Analysis of Neurosensory Changes in Orthognathic Surgery Using Saw or Piezoelectric Devices: A Scoping Review
Ailyn Navarrete, Víctor Ravelo, Leonardo Brito, Erick Vargas, Márcio de Moraes, Sergio Olate

TL;DR
This review compares neurosensory recovery after orthognathic surgery using a reciprocating saw or a piezoelectric device, finding better outcomes with the latter.
Contribution
The study provides a comparative analysis of neurosensory outcomes between two surgical tools in orthognathic procedures.
Findings
Three studies found piezoelectric surgery correlates with better neurosensory recovery and faster postoperative healing.
Two studies reported no significant difference in sensitivity recovery between the two devices.
Overall, piezoelectric systems typically show better postoperative recovery of sensitivity compared to traditional saws.
Abstract
Orthognathic surgery is a successful surgical method for correcting facial deformities, and the piezoelectric system can be used in place of or in addition to traditional tools like the reciprocating saw to perform osteotomies. This study assesses how using a reciprocating saw or a piezoelectric device exclusively affects neurosensory impairment. A review was performed following the PRISMA-ScR recommendations. A search was conducted until December 2024 in PubMed, Embase, and Web of Science. Clinical trials and quasi-experimental studies in English and Spanish were included. A total of nine articles were obtained for full-text review using inclusion and exclusion criteria. The selected articles included a total of 731 subjects. The age range of the studies included was between 18 and 49 years. Three of the six analyzed state that piezoelectric surgery positively correlates with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
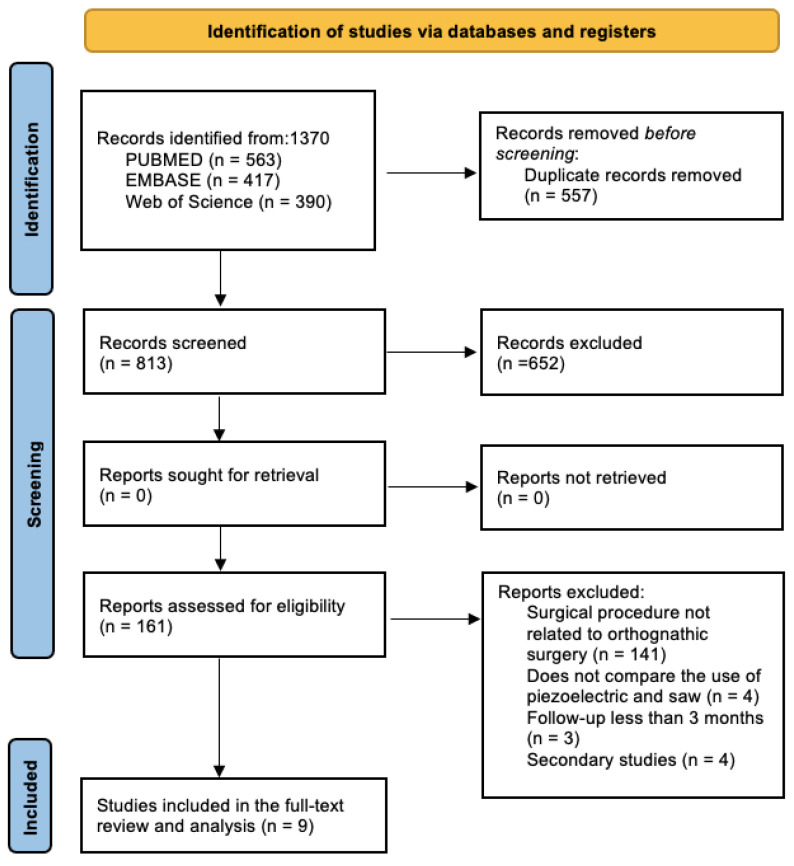 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthodontics and Dentofacial Orthopedics · Craniofacial Disorders and Treatments · Facial Nerve Paralysis Treatment and Research
1. Introduction
The introduction should Malocclusion affects approximately two-thirds of the world’s population [1] and is related to changes in facial structure with clinical problems, such as phonation and oral communication, difficulties in chewing, respiratory disorders, and others. Its etiology is usually multifactorial, influenced by genetic and environmental factors The classification of malocclusion is related to the position of some teeth [2] and can be present as the consequence of deficiencies in maxillomandibular position.
A poor three-dimensional relationship between the maxilla and mandible is frequently linked to malocclusions. In some clinical situations of moderate or severe discrepancies, orthognathic surgery is the treatment of choice, considered an effective surgical procedure that allows correction and restoration of muscular and masticatory function, phonation, respiration, and facial harmony [3].
In orthognathic surgery, the ultrasound system (piezoelectric) has become an alternative to conventional instruments like the saw. The use of piezoelectric (PE) reduces the risk of soft tissue injury and enhances less bleeding, which improves the accuracy of the osteotomy. Despite its advantages, the disadvantage has been raised that piezoelectric can take up 2 to 4 times longer than an osteotomy with a reciprocating saw and is more expensive than other surgical systems [4].
The different tools used in osteotomies can cause increased intraoperative bleeding, postoperative edema, and postoperative neurosensory alterations; the reciprocating saw commonly used in orthognathic surgery frequently poses challenges in control, limited visibility, and the conversion of electrical energy into a mechanical or rotary cutting motion, which can generate heat affecting adjacent structures like nerves and muscles, potentially leading to postoperative deterioration [5,6].
This study assesses differences in postoperative neurosensory impairment when using a piezoelectric device and a saw in orthognathic surgery.
2. Materials and Methods
2.1. Study Design
A literature review followed PRISMA-ScR [7] (Supplementary Materials Table S1) recommendations to answer the research question: Do neurosensory modifications differ following orthognathic surgery when an osteotomy uses piezoelectric versus saw systems? P: subjects who underwent orthognathic surgery; I: orthognathic surgery using piezoelectric surgery; C: orthognathic surgery using a saw; O: presence of neurosensory impairment and follow-up of three months or longer post-surgery.
2.2. Eligibility Criteria
We included studies evaluating the neurosensory response in orthognathic surgeries with piezoelectric and/or saw, in which a Le Fort osteotomy and/or sagittal mandibular ramus osteotomy was performed in a sample of more than 10 subjects with a follow-up of 3 months or more. Animal studies and studies in which the neurosensory response was evaluated in procedures other than orthognathic surgeries were excluded.
2.3. Source of Information and Search Strategy
A search was conducted from the year 2000 [8] (since it was in that year that the first article describing the use of piezoelectric in oral and maxillofacial surgery was published) to December 2024, which included articles in the PubMed, Embase, and Web of Science databases. Studies in English and Spanish were selected; there were no limitations in the type of study design. (((((((“Orthognathic Surgery”[Mesh]) OR (orthognathic surgeries)) AND (“Maxillary Osteotomy”[Mesh])) OR (osteotomy Lefort I)) AND (“Osteotomy, Sagittal Split Ramus”[Mesh])) OR (Sagittal split osteotomy)) AND (neurosensory disturbance)) OR (neurosensory alterations).
2.4. Study Selection and Data Extraction
The complete list of identified references was imported into the Mendeley 2.90.0 software (Reference Management, Elsevier, London, UK), where duplicates were automatically removed. Titles and abstracts were independently screened for eligibility by two investigators. In case of discrepancy, consensus was obtained by discussion or consultation with a third reviewer. References that appeared to fulfill the inclusion criteria were reviewed in full text by the same reviewers.
Data extraction was performed by two reviewers using a predefined and standardized data form:
- (a)Study group data (number of patients, sex, age, and race);
- (b)Research data (prospective or retrospective nature of the study, surgical procedure, surgical technique, and complementary technique);
- (c)Type of data analyzed (clinical methods to determine the presence of paresthesia and follow-up).
3. Results
The search conducted using the three metasearch engines yielded 1370 results, of which 557 were excluded due to duplication. A total of 813 articles were obtained for review based on title and abstract, using inclusion and exclusion criteria. Of all the studies analyzed, nine articles [9,10,11,12,13,14,15,16,17] were selected for full-text analysis (Figure 1).
The selected articles included a total of 731 subjects. The age range of the studies included was between 18 and 49 years. Concerning sex, 242 subjects were male (40%), and 371 were female (60%); only one study [8] did not mention the number of male and female patients. All the selected studies had a minimum follow-up of 3 months, ranging from 1 to 36 months (Table 1). Regarding the country where the study was conducted, only two mentioned the country where it was performed: Italy [11] and Brazil [16]. Four studies were prospective in design, and two were retrospective.
A total of 597 orthognathic surgeries were performed, of which 90 were performed in one hemiarch with piezoelectric (PE) and the other with a saw [12,13,15]. Two hundred thirty-seven operations were performed only with piezoelectric, 114 operations only with saw, and only one study did not mention how many surgeries were performed with piezoelectric or saw [14]. All the selected studies performed post-surgical follow-ups: one study performed follow-up up to 36 months [16], three studies up to 12 months [11,13,15], two studies up to 6 months [12,17], and one study up to 3 months [8,9,14]. Four studies assessed the measurement of neurosensory alterations using the light brush technique and two-point discrimination. In contrast, three studies evaluated it using the visual analog scale, neurosensory tests, light touch, and the two-point discrimination test [13,14,17]. Only one study was evaluated using the Semmes–Weinstein test [12].
Some authors reported that paresthesia after orthognathic surgery lasted up to 6 months [11,12,13,15,17], and that in the period between 2 and 3 years, the changes were insignificant. In the study by Da Costa et al. [16], of 376 patients, 152 presented paresthesia at 6 months. In the study by Cascino et al. [17], of a total of 100 patients, only 40 recovered skin sensitivity during the first month, while the study by Köhnke et al. [13] indicated that all patients presented postoperative paresthesia and that 50 presented paresthesia that gradually improved, reaching preoperative levels at 12 months. Sobol et al. [11] reported that in a study with 20 patients, none presented postoperative alterations in the sensitivity of the lingual nerve. Kokuryo et al. [14] reported that among 67 patients, only 22 presented paresthesia at 3 months, and Monnazzi et al. [12] stated that, of the 20 patients who underwent surgery, the side of the mandible operated on with piezoelectric recovered sensitivity, while the side treated with the saw took 6 months to recover sensitivity. Bertossi et al. [11] observed that at 12 months, all subjects operated on with piezoelectric instruments had recovered sensitivity within a mild to moderate range, whereas in the saw group, eight out of fifty-five subjects had not yet recovered sensation. Of those eight subjects evaluated at 12 months, only three had regained slight sensitivity in the area.
One study mentioned that sensitivity recovery was faster in patients operated on with piezoelectric, with a median recovery of 97 days, compared to the saw that presented a median recovery of 123 days [15]. In another study, however, it is mentioned that 16 patients out of 35 treated with piezoelectric and 28 out of 32 treated with saw did not recover sensitivity until the end of that study [14].
Regarding anatomy, the areas most affected were the lower lip and chin [12,16]. Of the six studies analyzed, three mentioned that surgeries performed with piezoelectric were positively associated with neurosensory recovery, in addition to a shorter operating time and a less painful and faster postoperative recovery compared to the saw, which presented a greater demand for analgesics and hospital stay [12,15,17].
In relation to Table 2, two studies mentioned that there was no significant difference in sensitivity recovery between the saw and the piezoelectric [12,14], and only one study included an analysis of risk factors for the development of sensory disturbances, which are as follows: advanced age, extensive mandibular advancement, and surgical procedures for nerve detachment. They also pointed out that in the analysis of the recovery of neurosensory alterations at 3 years, only 41 still presented some type of paresthesia without mentioning how many of these were performed with a saw or piezoelectric.
4. Discussion
The reciprocating saw has been a fundamental tool in osteotomies in orthognathic surgery for decades, achieving satisfactory results with low complication rates [18]. However, the introduction of the PE in the early 2000s marked a significant advance in technology for maxillofacial surgery [8]. Its characteristics, such as cooling, lower heat generation, and precision cutting that preserves soft tissues, make deep osteotomies possible and minimize surgical trauma, potentially reducing damage to adjacent neurovascular structures. This accuracy and reduced tissue damage appear to be a key advantage of PE [10].
The descriptive analysis of the six studies, which included 633 patients, showed no clinical differences between the two devices, and all studies reported the presence of postoperative paresthesia. However, differences were observed in the recovery time from these sensory alterations, with a shorter recovery time after six months in patients who underwent surgery with piezoelectric devices. This finding suggests that, although both methods may result in a similar incidence of paresthesia, piezoelectric surgery may be associated with faster sensory recovery. It is important to note that factors such as age, the type of surgery (whether advancement or setback), and the presence of sagittal facial abnormalities and/or asymmetries can influence the occurrence of facial sensory impairment.
The proximity of maxillomandibular osteotomies to sensitive nerve structures such as the inferior alveolar, infraorbital, and lingual nerves explains the high prevalence of postoperative neurosensory disturbances. Specifically, the sagittal ramus mandibular osteotomy (SRMO) shows an incidence of paresthesia ranging from 25% to 98% in the immediate postoperative period and from 10% to 30% in the long term [19]. This variability in the incidence of paresthesia could be influenced by several factors, including patient age, surgeon experience, type of instrumentation used, bone density, magnitude of surgical movement, concomitant genioplasty, and kind of fixation used [20,21].
Previous studies [22] have reported benefits of PE in neurosensory recovery, observing greater sensory function at 12 months in patients operated on with this technique compared to the saw. However, other studies like that by Köhnke et al. [13], which analyzed 50 patients, found no significant differences between the two methods. This discrepancy in findings could be attributed to the inherent variability in clinical studies, including differences in the characteristics of the study population, the surgical protocol used, and the surgeons’ experience. It has been reported that a less experienced surgeon is up to three times more likely to experience postoperative complications [23]. Although a high percentage of neurosensory disturbances resolve within the first 6 to 12 months, persistent disturbances may affect the patient’s quality of life and require additional interventions.
The development of the surgical technique also determines the neurosensory and postoperative recovery. For example, Raffaini et al. [24] used a hybrid use of the piezoelectric system in conjunction with chisels. In contrast, Olate et al. [25] used the PE tip exclusively without chisels or saws. It is possible to speculate that the postoperative outcomes could vary between the two scenarios. Although the piezoelectric system tends to increase the duration of the surgical procedure by approximately 30 to 50%, especially when cutting dense cortical bone, it has also been observed to reduce the incidence of sensitivity due to the preservation of soft tissues, including the perineurium of the nerve [26]. Several authors [27,28] mention that higher rotational speeds result in greater temperature ranges with smaller temperature variations and a reduction in surgical time, but that immediate cellular damage is associated with both the magnitude and duration of heat exposure. For their part, Delgado-Ruiz et al. [29], through in vitro studies, evaluated temperature variations in dense and trabecular bone tissue using two piezoelectric devices at 30 kHz, and they observed no differences in the temperature and time recorded during osteotomies performed with both devices. However, dense bone resulted in greater changes in temperature and time compared to osteotomies in trabecular bone.
Sagittal ramus mandibular osteotomy is one of the most common surgical procedures used to correct mandibular deformities such as prognathism, retrognathism, and facial asymmetry [30]. The anatomical conditions observed in dentofacial deformities could be associated with the position of the nerve and the internal mandibular canal [31]; in terms of skeletal class, individuals with Class III deformities present a higher chance of nerve paresthesia during mandibular setback than during mandibular advancement and then Class II patients. An anatomical option to explain these differences could be because Class III patients have a shorter distance between the buccal side of the cortical bone and the mandibular canal in the mandibular ramus than those with Class II skeletal deformities [32]. Those anatomical conditions are not included in the main articles to compare the treatment using PE or saw, and this bias in sample inclusion and selection can also explain the results in some papers published in this field.
Although the use of piezoelectric instruments during osteotomy allows for a precise cut on mineralized tissue and helps protect neurovascular structures by reducing thermal injury and microfractures [33,34], in the study by Gopinath et al. [35], an evaluation was carried out on the incidence of neurosensory disturbances following SRMO for mandibular setback. They observed that, among the 31 sites where the alveolar nerve was in the distal segment, there was no nerve manipulation, and the presence of postoperative neurosensory issues was low. In contrast, in the 14 sites where the nerve was found in the proximal segment, it had to be released in 60% of the cases, which presented a higher frequency of neurosensory disturbances. These data explain that another bias, such as osteotomy design, may be included in the comparative analysis, showing differences in the reports on the efficiency of the PE system.
5. Conclusions
The methodological heterogeneity among the included studies, including sample size and variability of factors, makes it difficult to draw definitive conclusions about the superiority of one method over the other in preventing neurosensory disturbances. Future studies with more robust designs, larger samples, and standardized evaluation methodologies are needed to clarify the influence of instrument type on postoperative neurosensory morbidity. However, we can conclude that the piezoelectric system offers conditions that allows a faster recovery from postoperative paresthesia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Čelar A. Tafaj E. Graf A. Lettner S. Association of anterior and posterior occlusal planes with different Angle and skeletal classes in permanent dentitions J. Orofac. Orthop.20187926727610.1007/s 00056-018-0139-z 29777251 PMC 6061169 · doi ↗ · pubmed ↗
- 2Ghodasra R. Brizuela M. Orthodontics Malocclusion. Stat Pearls Publishing 2025 Available online: https://www-ncbi-nlm-nih-gov.translate.goog/books/NBK 592395/?_x_tr_sl=en&_x_tr_tl=es&_x_tr_hl=es&_x_tr_pto=tc(accessed on 27 March 2025)37276298 · pubmed ↗
- 3Daluz A.D.J. da Silva T.V.S. Tôrres B.O. Costa D.F.N. Santos L.A.M. Long-term airway evolution after orthognathic surgery: Systematic Review J. Stomatol. Oral Maxillofac. Surg.202212319119810.1016/j.jormas.2021.04.00633882343 · doi ↗ · pubmed ↗
- 4Alrefai M. Daboul A. Fleischhacker B. Landes C. Piezoelectric versus conventional techniques for orthognathic surgery: Systematic review and meta-analysis J. Stomatol. Oral Maxillofac. Surg.202212327327810.1016/j.jormas.2021.12.00534923189 · doi ↗ · pubmed ↗
- 5Gilles R. Couvreur T. Dammous S. Ultrasonic orthognathic surgery: Enhancements to established osteotomies Int. J. Oral Maxillofac. Surg.20134298198710.1016/j.ijom.2012.12.00423312501 · doi ↗ · pubmed ↗
- 6Spinelli G. Lazzeri D. Conti M. Agostini T. Mannelli G. Comparison of piezosurgery and traditional saw in bimaxillary orthognathic surgery J. Craniomaxillofac. Surg.2014421211122010.1016/j.jcms.2014.02.01124742747 · doi ↗ · pubmed ↗
- 7Tricco A.C. Lillie E. Zarin W. O’Brien K.K. Colquhoun H. Levac D. Moher D. Peters M.D.J. Horsley T. Weeks L. PRISM Extension for Scoping Reviews (PRISMA-Sc R): Checklist and Explanation Ann. Intern. Med.201816946747310.7326/M 18-085030178033 · doi ↗ · pubmed ↗
- 8Vercellotti T. Piezoelectric surgery in implantology: A case report—A new piezoelectric ridge expansion technique Int. J. Periodontics Restor. Dent.20002035836511203575 · pubmed ↗