Clinical Relevance of IFT140 Loss-of-Function Variants in Development of Renal Cysts
Carlotta Pia Cristalli, Sara Calabrese, Luca Caramanna, Andrea Pietra, Giulia Vitetta, Bianca De Nicolo, Elena Bonora, Giulia Severi, Soara Menabò, Simona Ferrari, Francesca Ciurli, Valeria Aiello, Irene Capelli, Andrea Pasini, Irene Alberici, Roberto Pillon, Claudio La Scola

TL;DR
This study finds that loss-of-function variants in the IFT140 gene can cause a milder, atypical form of autosomal dominant polycystic kidney disease.
Contribution
The study identifies IFT140 as a new gene associated with atypical ADPKD and highlights hyperuricemia as a novel clinical feature.
Findings
IFT140 loss-of-function variants were found in 14 patients, contributing to an atypical, milder form of ADPKD.
Hyperuricemia is a previously unappreciated feature of IFT140-related ADPKD.
IFT140 variants were linked to bilateral kidney cysts and later-onset renal decline.
Abstract
Background: Autosomal dominant polycystic kidney disease (ADPKD) is the most common inherited kidney disease, affecting approximately 1 in 1000 individuals. This genetically heterogeneous condition is primarily caused by monoallelic pathogenic or likely pathogenic variants in the PKD1 and PKD2 genes, accounting for 78% and 15% of typical cases, respectively. Recently, the application of NGS methods has led to the identification of additional genes associated with ADPKD, which have been incorporated into routine diagnostic testing for detecting phenocopies of the disease. Methods: In this study, targeted NGS (tNGS) analysis of the main cystogenes associated with classic and atypical ADPKD was performed in a cohort of 218 patients clinically diagnosed with cystic nephropathies. Results: Genetic testing identified variants in 175 out of 218 cases (80.3%). Among these, 133 probands (76%)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
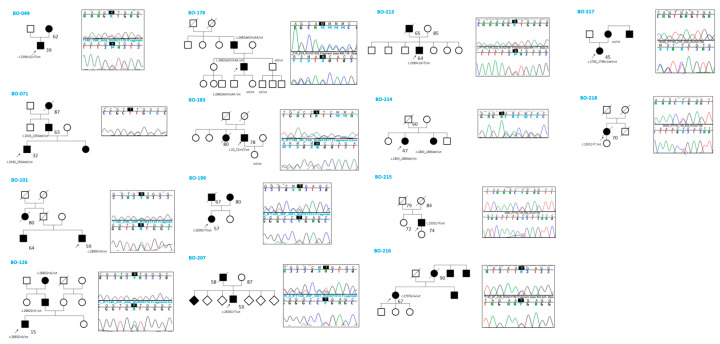 Figure 1
Figure 1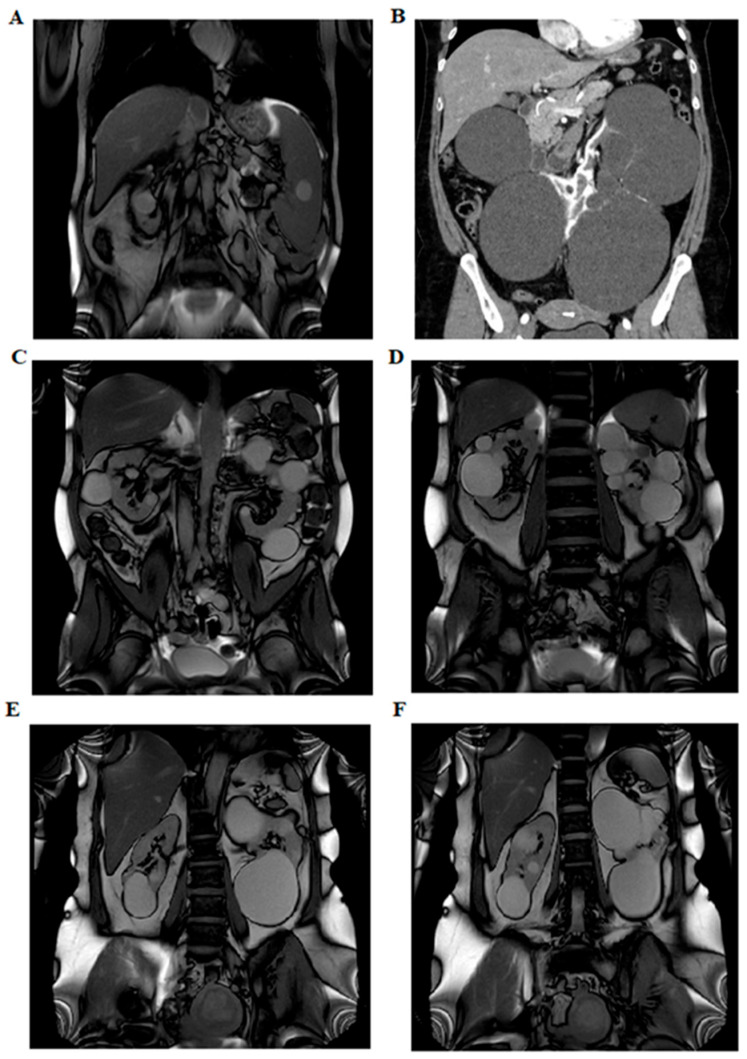 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic and Kidney Cyst Diseases · Renal and related cancers · Renal cell carcinoma treatment
1. Introduction
Autosomal dominant polycystic kidney disease (ADPKD (MIM: 173900)) is the most common inherited kidney disease, affecting approximately 1 in 1000 individuals. It is characterized by the progressive formation and enlargement of renal cysts, leading to kidney enlargement and, ultimately, renal failure. ADPKD is the fourth leading cause of end-stage renal disease (ESRD) in adults worldwide [1,2,3]. ADPKD can be classified as a multisystemic disorder, as it presents with both renal and extrarenal manifestations. These include polycystic liver disease (PLD), which may occasionally require surgical intervention, and the risk of ruptured intracranial aneurysms, leading to subarachnoid hemorrhage [4,5]. ADPKD is a genetically heterogeneous condition, with monoallelic pathogenic variants in PKD1 (encoding polycystin-1, PC1 (MIM: 601313)) and PKD2 (encoding polycystin-2, PC2 (MIM: 173910)) accounting for approximately 78% and 15% of cases, respectively [3].
The causative gene and the type of variant (loss-of-function (LoF) vs. missense) influence disease outcomes: PKD1-related disease is more severe, with an average age of onset for end-stage renal disease (ESRD) at 58.0 years, compared to 74.8 years for PKD2-related cases. Total kidney volume (TKV), assessed via MRI, is a strong predictor of disease severity [6]. Recent advancements in next-generation sequencing (NGS) techniques, including whole-exome sequencing (WES) and targeted NGS panels (tNGS), have led to the identification of additional ADPKD-associated genes, which are now incorporated into routine diagnostic testing [7,8,9]. Recent studies have highlighted the IFT140 gene as an important contributor to ADPKD. Senum et al. reported monoallelic pathogenic IFT140 variants in 12 multiplex ADPKD families and 26 singleton index cases. Heterozygous loss-of-function (LoF) IFT140 variants result in an atypical, mild form of ADPKD characterized by large bilateral cysts and renal functional decline at older ages [10], along with a few liver cysts. Additionally, Salhi et al. confirmed that heterozygous IFT140 frameshift variants are responsible for a renal cystic phenotype. Their study also raised the possibility of an associated cardiac phenotype, specifically dilated cardiomyopathy. This condition was of unknown origin, as exome sequencing analysis failed to identify an alternative genetic cause, suggesting a potential link between IFT140 and heart disease [11]. Dordoni et al. included the IFT140 gene in a new NGS panel and retrospectively analyzed a cohort of patients with a negative ADPKD-spectrum diagnosis. Loss-of-function pathogenic variants in the IFT140 gene were identified in three unrelated patients (2.3%) [12]. The IFT140 gene (MIM: 614620) consists of 31 exons and has a coding region of 4386 bp (GenBank: NM_014714.4). It encodes the IFT140 protein, composed of 1462 amino acids (GenBank: NP_055529.2). IFT140 is a key component of the IFT-A core complex responsible for dynein-associated retrograde trafficking of proteins from the ciliary tip back to the basal cell body [13,14,15]. Bi-allelic pathogenic variants in IFT140 have been associated with the syndromic ciliopathy Short-Rib Thoracic Dysplasia 9 with or without Polydactyly (SRTD9 (MIM: 266920)), also known as Mainzer–Saldino Syndrome [16,17,18]. The SRTD9 phenotype includes retinal dystrophy, skeletal malformations (small thorax, cone-shaped epiphyses, craniofacial abnormalities, and digit malformations), and chronic kidney disease (renal cysts and fibrosis) [16,17]. Additionally, bi-allelic variants in IFT140 are associated with non-syndromic forms of retinal dystrophies (MIM: 617781) [19].
In this study, we use a targeted NGS approach to analyze known cystogenes [20] and describe 14 Italian families exhibiting monoallelic LoF variants in IFT140, including the second reported case of pediatric IFT140-related diagnosis. Notably, 35.7% of the patients (5 out 14) also presented with hyperuricemia.
2. Materials and Methods
2.1. Patient Recruitment
A cohort of 218 patients with a clinical diagnosis of ADPKD was referred from various centers to the Medical Genetics Unit at IRCCS Azienda Ospedaliero-Universitaria of Bologna over a 15-month period (January 2023–March 2024). Genetic counseling was provided both before and after genetic testing. All patients provided informed consent for genetic analyses and the potential publication of results.
Ethical review and approval were waived for this study because sample analysis did not deviate from current clinical practice, and local policy allows reporting of clinical data provided that the patients involved have expressed their agreement through the informed consent form. Clinical and imaging data were collected through a review of medical records. Hyperuricemia was defined as a serum uric acid level > 6.8 mg/dL [21] or acute gout attack.
2.2. Genetic Testing
Genetic testing was performed on DNA isolated from EDTA peripheral blood using a semi-automatic Maxwell 16 instrument (Promega Corporation, Madison, WI, USA). Targeted next-generation sequencing (tNGS) was conducted using a panel of 17 polycystic kidney disease (PKD) and ciliopathy genes, as detailed in Table S1.
Raw sequencing data were transferred to the Torrent Server, where TorrentSuite™ performed alignment to a reference genome to generate FASTQ files, a Binary Alignment Map (BAM) with a corresponding Binary Alignment Index (BAI), and Variant Call Format (VCF) files. Reads were aligned to the reference genome based on Human Genome 19 (GRCh37). All VCF files were uploaded into Ion Reporter software v5.10 (Thermo Fisher Scientific Inc., Waltham, MA, USA), selecting the Annotation Variant workflow to associate each variant with its nucleotide change in the mRNA transcript, amino acid change, exon or intronic variant (IVS) location, and function.
BAM/BAI files generated after alignment were visualized using the Integrative Genome Viewer (IGV) software v2.18.2 to assess sequencing read depth, zygosity, read quality, and mapping accuracy. Variant filtering based on population frequency was performed using population databases, including ExAC, gnomAD v4.1.0 [22], 1000 Genomes [23], and dbSNP, retaining only alleles with a minor allele frequency (MAF) ≤ 0.01. Variants were then annotated according to the guidelines of the Human Genome Variation Society [24] and classified into five categories following the standards of the American College of Medical Genetics and Genomics (ACMG) [25].
To achieve this, public variant databases such as ClinVar [26] and LOVD [27], as well as online tools including VarSome Premium [28] and Franklin [29], were utilized. The potential significance of missense variants was assessed using SIFT4G, PolyPhen-2, MutationTaster, MutationAssessor, PROVEAN, FATHMM, BLOSUM, REVEL, and CADD. Large rearrangements in PKD1 or PKD2 genes were excluded using multiplex ligation-dependent probe amplification (SALSA MLPA kit P351 PKD1, Lot No. D1-0421, and P352 PKD1-PKD2, Lot No. E1-0421, MRC-Holland).
Exon-specific PCR primers were designed for confirmation of variants identified in IFT140. Primer sequences are available upon request. Segregation analysis was conducted in family members, where possible, to support the causative role of IFT140 variants. Some patients underwent abdominal imaging via nuclear magnetic resonance imaging (MRI) and/or computed tomography (CT).
3. Results
From January 2023 to March 2024, 218 individuals with a clinical diagnosis of cystic nephropathy suggestive of ADPKD were evaluated (110 females and 108 males, with a mean age of 47 years at clinical diagnosis). Genetic testing identified a variant in 175 out of 218 cases (80.3%). Among these, 133 probands (76%) carried likely pathogenic or pathogenic variants in one or more genes included in the panel, while 42 cases (24%) harbored a variant of unknown significance (VUS). Specifically, in 111 (83.5%) out of 133 cases, one or more class 4/5 variants in PKD1, PKD2, or both were identified.
Within our cohort, 13 patients (9.8%) carried more than one variant, and 23 (16.5%) had causative variants in genes associated with atypical or uncommon forms of ADPKD. A molecular defect could not be detected in 43 cases (19.7%). The complete list of variants identified through tNGS is provided in Table S2. Notably, heterozygous loss-of-function (LoF) variants in IFT140 (NM_014714.4) were identified in 14 index cases out of 133 (10.5%, 6.4% of the global cohort). These included four frameshift variants c.20_21insT (p.Gln8ProfsTer82), c.1863_1866del (p.Glu623ArgfsTer20), c.2545_2554del (p.Val849TrpfsTer24), c.2682delCinsAA (p.His894GlnfsTer58), four stop-gain variants c.919C > T (p.Arg307Ter), c.1501C > T (p.Arg501Ter), c.2500C > T (p.Arg834Ter), c.2880G > A (p.Trp960Ter), and two splice-site defects c.2399 + 1G > T and c.2766_2768 + 1del. Some variants were recurrent (Table 1).
The proband (BO-216) carrying the p.Arg307Ter variant also harbored an IFT140 missense variant classified as a VUS c.2797G > A (p.Glu933Lys). Furthermore, proband BO-199 had an additional variant in PKD1 classified as a VUS, c.2411A > G (p.Asn804Ser), and proband BO-133 had a dual molecular diagnosis since an HNF4A whole gene deletion causing MODY type 1 was identified.
Table 1 summarizes the genetic coordinates of the identified variants, their frequencies in the gnomAD v4.1.0 population database, and their classification according to ACMG guidelines. Clinical features are detailed in Appendix A reported below. In summary, all probands (nine males, five females) presented with bilateral cortical renal cysts (average age at clinical diagnosis was 47 years), while liver involvement was observed in one single patient (B0-215). The detection of kidney cysts was usually accidental, e.g., during the work-up for unexplained high blood pressure, which was present in nine patients. The severity of kidney dysfunction was heterogeneous, ranging from normal kidney function to end-stage renal disease (ESRD) (Table 2).
Among the 11 patients with available data, six (54.5%) had an eGFR >60 mL/min, three (27.3%) had CKD stage IIIa, and two (18.2%) had CKD stage IV.
Five cases also exhibited hyperuricemia (BO-101, BO-178, BO-207, BO-213, and BO-218)—a trait described for the first time in this study. Regarding extrarenal phenotypes, 11 out of 14 patients underwent cardiac ultrasound, and four individuals (BO-101, BO-213, BO-216, BO-217) were found to have mitral valve prolapse; however, none had dilated cardiomyopathy. Two individuals (BO-214 and BO-216) were found to have cerebral aneurysms, although none ruptured. BO-199 had mild right microphthalmia. All patients, except one (BO-215), had a positive family history of cystic kidney disease. Segregation analysis of the identified variants was performed in 6 out of 14 families (Figure 1).
In five of these families, the respective variant co-segregated with the cystic phenotype. In family BO-217, the c.2766_2768 + 1del variant was absent in the affected mother, who instead carried an ALG8 variant: c.980C > G (p.Thr327Arg), absent in the proband, classified as a VUS (CADD: Benign Moderate (21.7)). Abdominal MRI images of three patients (BO-183, BO-214, and BO-216) showing multiple bilateral cortical renal cysts are provided in Figure 2.
4. Discussion
ADPKD is the most common inherited cause of end-stage renal disease (ESRD) worldwide, with an estimated birth prevalence of approximately 1 in 1000. The two primary genes associated with ADPKD are PKD1 and PKD2. However, additional genes, including IFT140, GANAB, DNAJB11, ALG8, and ALG9, have been identified in association with rarer ADPKD phenocopies. Variants in these newly recognized disease-associated genes should be considered in cases presenting with atypical imaging patterns (e.g., unilateral, asymmetric, segmental, lopsided, or bilateral cystic disease with unilateral or bilateral kidney atrophy) or in the absence of typical extrarenal manifestations, such as liver cysts [30]. The IFT140 gene is emerging as the third most common and frequently mutated gene in individuals with ADPKD, with a clinical picture that is usually at the milder end of the phenotypic spectrum: ESRD is rare but can occur in older individuals [10,11,12,17,30]. Due to the mild phenotype of polycystic kidney disease associated with the IFT140 gene, renal disease in parents may go unnoticed. Consequently, patients lacking a documented family history are more likely to harbor pathogenic variants in the IFT140 gene [31].
In this study, we report the results of a tNGS analysis of cystogenes responsible for classic and atypical ADPKD obtained in a cohort of 218 consecutive unrelated individuals who were tested in a single laboratory. As expected, PKD1 and PKD2 are the most prevalent genes, with a causative variant identified in 111 index-positive cases (83.5%), as shown in Table S2. The IFT140 gene is confirmed to be the third most frequently mutated gene in these patients, with 14 unrelated patients out of 218 (6.5%). In addition, we provide a detailed clinical description of these 14 Italian families (Table 1), including the second pediatric IFT140-related phenotype, the first with a single nucleotide variant (SNV). At the time of this publication (March 2025), the only reported pediatric case in the literature was that of a 6-year-old girl with cystic nephroma and a heterozygous deletion of exon 13 in the IFT140 gene. The molecular diagnosis in the patient was established after nine years, as the initial NGS sequencing had yielded negative results [32]. As can be seen from Seeman’s study, a limitation of our study is the lack of IFT140 structural variants investigation in atypical negative cases. MLPA IFT140 analysis could improve the detection rate of our diagnostic test.
Our results support the findings of previous studies: heterozygous pathogenetic IFT140 variants are the third genetic cause of ADPKD, and liver involvement is rare (BO-215) and many carriers show atypical features in renal cyst size and locations, such as large, exophytic cysts (BO-183), with a total kidney volume not increased and preserved renal function compared to classical ADPKD caused by PKD1/2 variants. Renal functional decline occurs only late in life, in contrast to what happens in patients with the classic ADPKD form. The prevalence of arterial hypertension is comparable to that observed in patients with pathogenic variants in PKD1/2. None of our patients had a cardiac phenotype (DCM) as described by Salhi S [11], but four showed mitral valve prolapse. Interestingly, 5/14 patients (35.7%) exhibited a hyperuricemic trait. The coexisting presence of CKD in three of them is a possible influencing factor.
To the best of our knowledge, this study reports the highest incidence of IFT140 LOF variants in a cohort of subjects with cystic nephropathy. A recent large European cohort reported IFT140 LOF variants in seventy-five individuals (from 61 independent families) among 2797 with ADPKD-like phenotypes [33]. The prevalence is less than 3%, similar to a distinct Italian cohort (2.3%) [12], but much lower than what we report here (6.4%). One possible explanation may be that our cohort is enriched with atypical cases, mirroring an enhanced interest of clinical nephrologists to identify the origin of renal cystic phenotypes and a frequent request for genetic tests.
Among the 11 variants identified in this case series, ten are loss of function, four of which are recurrent, and one missense. Five are novel variants, while six are reported in population databases (gnomADv4.1.0). In this context, as many as 7 of the 11 variants identified in our cohort are located between intron 19 and exon 23, suggesting that there may be a mutational hotspot.
The only missense variant, c.2797G > A (p.Glu933Lys), was classified as VUS and was present in proband BO-216 together with p.Arg307Ter. Unfortunately, the phase is unknown because no family members could be tested, but the phenotype was mild (few large kidney cysts at 67 years with normal renal function). Another individual, BO-199, had an IFT140 LOF variant (p.Arg834Ter) and a missense variant in PKD1 (p.Asn804Ser) classified as VUS. It is intriguing to note that both parents were known to have cystic nephropathy, but the father died at 67, and the mother, 80 years old, was not available for testing, but the presence of renal cysts was confirmed. This patient seemingly had a mild phenotype (bilateral kidney cysts, normal renal function at 57 years) but presented microhaematuria and was on regular follow-up. We also report a subject with a dual molecular diagnosis, BO-133, who had chronic kidney disease (stage IV at 78 years) with multiple bilateral cysts and diabetes mellitus: he had a frameshift variant in IFT140, but he was also found to have a whole gene deletion of HNF4A associated to MODY type 1. The association of MODY with a renal cystic phenotype caused by an IFT140 LOF variant might have accelerated the decrease in renal function.
Segregation analysis could be performed in six families, and the respective variant was found to co-segregate with the cystic phenotype in five families. In one family (BO-217), the c.2766_2768 + 1del variant was not present in the affected mother who had a classic ADPKD phenotype (multiple cysts in kidney and liver, ESRD at 55 years), but no variants were identified in PKD1 or PKD2; she was found to carry an ALG8 variant (p.Thr327Arg), absent in the proband, but this SNV cannot be definitely associated to the phenotype at the moment (it is classified as VUS with a CADD score benign moderate [21.7]).
Overall, genetic factors are increasingly recognized to contribute significantly to cystic nephropathies, even in mild/atypical cases where variants in genes other than PKD1 and PKD2 are more frequently identified. Among these genes, IFT140 is emerging as an important phenotypic driver. It is likely that several milder cases will turn out to be oligogenic with distinct genetic contributions. At the same time, in the interplay among different cystogenes, IFT140 variants may well be considered candidates to modify the disease course of PKD1- and PKD2-related ADPKD.
5. Conclusions
This study confirms that IFT140 LoF variants represent a strong contributor to renal cyst development. Kidney function is usually preserved even in older individuals, but a careful follow-up is warranted. The possible association with extrarenal manifestations is not common and needs larger clinical cohorts to be ascertained, but this study does not confirm the association with dilated cardiomyopathy. Hyperuricemia appears to be a new trait associated with this condition. Further studies in larger cohorts will be needed to confirm this evidence. Finally, expanding genetic testing beyond PKD1 and PKD2 is crucial in order to achieve an accurate diagnosis and should definitely include IFT140.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cornec-Le Gall E. Alam A. Perrone R.D. Autosomal Dominant Polycystic Kidney Disease Lancet 201939391993510.1016/S 0140-6736(18)32782-X 30819518 · doi ↗ · pubmed ↗
- 2Bergmann C. Guay-Woodford L.M. Harris P.C. Horie S. Peters D.J.M. Torres V.E. Polycystic Kidney Disease Nat. Rev. Dis. Primers 201845010.1038/s 41572-018-0047-y 30523303 PMC 6592047 · doi ↗ · pubmed ↗
- 3Mantovani V. Bin S. Graziano C. Capelli I. Minardi R. Aiello V. Ambrosini E. Cristalli C.P. Mattiaccio A. Pariali M. Gene Panel Analysis in a Large Cohort of Patients with Autosomal Dominant Polycystic Kidney Disease Allows the Identification of 80 Potentially Causative Novel Variants and the Characterization of a Complex Genetic Architecture in a Subset of Families Front. Genet.20201146410.3389/fgene.2020.0046432457805 PMC 7224062 · doi ↗ · pubmed ↗
- 4Sanchis I.M. Shukoor S. Irazabal M.V. Madsen C.D. Chebib F.T. Hogan M.C. El-Zoghby Z. Harris P.C. Huston J. Brown R.D. Presymptomatic Screening for Intracranial Aneurysms in Patients with Autosomal Dominant Polycystic Kidney Disease Clin. J. Am. Soc. Nephrol.2019141151116010.2215/CJN.1469121831362991 PMC 6682820 · doi ↗ · pubmed ↗
- 5Heyer C.M. Sundsbak J.L. Abebe K.Z. Chapman A.B. Torres V.E. Grantham J.J. Bae K.T. Schrier R.W. Perrone R.D. Braun W.E. Predicted Mutation Strength of Nontruncating PKD 1 Mutations AIDS Genotype-Phenotype Correlations in Autosomal Dominant Polycystic Kidney Disease J. Am. Soc. Nephrol.2016272872288410.1681/ASN.201505058326823553 PMC 5004648 · doi ↗ · pubmed ↗
- 6Lavu S. Vaughan L.E. Senum S.R. Kline T.L. Chapman A.B. Perrone R.D. Mrug M. Braun W.E. Steinman T.I. Rahbari-Oskoui F.F. The Value of Genotypic and Imaging Information to Predict Functional and Structural Outcomes in ADPKDJCI Insight 20205 e 13872410.1172/jci.insight.13872432634120 PMC 7455088 · doi ↗ · pubmed ↗
- 7Aiello V. Ciurli F. Conti A. Cristalli C.P. Lerario S. Montanari F. Sciascia N. Vischini G. Fabbrizio B. Di Costanzo R. DNAJB 11 Mutation in ADPKD Patients: Clinical Characteristics in a Monocentric Cohort Genes 202315310.3390/genes 1501000338275584 PMC 10815778 · doi ↗ · pubmed ↗
- 8Cornec-Le Gall E. Olson R.J. Besse W. Heyer C.M. Gainullin V.G. Smith J.M. Audrézet M.P. Hopp K. Porath B. Shi B. Monoallelic Mutations to DNAJB 11 Cause Atypical Autosomal-Dominant Polycystic Kidney Disease Am. J. Hum. Genet.201810283284410.1016/j.ajhg.2018.03.01329706351 PMC 5986722 · doi ↗ · pubmed ↗