Survival Outcomes of Luminal Metastatic Breast Cancer Patients According to Changes in Molecular Subtype at Re-Biopsy: Insights from the GIM-13—AMBRA Study
Marina Elena Cazzaniga, Paolo Pronzato, Domenico Amoroso, Grazia Arpino, Francesco Atzori, Alessandra Beano, Laura Biganzoli, Giancarlo Bisagni, Livio Blasi, Cristina Capello, Rita Chiari, Alessia D’Alonzo, Michelino De Laurentiis, Angela Denaro, Alessandra Fabi, Daniele Farci

TL;DR
This study examines how changes in breast cancer molecular subtypes at relapse affect patient survival, emphasizing the importance of re-biopsy for treatment decisions.
Contribution
The study provides new insights into the clinical relevance of molecular subtype changes in metastatic breast cancer patients.
Findings
No significant differences in DFS, PFS, or OS were found between patients with or without molecular subtype changes.
Post-progression survival from first-line treatment varied between the two groups.
Receptor discordance between primary tumors and metastases was confirmed, highlighting the need for re-biopsy.
Abstract
Breast cancer is one of the most common oncological diseases among women in western countries and Italy as well. GIM 13-AMBRA is a patient journey study regarding how the prognosis of metastatic breast cancer patients can change according to the change in molecular subtype at relapse. Introduction: The treatment of MBC patients is guided by receptor status, with re-biopsy at relapse recommended to reassess hormone receptor (HR) status. Various treatment options are available for HER2-veMBC, including CDK4/6 inhibitors, PARP inhibitors, and checkpoint inhibitors. The study highlights the importance of determining receptor subtype for guiding treatment choices. Patients and Methods: The GIM 13 AMBRA study is a longitudinal cohort study involving 42 centers in Italy. It includes data from 939 HER2- MBC patients enrolled between May 2015 and September 2020. The study analyzes the impact of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
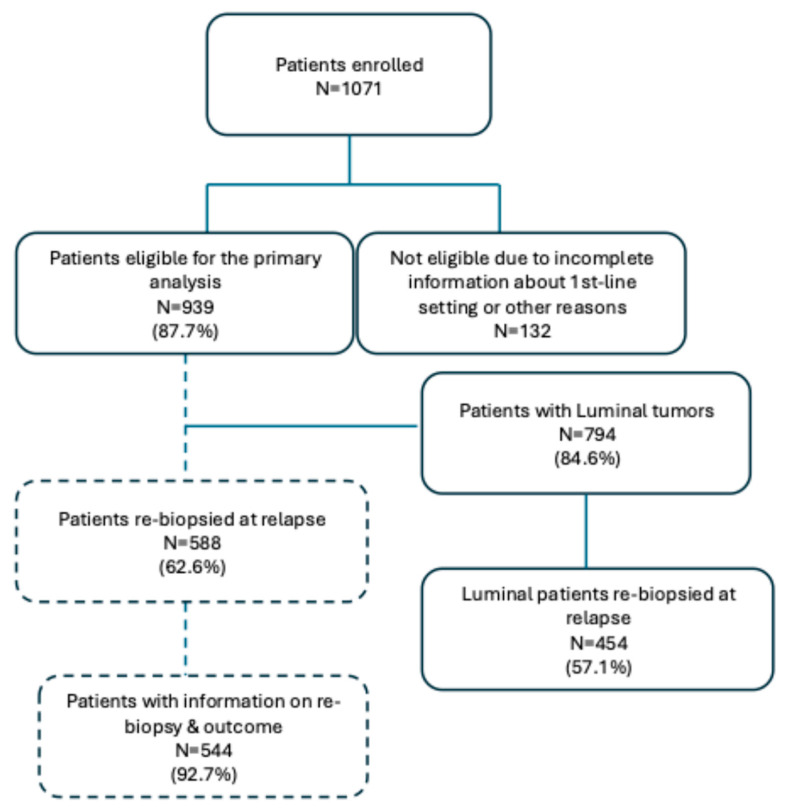 Figure 1
Figure 1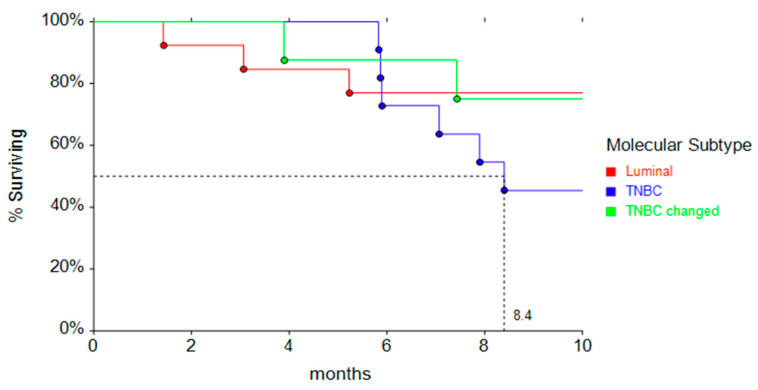 Figure 2
Figure 2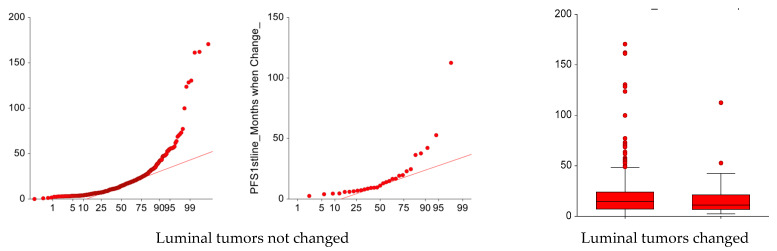 Figure 3
Figure 3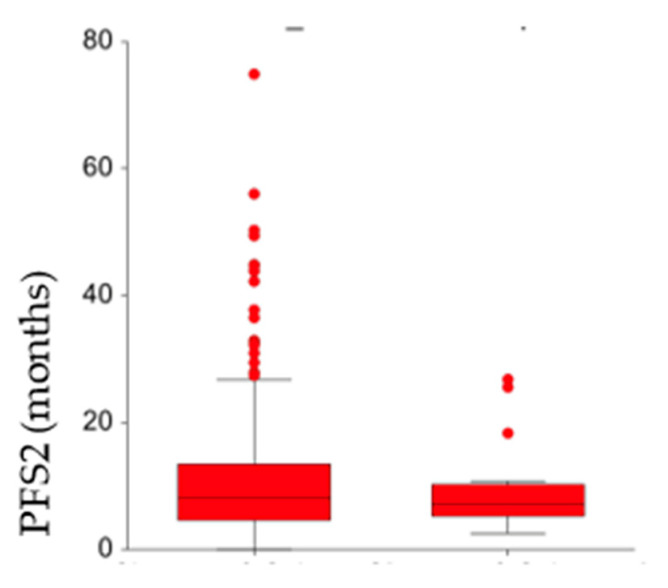 Figure 4
Figure 4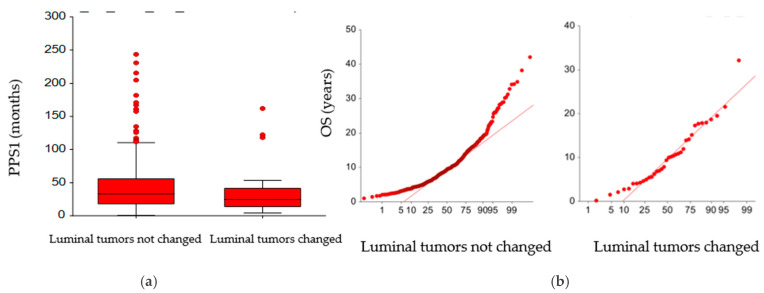 Figure 5
Figure 5- —Gruppo Italiano Mammella (GIM)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Breast Cancer Therapies · Breast Cancer Treatment Studies · HER2/EGFR in Cancer Research
1. Introduction
Breast cancer (BC) remains the leading cause of cancer death among women worldwide [1]. In Italy, 55,000 new diagnosed cases per year and 13,000 deaths have been recorded [2]. Despite the great progress achieved in the treatment of the primary tumor, about 30% of breast patients are destined to develop distant metastases [3]. Among the most important factors associated with disease recurrence and overall survival, nodal involvement, hormone receptor status, Human Epidermal growth factor receptor-2 (HER2) expression and proliferation index play key roles [4]. The clinical course of metastatic breast cancer (MBC) is very heterogeneous in terms of growth rate and response to systemic therapies; however, medical treatments remain a palliative cure. Median survival is about 2 years for some subtypes. Treatment of metastatic breast cancer (MBC) patients is mostly based on the receptor status [5], independently of the setting (adjuvant vs. metastatic) and the line of therapy. In Human Epidermal growth factor Receptor 2-negative (HER2-) patients, a first biopsy at the time of relapse is strongly recommended to reassess hormone receptor status, especially in HR+, considering the wide choice of multiple therapeutic agents [6]. If the determination of hormone receptors (estrogen receptor—ER and progesterone receptor—PR) in the primary tumor is clinically essential to define breast cancer subtypes, clinical outcome and the choice of treatment, a redefinition of HR status as well of HER2 status in the metastatic setting can be useful to refine the choice and is now mandatory to allow patients access to some drugs [7]. Liquid biopsy, a recent technique which allows identification of fragments of tumor cells or DNA circulating in the blood [7,8] has replaced tissue biopsy for detection of gene mutations; however, the latter method remains fundamental to reassessing HR and HER2 status.
Retrospective and prospective studies suggest that there is substantial discordance in receptor status between primary and recurrent breast cancer. Despite this evidence and current recommendations, the acquisition of tissue from metastatic deposits is not routine practice everywhere. Therefore, therapeutic decisions for treatment in the metastatic setting are based on the features of the primary tumor. Reasons for this attitude include the invasiveness of the procedure and the unreliable outcome of biopsy, in particular for biopsies of lesions at complex visceral sites.
In recent years, various treatment options have become available for HER2- MBC. In the first-line setting, these options have included Cycline-Dependent Kinases 4/6 inhibitors (CDK4/6i) in combination with aromatase inhibitors or tamoxifen for HR+ patients, [9,10,11,12], PARP inhibitors for patients with BRCA1/2 mutations [13,14], and checkpoint inhibitors for PD-L1-positive triple-negative disease (TNBC) [15]. Following these developments, it has become increasingly important to determine the receptor subtype of the tumor in guiding systemic treatment choices, even in second- and further-line settings due to the potential changes in HR and HER2 expression between primary tumor and metastatic sites, or before and after a first- or second-line treatment. A recent meta-analysis, including 39 prospective and retrospective studies found discordance rates in terms of estrogen receptor (ER), progesterone receptor (PR), and HER2 status between primary breast tumor and loco-regional or distant recurrences of 19% for ER, 31% for PR, and 10% for HER2 [16]. In terms of clinical implications, a change in receptor subtype often leads to an adjustment in the treatment strategy, which can also translate into different outcomes, as different authors have reported [17]. The GIM 13—AMBRA study is a longitudinal, cohort study aiming to describe therapeutic choices in HER2- MBC in the Italian real-life setting. The main objectives of the GIM 13-AMBRA study have been previously described [18] and are described here briefly. They include the description of the strategies used as first, second or subsequent lines of treatment in patients receiving at least one chemotherapy line (CHT), and the evaluation of possible correlations between the choice of treatment (both in the adjuvant phase and for metastatic disease) and patient characteristics (age, menopausal status, comorbidities), as well as the evaluation of adherence to the literature recommendations for therapeutic sequences in the clinical practice. Here, we report data regarding the impact of molecular subtype changes (lack of hormone receptors at the first biopsy for metastatic disease) on clinical outcomes, on real-word outcomes progression-free survival (rwPFS), time to treatment change (TTC) and overall survival (OS).
2. Patients and Methods
2.1. Study Design
The GIM 13 AMBRA is a longitudinal cohort study, which has collected data of the first 50 consecutive HER2- MBC patients, who started a first-, second- or subsequent line CHT between January 2012 and December 2016 at 42 centers in Italy. As the type of treatment can vary according to different factors, i.e., the presence of clinical trials, or the availability of in-house services like pathology, the centers have been selected from the 192 national Oncological Centers listed in the “Libro Bianco 2012 of the Italian Association of Medical Oncology—AIOM), according to the hospital type (Cancer Center, University Hospital or General hospital) and geographical distribution. This selection ensured that the data collected were representative of the Italian situation. The inclusion criteria were as follows: age ≥ 18 years; patients with HER2-negative metastatic breast cancer (Stage IV) who have received or not received endocrine therapy for metastatic disease and were candidates for first-line chemotherapy treatment in the years 2014–2016 (prospective cohort), or who have received first, second, or subsequent lines of chemotherapy for metastatic disease in the years 2012–2013 (retrospective cohort); availability of all information required by the study, including histology, hormone receptor status, grading, stage of disease at diagnosis, type of surgery for the primary tumor, type of adjuvant therapy (chemo- or hormone therapy), type of drug received as adjuvant therapy, date and site of relapse, type of treatment received for the first/second/third line of treatment of metastatic disease (chemo- or hormone therapy), type of chemotherapy regimen used and details of the drugs, date and site of disease progression; and able to provide written informed consent. The exclusion criteria included the following: metastatic disease at diagnosis, HER2-positive status, and participation in clinical trials. All the centers were authorized by their ethical committees (ECs), after the approval of the Coordinating Center Ethical Committee (Comitato Etico Brianza, approved 27 November 2014, Authorization N.1831).
2.2. Objectives
The primary objective of the main study was to describe the strategies in terms of first, second and subsequent lines of treatment in patients receiving at least one chemotherapy line (CHT) and the relative outcome parameters of 939 HER2-ve MBC patients. Taxanes-based regimens, w/o targeted agents, were the preferred first choice in both Luminal (30.2%) and TNBC (33.3%) patients. Briefly, the median PFS1 was 12.5 months (95% CI: 16.79–19.64), without any significant difference according to subtypes, while PFS2 was significantly shorter in TNBC patients (5.5 months, 95% CI: 4.3–6.5 vs. Luminal A—9.4, 95% CI: 8.1–10.7, and Luminal B—7.7 95% CI: 6.8–8.2, F-Ratio 4.30, p = 0.014). [13]. In the present analysis, we report the data regarding the impact of HR expression change or not measured at the first biopsy performed at relapse on the main outcome parameters in HR+/HER2- tumors.
2.3. Statistical Analysis
The clinical outcomes were real-world progression-free survival at first- (rwPFS1) or second-line treatment (rwPFS2), defined as the time between first/second-line therapy start and time to progression, according to investigator, or censored to date of latest news; time to treatment change of first- (TTC1) or second-line (TTC2) therapy, defined as the time between the start date, declared by the investigator, of first- or second-line treatment and the date, not defined a priori due to the observational design of the study, of the subsequent therapy start. The variables were analyzed in the different groups of patients according to whether the hormone receptor status changed at relapse. Normal probability plots have been used to identify substantive deviations from original evolution. This includes identifying outliers, skewness, kurtosis, the need for transformations, and mixtures. Analyses were carried out using NCSS^®^ 12 statistical Software 2018 (Kaysville, UT, USA). Continuous variables were evaluated with descriptive statistics (including number of patients, mean, standard deviation, median, minimum, 25th and 75th percentiles, maximum). Categorical variables were evaluated with frequency and percentage. Tumor subtypes were defined according to the definition provided by Prat et al. [19].
3. Results
Patients’ and Tumor Characteristics at First Relapse
Between May 2015 and September 2020, 1071 patients were enrolled in the main study, of whom 132 (12.3%) were not considered eligible due to (1) incomplete information about first-line treatment, and (2) other reasons, leaving a total of 939 (Luminal N = 794; TNBC, N = 145) evaluable patients for the main analysis. The demographic characteristics have been described in our previous paper. Briefly, median age at primary tumor diagnosis was 51.9 years (range 50.6–52.9), and most of the patients received adjuvant CHT (71.8%), mainly a combination of anthracycline + taxanes (305, 31.5%), or anthracycline + other drugs (266, 28.3%). Re-biopsy at relapse was performed in 588 out of 939 patients (62.6%) (Figure 1).
Percentages of tumors rebiopsed at relapse did not significantly differ according to the molecular subtype at primary diagnosis. More than 60% of the relapsed patients were retested for HR status at relapse. The details are reported in Table 1.
A total of 4 tumors (7.5%) among those rebiopsied changed their molecular category at relapse: among the Luminal tumors, 2 Luminal A became Luminal B and 31 became TNBC. Conversely, 11 TNBC tumors acquired a Luminal subtype at relapse. We did not collect data regarding change in HER2 status as all the patients enrolled were HER2-ve at the primary site. As previously declared and considering the occasional change into Luminal subtype occurring in TNBC tumors, as well as the unknown clinical relevance of this event, we report here outcome data only for Luminal tumors.
Five-hundred eighty-eight patients were retested for HR status determination at relapse; the 488 Luminal patients (134, 27.5%%) were treated with endocrine treatment in the adjuvant setting, either alone (134, 27.5%) or after chemotherapy (326, 66.8%), while the remaining were treated with chemotherapy alone (28, 5.7%%).
Most of the rebiopsied patients showed relapse at visceral sites (161, 32.9%) and bone (26.6%), as the non-rebiopsed one (visceral: 163, 46.4%; bone: 140, 39.9%. The majority of patients in both groups were treated with endocrine treatment at relapse, alone or sequenced after chemotherapy. Table 2 summarizes the type of treatments at relapse in retested and non-retested Luminal patients. Conversely, 11 TNBC tumors at primary acquired a Luminal profile at relapse: all patients but two were treated with chemotherapy, mainly a combination of Taxane + Bevacizumab.
No difference in terms of median disease-free survival (DFS) was observed in Luminal tumors according to the change in molecular subtype in comparison to tumors which did not change (Luminal: 74.6 months, 95% CI: 66.8–82.1 vs. Luminal becoming TNBC: 89.7 months, 95% CI: 44.7–103.5). Type of treatment was not significantly different between tumors with changed molecular subtype at relapse and tumors without change, as shown in Table 3.
Conversely, 11 TNBC patients changed their molecular subtype, becoming Luminal at relapse. The median PFS1 in these patients is very similar to that observed in Luminal ones at primary (Figure 2).
Chemotherapy, alone or sequenced by ET, remained the most administered treatment, independently of the molecular subtype change or not.
Subtype change did not significantly affect the main progression outcomes: no difference in median PFS1 was observed between the Luminal tumors which remain as such (14.4 months, 95% CI: 12.4–16) and those that changed into TNBC subtype (11.1 months, 95% CI: 7.2–16.8; p = 0.36) (Figure 3).
For the two groups, the median PFS2 was 8.1 months (95% CI: 7.3–9.2) and 7.1 months (95% CI: 5.3–9.1), respectively, (p = 0.59) (Figure 4).
Only median post-progression survival from first line treatment (PPS1) was different in the two groups (33.1 months, 95% CI: 30.1–36.6 vs. 24 months (95% CI: 15.8–30.9; p = 0.031) (Figure 5a), while no difference in median OS was observed between the two groups according to the change in molecular subtype (9.4 years, 95% CI: 8.7–9.8 vs. 9.7 years, 95% CI: 5.6–11.2) (Figure 5b).
4. Discussion
Discordance in ER, PgR and HER2 status between primary breast tumors and metastases is a well-known phenomenon, previously described by many authors and analyzed in different, even small, series [15,16]. However, the magnitude of this change in affecting patients’ management and survival outcomes remains important for defining therapeutic strategies, particularly in Luminal patients. The GIM 13-AMBRA study is a cohort, real-world study which collected data from more than 900 HER2- metastatic breast cancer patients in Italy from diagnosis until death, or data censoring, and so far, represents a priceless opportunity to collect insights useful for future trials. ESMO guidelines [2] strongly support the practice of having a biopsy for patients with recurrent MBC to confirm histology and to reassess ER, PgR and HER2 status. Among the 939 patients registered into the study, 588 (62.6%) were rebiopsied at first relapse, without any difference among Luminal A, Luminal B and TNBC patients. In a large retrospective study, Meegdes et al. [20] conducted a large real-world study which included all patients diagnosed with MBC between 2007 and 2018 in seven hospitals in the southeast Netherlands and registered in the SONABRE registry, with the aim of assessing the biopsy rate and the factors associated with taking a biopsy of a metastatic site at MBC diagnosis. Interestingly, they found that 60% of patients had a biopsy of a metastatic site at presentation, and the decision to have a biopsy was higher in academic hospitals (73%), in comparison to teaching hospitals (60%) and non-teaching hospitals (59%). The authors also found that a more recent period of MBC diagnosis was associated with a higher biopsy rate: 67% in 2016–2018 compared with 51% in 2007–2009 (OR = 2.14; 95% CI: 1.70–2.70). They also found that biopsy was performed more frequently in younger patients in comparison to older ones (56–75 years vs. >75 years: OR = 1.80; 95% CI: 1.48–2.19; ≤55 years vs. >75 years: OR = 2.20; 95% CI: 1.74–2.78)
The percentage of re-biopsies performed in our study is among the highest, if compared with also those reported in other retrospective studies, the largest one being the ESME database [16]. Grinda et al. reported that re-biopsy was performed in 17.6% of the 16,703 patients included in the ESME database.
In our analysis, a total of 49 tumors (9.1%) among those rebiopsied changed their molecular category at relapse: 36 Luminal A or Luminal B tumors became TNBC (7.9%), and 13 TNBC became Luminal B (13%). Discordance rates between primary and metastases greatly varies according to the different series, strongly depending on the size of population analyzed. Meegdes et al. reported an overall receptor discordance rate of 18%; discordance rates were 13% for HR+/HER2- and 12% for TNBC. Mellouli et al. [21] collected data on 68 BC patients at a single-center in a retrospective study, reporting a discordance in ER status in 20 patients (29.4%, p = 0.041), with ER-negative conversion in 15 patients (22%) and ER-positive conversion in 5 patients (7.3%). They observed a difference in PR status in 27 of the cases (39.7%, p = 0.001): in 24 of the patients (35.2%), the PR status had changed from positive in PBC to negative in metastatic lesions, while in 3 of the patients (4.4%), the PR status had changed from negative to positive. HR status conversion was detected in 20 cases (29.4%, p = 0.04): 15 patients (22%) had changed from HR-positive status in primary breast cancer to HR-negative status in the metastatic tissues, and 5 patients (7.35%) from HR-negative to HR-positive. In the ESME cohort [22], one of the most important analyses ever conducted in a large population, regarding the discordance rate in HR expression between the primary site and the metastatic ones, Grind et al. reported a change rate for HR status of 14.2% [95% CI: 12.5–16.0], with expression loss in 72.5% and expression gain in 27.5%. For ER status, 15.1% [95% CI: 13.3–17.0] of cases showed a change with loss in 67.7% and gain in 32.3%. For PR status, a modification was observed in 31.1% [95% CI: 28.7–33.5] with loss in 75.3% and gain in 24.7%. To date, our results in terms of percentages of discordance between primary and metastases are in the middle of those reported by other authors [17], and this can be explained in part by the absence of a central review, as often happens in real-world studies, as well the unavailability of information regarding the site where the biopsy was taken. Other authors have thus showed that among the factors associated with HR discordance, there were metastases to bone only and primary tumor treatments with endocrine therapy [22].
The clinical meaning of discordance and, moreover, the impact in terms of treatment choice remains a matter of debate. In our analysis, we evaluated outcomes (rwPFS1, rwPFS2, PPS1 and OS) of 454 out of 490 rebiopsied Luminal patients, finding no differences in rwPFS1, rwPFS2 and OS. Differences among the various series remain wide, indicating there is probably the need for larger, prospective trials. Schwieger et al. [18] recently reported that the change from an ER or PgR+/HER2− at primary tumor to TNBC paired metastatic one was not associated with decreased survival (p > 0.05) in 258 analyzed patients. Similarly, Peng et al. [23] found no statistical difference in PFS according to the subtype of the recurrent or metastatic breast cancer (p > 0.05). In another retrospective study, Yang et al. [19] evaluated the frequency and the prognostic impact of changes in HR and HER2 between primary and recurrent/metastatic lesions in 133 patients: in their population, the ER-discordant cases and ER-loss cases experienced a worse overall survival (OS) (p = 0.001 and p = 0.016, respectively) and post-recurrence survival (PRS) (p = 0.001 and p = 0.018, respectively), compared with the respective concordant cases.
Testing for HER2 status is also important in that ~10% of HER2 status can change, including changing from negative to positive, due to clonal selection over time and therapeutic selection pressure. HER2 was not retested in our study, and we unfortunately do not know how often this occurred in this cohort, which is one of the limitations of our study.
In the contemporary era, the treatment choice for HR+ BC which do not change hormone receptor expression from primary to metastases and for those which change into TNBC can significantly differ, both in terms of drugs, as well as in terms of additional molecular tests. For example, first-line treatment of TNBC patients is largely guided by the expression of programmed-death ligand 1 (PDL-1), while HR+ tumors may derive a benefit from more personalized approaches based on the detection of ESR1, AKT or PIK3CA mutations.
In recent years, different trials have evaluated the role of specific targeted agents, like elacestrant [7], imlunestrant [24], or inavolisib [25], as second-line treatment in advanced Luminal cancers, with the aim of delaying the use of chemotherapy. Overall, these trials demonstrated that, in the presence of specific gene mutations, they are highly efficacious in disease control. Nevertheless, most of them have been studied in patients who have been treated with CDK 4/6 inhibitors as first-line therapy and have received at least one prior chemotherapy line of treatment. Moreover, nothing is known about those patients excluded from enrollment in these trials and perhaps treated with chemotherapy.
Based on the evidence presented so far, when and how should we biopsy our metastatic patients? The availability of liquid biopsy, a technique which allows detection of breast cancer cell mutations in different organic fluids, mainly blood and urine, has revolutionized the approach to MBC patient treatment as it is easier to perform than tissue biopsies and is virtually non-invasive to the patient. However, it is our opinion that tissue biopsy should remain mandatory to assess ER and PgR status as a first approach, followed by a potential subsequent use of liquid biopsy to detect mutations specific to the molecular subtype. Several questions remain open: For example, considering the high heterogeneity of breast cancers, should we test for PDL-1 expression those Luminal tumors which lost HR expression, becoming TNBC at the time of relapse? How much is a biopsy obtained from a single metastatic site representative of the whole disease? Regarding these and other questions, answers are becoming more and more important, considering the high costs of the new drugs and, above all, the different safety profiles of the various drugs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H. Ferlay J. Siegel R.L. Laversanne M. Soerjomataram I. Jemal A. Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA A Cancer J. Clin.20217120924910.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Cos’è il Cancro|AIRC Available online: https://www.airc.it/cancro/informazioni-tumori/cose-il-cancro/numeri-del-cancro(accessed on 4 April 2025)
- 3Sørlie T. Perou C.M. Tibshirani R. Aas T. Geisler S. Johnsen H. Hastie T. Eisen M.B. Van De Rijn M. Jeffrey S.S. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications Proc. Natl. Acad. Sci. USA 200198108691087410.1073/pnas.19136709811553815 PMC 58566 · doi ↗ · pubmed ↗
- 4Allison K.H. Prognostic and predictive parameters in breast pathology: A pathologist’s primer Mod. Pathol.2021349410610.1038/s 41379-020-00704-733154551 · doi ↗ · pubmed ↗
- 5Curigliano G. Burstein H.J. Winer E.P. Gnant M. Dubsky P. Loibl S. Colleoni M. Regan M.M. Piccart-Gebhart M. Senn H.J. De-escalating and escalating treatments for early-stage breast cancer: The St. Gallen International Expert Consensus Conference on the Primary Therapy of Early Breast Cancer 2017 Ann. Oncol.2017281700171210.1093/annonc/mdx 30828838210 PMC 6246241 · doi ↗ · pubmed ↗
- 6Gennari A. AndréF. Barrios C.H. Cortes J. de Azambuja E. De Michele A. Dent R. Fenlon D. Gligorov J. Hurvitz S.A. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer 5 behalf of the ESMO Guidelines Committee Ann. Oncol.2021321475149510.1016/j.annonc.2021.09.01934678411 · doi ↗ · pubmed ↗
- 7Bidard F.C. Kaklamani V.G. Neven P. Streich G. Montero A.J. Forget F. Mouret-Reynier M.A. Sohn J.H. Taylor D. Harnden K.K. Elacestrant (oral selective estrogen receptor degrader) Versus Standard Endocrine Therapy for Estrogen Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Advanced Breast Cancer: Results From the Randomized Phase III EMERALD Trial J. Clin. Oncol.2022403246325610.1200/JCO.22.0033835584336 PMC 9553388 · doi ↗ · pubmed ↗
- 8Mazzeo R. Sears J. Palmero L. Bolzonello S. Davis A.A. Gerratana L. Puglisi F. Liquid biopsy in triple-negative breast cancer: Unlocking the potential of precision oncology ESMO Open 2024910370010.1016/j.esmoop.2024.10370039288656 PMC 11421323 · doi ↗ · pubmed ↗