Impact of Institutional Monthly Volume of Transcatheter Edge-to-Edge Repair Procedures for Significant Mitral Regurgitation: Evidence from the GIOTTO-VAT Study
Nicola Corcione, Paolo Ferraro, Filippo Finizio, Michele Cimmino, Michele Albanese, Alberto Morello, Giuseppe Biondi-Zoccai, Paolo Denti, Antonio Popolo Rubbio, Francesco Bedogni, Antonio L. Bartorelli, Annalisa Mongiardo, Salvatore Giordano, Francesco De Felice, Marianna Adamo

TL;DR
This study finds that higher institutional volume of a heart procedure called TEER is linked to better outcomes, including higher success rates and shorter hospital stays.
Contribution
The study provides evidence that institutional monthly procedural volume impacts clinical outcomes in TEER for mitral regurgitation.
Findings
Procedural success rates and shorter hospital stays were observed in higher-volume centers.
Long-term cardiac death or hospitalization for heart failure was less common in the busiest centers.
Baseline risk profiles varied between low- and high-volume centers.
Abstract
Background and Objectives: Mitral valve transcatheter edge-to-edge repair (TEER) is a widely adopted therapeutic approach for managing significant mitral regurgitation (MR) in high-risk surgical candidates. While procedural safety and efficacy have been demonstrated, the impact of institutional expertise on outcomes remains unclear. We aimed at evaluating whether the institutional monthly volume of TEER influences short- and long-term clinical results. Materials and Methods: This analysis from the multicenter, prospective GIOTTO trial study evaluated the impact of institutional monthly volume on outcomes of TEER to remedy significant mitral regurgitation. Centers were stratified into tertiles based on monthly volumes (≤2.0 cases/month, 2.1–3.5 cases/month, >3.5 cases/month), and key clinical, echocardiographic, and procedural outcomes were analyzed. Statistical analysis was based on…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
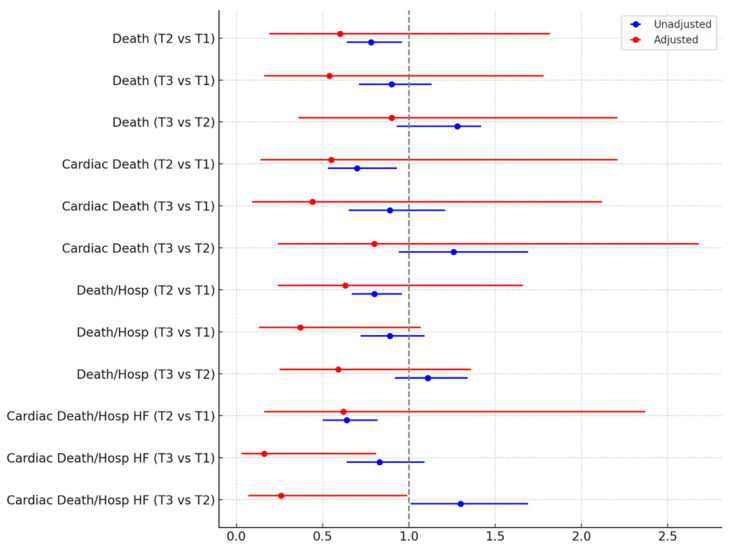 Figure 1
Figure 1- —Italian Society of Invasive Cardiology, with an unrestricted grant by Abbott Vascular, Santa Clara, CA, USA
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiac Imaging and Diagnostics · Infective Endocarditis Diagnosis and Management
1. Introduction
Transcatheter edge-to-edge repair (TEER) has emerged as an effective alternative to surgical valve repair in high-risk patients, and to conservative medical therapy only in carefully selected individuals considered unfit for surgery [1,2]. Indeed, given its ability to improve functional outcomes and reduce heart failure hospitalizations, TEER is increasingly performed worldwide [3]. However, the early and long-term effectiveness of TEER is impacted by several factors, ranging from patient to anatomic and procedural ones [4,5,6,7,8,9,10,11].
On top of patient, procedural, and operator features, institutional characteristics have been the focus of attentive recommendations and analysis [12]. Indeed, in most settings, TEER is only provided as long as surgical mitral valve repair/replacement is also available. Yet, this minimum requirement might be too lenient because expertise in patient screening and selection, procedural efficiency, and seamless quality of care are paramount to achieve optimal outcomes with TEER [13]. In particular, a number of cutoffs have been proposed and tested formally in the past, under the key premise that higher-volume centers may provide better results, shortly after the procedure as well as subsequently. However, results have been inconsistent so far, with some studies suggesting that no evident cutoff can be envisioned, and others ending up recommending a minimum yearly volume ranging from 8 to 24 cases [14,15,16].
We hypothesized that the institutional monthly volume of TEER could influence short- and long-term clinical results of this technically demanding procedure, in the sense that institutions exhibiting higher monthly volumes could provide better outcomes in comparison to centers with a lower monthly caseload. We thus aimed at appraising the impact of the institutional monthly volume of TEER on early and long-term outcomes, and in order to test this hypothesis, we chose to leverage the extensive and detailed dataset of the ongoing prospective GIOTTO (GIse registry Of Transcatheter treatment of mitral valve regurgitaTiOn) registry, an Italian multicenter observational study including patients undergoing TEER with a MitraClip (Abbott Vascular, Santa Clara, CA, USA) [5]. Indeed, key strengths of GIOTTO include its contemporary stance and follow-up that goes well beyond discharge.
2. Methods
This study was based on the dataset accrued in the GIOTTO trial, which is sponsored by the Italian Society of Invasive Cardiology (GISE—Società Italiana di Cardiologia Interventistica, Milan, Italy) and is registered online at ClinicalTrials.gov (NCT03521921) [5]. Notably, ethical approval was obtained from all participating institutions, and all patients provided written informed consent.
For the purpose of this analysis, which we labelled GIOTTO-VAT (volume and time), we mainly focused on comparing tertiles of cases per month, center-wise, with the first tertile up to 2.0 cases per month, the second tertile with more than 2.0 and up to 3.5 cases per month, and the third tertile with more than 3.5 cases per month. Exploratory analyses were conducted according to tertiles of total volume, center-wise, with the first tertile up to 100 cases, the second tertile with more than 100 and up to 200 cases, and the third tertile with more than 200 cases, as well as distinguishing between the first 50 cases per center and the subsequent ones.
Details on baseline variables were collected, including demographic data, comorbidities, functional class, prior cardiac procedures, and medication history. Echocardiographic parameters being assessed included left atrial diameter, left ventricular dimensions, mitral valve gradient, and severity of tricuspid regurgitation. Procedural variables of interest included number and generation of MitraClip devices implanted, fluoroscopy time, device time, and procedural success. Fatal and non-fatal outcomes occurring during the index hospitalization and during follow-up were systematically collected, with specific attention to the following events: death, cardiac death, the composite of death or hospitalization, and the composite of death or hospitalization for heart failure.
Descriptive statistics were computed for all variables, with medians and first and third quartiles provided for continuous variables, and counts and percentages for categorical variables. Bivariate analysis was based on Kruskal–Wallis tests for continuous variables and Fisher exact tests for categorical variables. Censored outcomes were analyzed with Cox proportional hazard models, unadjusted as well as adjusted for potential confounders. Notably, the following potential confounders were forced into the adjusted models: age, gender, smoking history, dyslipidemia, degenerative etiology, baseline functional class, prior mitral valve repair, prior stroke, frailty, peripheral artery disease, surgical risk scores, left atrial diameters, left ventricular diameters, left ventricular volumes, tenting area, severe calcification, prolapse, severity of tricuspid regurgitation, concomitant ECG abnormalities, atrial fibrillation, and significant coronary artery disease. No missing data imputation was performed. Statistical significance was set at a 2-tailed p-value of 0.05, without multiplicity adjustments, and all analyses were conducted using Stata 18 (StataCorp, College Station, TX, USA).
3. Results
A total of 2213 patients were included, with 645 (29.1%) individuals treated in centers performing ≤ 2.0 cases/month, 947 (42.8%) treated in institutions reporting between 2.1 and 3.5 cases/month, and 621 (28.1%) patients treated in hospitals with >3.5 cases/month (Table 1). Several differences according to such stratifications were found in key baseline features, with some suggesting a higher complexity in patients treated in lower-volume centers, such as age, functional class, and surgical risk score (all p < 0.05), and others suggesting a higher risk in those treated in busier centers, such as smoking, dyslipidemia, prior mitral valve intervention, prior stroke, peripheral artery disease, and frailty score (all p < 0.05).
Other significant differences were found for left ventricular dimensions and function, and mitral valve tenting area (Table 2), disfavoring less busy centers (all p < 0.05), and for left atrial dimensions, mitral valve calcification, mitral valve prolapse, tricuspid regurgitation severity, concomitant ECG abnormalities, and prevalence of atrial fibrillation, disfavoring higher-volume institutions (all p < 0.05).
In terms of procedural details, significant differences were found in rates of implantation of multiple MitraClips, type of MitraClip used, device time, and fluoroscopy time (all p < 0.05; Table 3). Notably, device success rates were similar across tertiles, but procedural success was marginally albeit significantly higher in busier centers (p < 0.001), with concomitantly lower rates of severe residual mitral regurgitation (p = 0.001). Patients in high-volume centers experienced fewer in-hospital bleeding events (p = 0.006) but more vascular complications (p = 0.008), without significant differences in in-hospital mortality (p = 0.123). Length of hospital stay was significantly shorter in higher-volume centers (p < 0.001).
During a median follow-up of 14 months, details on a total of 539 (24.4%) deaths, 286 (12.9%) cardiac deaths, 685 (31.0%) deaths or hospitalizations, and 359 (16.2%) cardiac deaths or hospitalizations for heart failure were accrued (Table 4). Moderate or severe mitral regurgitation was reported overall in 308 (14.3%). Survival analysis was performed using first unadjusted models (Table 5), and these suggested worse outcomes in less busy centers for death, cardiac death, the composite of death or hospitalization, and the composite of cardiac death or hospitalization for heart failure (all p < 0.05). However, after taking into account potential confounders, all these differences were no longer significant, except for cardiac death or hospitalization for heart failure, which appeared significantly less common in the busiest centers (all p < 0.05; Figure 1).
Similar trends were observed when leveraging tertiles of overall center volume and when comparing for each center the first 50 cases with the following ones (Tables S1–S4), with higher procedural success rates in busier/more experienced centers, and similarly trends favoring them for long-term clinical outcomes.
4. Discussion
A high institutional monthly volume of TEER mitral valve repair appears to correlate with improved procedural success rate and shorter hospitalizations. Similarly favorable results were found for long-term rates of cardiac death or hospitalization for heart failure.
The evidence base appraising the impact of institutional volume and expertise on TEER outcomes is complex and heterogeneous, but some studies have indeed suggested that some thresholds are important to achieve satisfactory procedural, in-hospital, and mid-term outcomes (Table S5) [10,12,14,15,16,17]. The findings from the present GIOTTO-VAT study support the concept that institutional volume in TEER may significantly impact on clinical outcomes. Notably, centers with higher monthly case volumes demonstrated greater procedural success. Furthermore, similarly favorable results were evident for long-term outcomes at unadjusted and adjusted analysis. These results align with existing evidence in the field of structural heart interventions, where operator and institutional experience have been shown to positively impact clinical outcomes [10,11].
Interestingly, while higher-volume centers showed better procedural metrics, long-term clinical outcomes, including mortality, were comparable across tertiles. This suggests that while experience improves technical execution and immediate safety, patient selection and underlying clinical conditions remain key determinants of long-term prognosis. Moreover, the impact of experienced proctors affiliated with high-volume centers providing careful guidance to lower-volume institutions cannot be discounted, in person or remotely. Indeed, the impact of proctors should be carefully appraised in future studies, together with detailed analyses on post-procedural care and management protocols.
A notable finding was the reduced hospitalization duration in high-volume centers compared to lower-volume ones. This may reflect more efficient perioperative management, shorter procedural times, and faster post-operative recovery [18]. Shorter hospital stays can also reduce healthcare costs, which is a significant consideration in the growing adoption of TEER for mitral regurgitation management, thus reinforcing the call for established expertise in all phases of management of patients with significant mitral regurgitation [19].
Our results prove informatively complementary to those reported by Grayburn and colleagues, who analyzed the American College of Cardiology/Society of Thoracic Surgeons Transcatheter Valve Therapy Registry and the Society of Thoracic Surgeons Adult Cardiac Surgery Database comparing institutions with high volumes for mitral valve repair, including surgical interventions [20]. In this study of 41,834 patients, the TEER success rate was similar in low- vs. high-volume centers, but 1-year survival and freedom from heart failure readmission were better in higher-volume hospitals.
This study has several key limitations that should be carefully considered by readers. First, despite some clear hints that higher volumes over time are associated with better outcomes in patients undergoing TEER for significant mitral regurgitation, results were not altogether consistent [21]. In addition, even adjusted analyses cannot be considered devoid of risk of residual confounding, such as ethnic features, which were not collected in our study. This is a key drawback, as minorities often have a more difficult time in accessing high-volume centers [22]. Furthermore, the risk of duplicity and type I error inflation due to a plethora of statistical tests remains substantial, and thus external replication of the present findings is paramount [23].
5. Conclusions
The present GIOTTO-VAT study suggests that hospitals with a higher volume of cases over time may yield improved procedural success rates, with ensuing shorter hospitalizations. Long-term rates of cardiac death or hospitalization for heart failure also favored centers with higher case/month figures. These findings inform on the importance of operator experience and center expertise in achieving state-of-the-art results with TEER, while confirming the usefulness of the proctoring approach when naïve centers begin a TEER program.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Feldman T. Foster E. Glower D.D. Kar S. Rinaldi M.J. Fail P.S. Smalling R.W. Siegel R. Rose G.A. Engeron E. Percutaneous repair or surgery for mitral regurgitation N. Engl. J. Med.20113641395140610.1056/NEJ Moa 100935521463154 · doi ↗ · pubmed ↗
- 2Stone G.W. Lindenfeld J. Abraham W.T. Kar S. Lim D.S. Mishell J.M. Whisenant B. Grayburn P.A. Rinaldi M. Kapadia S.R. Transcatheter Mitral-Valve Repair in Patients with Heart Failure N. Engl. J. Med.20183792307231810.1056/NEJ Moa 180664030280640 · doi ↗ · pubmed ↗
- 3Zhou S. Egorova N. Moskowitz G. Giustino G. Ailawadi G. Acker M.A. Gillinov M. Moskowitz A. Gelijns A. Trends in Mitra Clip, mitral valve repair, and mitral valve replacement from 2000 to 2016 J. Thorac. Cardiovasc. Surg.2021162551562.e 410.1016/j.jtcvs.2019.12.09732089343 PMC 7957952 · doi ↗ · pubmed ↗
- 4Shi W. Zhang W. Zhang D. Ye G. Ding C. Mortality and Clinical Predictors After Percutaneous Mitral Valve Repair for Secondary Mitral Regurgitation: A Systematic Review and Meta-Regression Analysis Front. Cardiovasc. Med.2022991871210.3389/fcvm.2022.91871235859589 PMC 9289259 · doi ↗ · pubmed ↗
- 5Giordano A. Biondi-Zoccai G. Finizio F. Ferraro P. Denti P. Rubbio A.P. Petronio A.S. Bartorelli A.L. Mongiardo A. De Felice F. Characteristics and outcomes of Mitra Clip in octogenarians: Evidence from 1853 patients in the GIOTTO registry Int. J. Cardiol.2021342657110.1016/j.ijcard.2021.08.01034375704 · doi ↗ · pubmed ↗
- 6van-Roessel A.M. Asmarats L. Li C.H.P. Millán X. Fernández-Peregrina E. Menduiña I. Sanchez-Ceña J. Arzamendi D. Mitral transcatheter edge-to-edge repair: Patient selection, current devices, and clinical outcomes Expert. Rev. Med. Devices 20242118719610.1080/17434440.2023.229871338155555 · doi ↗ · pubmed ↗
- 7Sonaglioni A. Nicolosi G.L. Bruno A. Lombardo M. Muti P. Echocardiographic Assessment of Mitral Valve Prolapse Prevalence before and after the Year 1999: A Systematic Review J. Clin. Med.202413616010.3390/jcm 1320616039458110 PMC 11508471 · doi ↗ · pubmed ↗
- 8Stolz L. Stocker T.J. Lurz P. Hausleiter J. Growing Evidence for Edge-to-Edge Repair in Secondary Mitral Regurgitation: What to Learn From COAPT, MITRA-FR, and RESHAPE-HF 2JACC Cardiovasc. Interv.20251892793210.1016/j.jcin.2025.01.42940240087 · doi ↗ · pubmed ↗