review.
2.6. Data Charting Process and Items
The selected studies were analyzed independently by each researcher, extracting the following information in an Excel rubric. In studies reporting combined exercises (concurrent training), only the RT information was extracted:
- General information of the study: year of publication, design, sample size, age, sex and post-transplant time of the participants.
- Characteristics of the RT program: training methodology, exercise selection, sets, repetitions, intensity, load progression, rest interval between sets, execution velocity, weekly frequency, and duration.
2.7. Data Extraction and Analysis Process
A qualitative descriptive analysis of the training programs was carried out. The researchers extracted the information presented in each manuscript in the methodology sections. In cases where one of the proposed characteristics was not clearly specified in the text, it was recorded as “not reported”. At the end of this process, cross-checking of all the information retrieved was carried out. A third review by an experienced proofreader resolved the divergences.
3. Results
3.1. Selection of Sources of Evidence
Initially, 645 studies were identified. After removing duplicates, 501 titles and abstracts were screened, resulting in 26 potentially eligible full texts. A total of 15 studies were included in this review. Figure 1 presents the PRISMA flow diagram of this study.
3.2. Characteristics of Sources of Evidence
Table 1 shows the characteristics of the selected studies. A total of 666 participants were included across all studies, with both men and women taking part in the 15 interventions [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40]. The age of the experimental groups ranged from 27 to 56 years. The post-transplant time before initiating the physical exercise program was reported in only five studies with a mean of 57.6 months.
3.3. Synthesis of Results
Table 2 summarizes the exercise prescription details. Three studies focused on RT [27,32,38], two compared endurance and RT [34,37], and the remaining implemented concurrent training [26,28,29,30,31,33,35,36,39,40]. Training frequency ranged from three to five sessions per week, the intervention duration ranged from 2.5 to 12 months, and session length ranged from 30 to 90 min. Six studies used light dumbbells, body weight, and elastic bands [28,29,30,31,33,35], while four included machine-based exercises [27,37,38,40]. Four studies did not specify the exercise type [26,32,34,36]. The number of exercises per session ranged from 5 to 12.
Table 3 details the periodization characteristics. Intensity was primarily controlled using a percentage of one-repetition maximum (1RM) [26,32,35,36,37,38,40]. Other methods included OMNI scale [30], maximum heart rate (MHR) [28], and maximum repetitions [27]. Sets ranged from two to eight, repetitions from 10 to 20, and rest intervals from 1 to 5 min. Load progression was based on intensity, volume, or exercise complexity. Execution velocity was reported in one study [30] using self-perception.
4. Discussion
This review provides a comprehensive analysis of the characterization of load components in RT programs for kidney transplant recipients. Based on the analysis of thirteen studies, certain trends were identified; however, one of the main findings of this review was the high variability in exercise prescription and the lack of standardized criteria for load dosing.
Regarding the type of training, most of the reviewed studies suggest a concurrent training methodology [26,28,29,30,31,33,35,36,39,40]. This approach integrates RT as a fundamental component of the training session while complementing it with cardiorespiratory exercises. In fact, evidence from other populations indicates that concurrent training does not impair muscle hypertrophy or maximal strength development [41]. However, gains in explosive strength may be attenuated, particularly when cardiorespiratory exercise and RT are performed within the same session [42]. Moreover, concurrent training appears to be an effective exercise methodology for enhancing motivation and adherence, particularly among sedentary individuals with no prior experience in structured training programs [43,44,45]. This could explain its frequent implementation in the transplant population.
Load intensity is a critical variable in RT load dosing across different populations [46,47,48,49]. Among the studies included in this review, six used %1RM to control this variable [26,32,35,36,37,38,40], making it the most commonly employed indicator. However, the reported training intensities ranged from 30% to 80% of 1RM, highlighting a lack of conceptual clarity regarding the optimal intensity range for kidney transplant recipients.
Regarding volume, the number of exercises per session ranged from five to eight, the number of sets varied between two and eight, and repetitions ranged from 10 to 20. Similarly to intensity, these broad ranges reflect the absence of conclusive scientific evidence establishing precise training volumes to induce specific chronic adaptations, as has been determined for other populations [50,51]. Similarly, it was observed that rest intervals between sets is a fundamental variable for specific adaptations such as hypertrophy development [52] were not reported in nine of the reviewed studies [26,28,29,32,33,34,35,36,39]. This suggests that the importance of this variable has been overlooked when designing training protocols for transplant populations.
Among the load components, execution velocity has received the least attention in this population, with only one study reporting its use [30]. In contrast, research in other populations (i.e., older adults) has demonstrated that high-speed resistance training is effective for improving overall health outcomes [53]. It is worth mentioning that movement velocity is an accurate approach for prescribing RT, offering multiple advantages such as controlling intensity from the first repetition of a set [54,55,56] and regulating volume based on velocity loss [20,57]. Controlling this variable eliminates many of the inconsistencies associated with traditional RT methods of RT [18]. If a linear position transducer is not available, perceived exertion and movement velocity scales serve as valid, economical, and practical tools for assessing RT load progression and complementing other training monitoring variables, although familiarization remains key [58].
Regarding exercise selection, six of the reviewed studies recommended the use of light dumbbells, body weight exercises, and elastic bands [28,29,30,31,33,34]. A possible rationale for this recommendation is the ease of execution, particularly for individuals with limited RT experience, a common characteristic in this population.
One of the main limitations of this study is that only 15 out of the 501 initially identified studies were included. While the strict eligibility criteria ensured the quality of the analyzed studies, they may have excluded some training programs developed for this population. It is important to note that the scope of this review was limited to the load components of strength training programs; the effects of these interventions on the outcome variables assessed in each study were not analyzed. Additionally, certain strength training methodologies, such as suspension exercises, were not considered.
Considering the absence of standardized criteria for periodizing load components in kidney transplant recipients, Table 4 summarizes the most frequently reported elements in the reviewed studies. These elements can serve as a foundation for exercise professionals in designing training programs for this population.
Future Directions
One of the most significant insights derived from this review is the recognition that, while a substantial body of scientific evidence supports the beneficial effects of structured exercise programs on various health outcomes, notable methodological limitations continue to persist within the design and implementation of these training protocols. These shortcomings highlight the need for a more rigorous and standardized approach to exercise prescription, particularly in clinical populations where individualized interventions are crucial. In this regard, fostering interdisciplinary collaboration among nephrologists, sports medicine physicians, and exercise professionals presents a promising avenue for addressing these challenges. By integrating their respective expertise, these specialists could contribute to the development of more precise, evidence-based, and systematically structured training regimens tailored to the specific physiological and medical needs of patients. Such an approach would not only enhance the efficacy of exercise interventions, but also ensure their safety and long-term adherence.
The heterogeneity of the implemented programs hinders the establishment of specific and detailed parameters for load prescription. However, the common elements identified can serve as a foundation for exercise professionals to design more structured and effective training plans. Future research should focus on developing more rigorous protocols supported by robust methodological frameworks that include well-defined exercise parameters, appropriate control conditions, and standardized outcome measures. Additionally, it is essential to determine the optimal exercise modalities, intensities, and durations that maximize therapeutic benefits in patients with various health conditions. Strengthening the scientific foundation in this field will facilitate the integration of structured exercise as a fundamental component of clinical care, enhancing both the effectiveness of interventions and the overall health and well-being of patients.
5. Conclusions
This scoping review described the general characteristics of the load components in RT programs for kidney transplant recipients. The findings highlight a lack of standardized criteria in the prescription of fundamental periodization variables; however, several recommendations based on available evidence are given regarding intensity, volume, and load progression. Additionally, movement velocity remains an overlooked component in the design of strength training programs for this population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rahimzadeh N. Otukesh H. Seirafianpour F. Hoseini R. Long-Term Outcome of Kidney Transplant Among Iranian Children: A Systematic Review and Meta-Analysis Exp. Clin. Transplant.20222089590010.6002/ect.2020.027433928879 · doi ↗ · pubmed ↗
- 2Burns T. Fernandez R. Stephens M. The experiences of adults who are on dialysis and waiting for a renal transplant from a deceased donor: A systematic review JBI Evid. Synth.20151316921110.11124/jbisrir-2015-197326447040 · doi ↗ · pubmed ↗
- 3Keyzer C.A. Vermeer C. Joosten M.M. Knapen M.H. Drummen N.E. Navis G. Bakker S.J. de Borst M.H. Vitamin K status and mortality after kidney transplantation: A cohort study Am. J. Kidney Dis.20156547448310.1053/j.ajkd.2014.09.01425453995 · doi ↗ · pubmed ↗
- 4Jansz T.T. Neradova A. van Ballegooijen A.J. Verhaar M.C. Vervloet M.G. Schurgers L.J. van Jaarsveld B.C. The role of kidney transplantation and phosphate binder use in vitamin K status P Lo S ONE 201813 e 020315710.1371/journal.pone.020315730161193 PMC 6117040 · doi ↗ · pubmed ↗
- 5Haasova M. Snowsill T. Jones-Hughes T. Crathorne L. Cooper C. Varley-Campbell J. Mujica-Mota R. Coelho H. Huxley N. Lowe J. Immunosuppressive therapy for kidney transplantation in children and adolescents: Systematic review and economic evaluation Health Technol. Assess.201620132410.3310/hta 20610 PMC 500290027557331 · doi ↗ · pubmed ↗
- 6Sgambat K. Clauss S. Lei K.Y. Song J. Rahaman S.O. Lasota M. Moudgil A. Effects of obesity and metabolic syndrome on cardiovascular outcomes in pediatric kidney transplant recipients: A longitudinal study Pediatr. Nephrol.2018331419142810.1007/s 00467-017-3860-829290033 · doi ↗ · pubmed ↗
- 7Sgambat K. Clauss S. Moudgil A. Comparison of BMI, waist circumference, and waist-to-height ratio for identification of subclinical cardiovascular risk in pediatric kidney transplant recipients Pediatr. Transplant.201822 e 1330010.1111/petr.1330030294896 · doi ↗ · pubmed ↗
- 8Nguyen T.H. Mat Daud Z.A. Abd Talib R. Mohd R. Poh B.K. Metabolic Syndrome and Dietary Intake are Associated With Quality of Life in Kidney Transplant Recipients Transplant. Proc.2023552176218210.1016/j.transproceed.2023.08.00837743189 · doi ↗ · pubmed ↗