Molecular and Pathological Heterogeneity of Synchronous Small and Large Duct Intrahepatic Cholangiocarcinoma—A Case Series
Savelina Popovska, Vladislav Nankov, Boriana Ilcheva, George Dimitrov

TL;DR
This study examines the differences between two types of liver cancer, showing they have distinct genetic and clinical features that require personalized treatment approaches.
Contribution
The study identifies distinct molecular and pathological profiles of synchronous small- and large-duct intrahepatic cholangiocarcinoma and their clinical implications.
Findings
Small-duct iCCA is linked to IDH1/2 mutations and FGFR2 fusions with better progression-free survival.
Large-duct iCCA shows KRAS, TP53, and NF1 mutations with aggressive behavior and lower survival rates.
Some large-duct cases show TMB-H and MSI-H, suggesting potential for immune checkpoint inhibitors.
Abstract
Background: Synchronous small- and large-duct intrahepatic cholangiocarcinoma (iCCA) represents a rare and heterogeneous entity, posing challenges for diagnosis, prognosis, and treatment selection. The pathological and molecular diversity between these subtypes influences tumor behavior and therapeutic response, necessitating a personalized approach. This study investigates the molecular and pathological heterogeneity of synchronous iCCA and its clinical implications. Methods: This prospective case series included six patients diagnosed with synchronous small- and large-duct iCCA at the Military Medical Academy, Sofia, between January 2023 and January 2025, with a median follow-up of 15 months. Tumor classification was based on histopathological examination, immunohistochemical analysis, and next-generation sequencing (NGS)-based genomic profiling. Radiological and clinical data were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
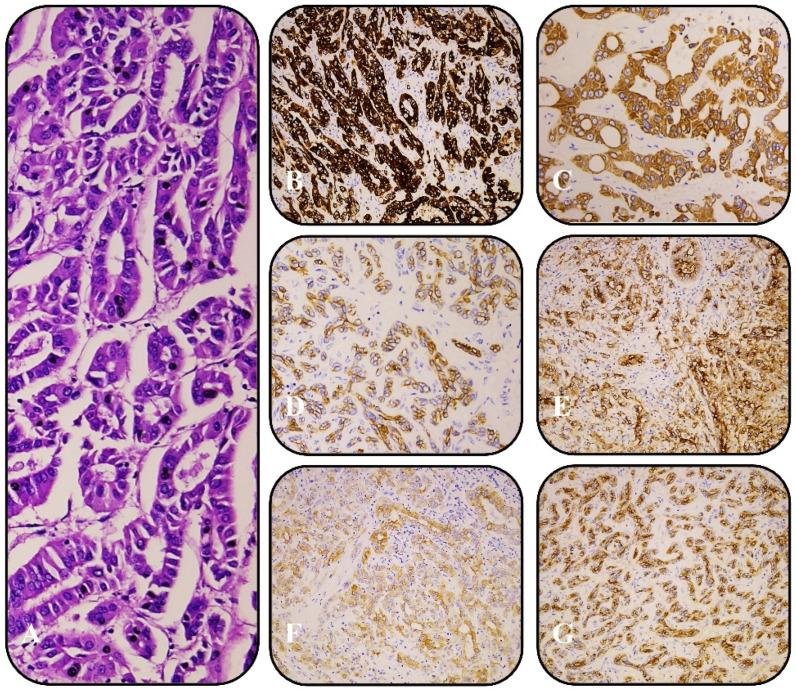 Figure 1
Figure 1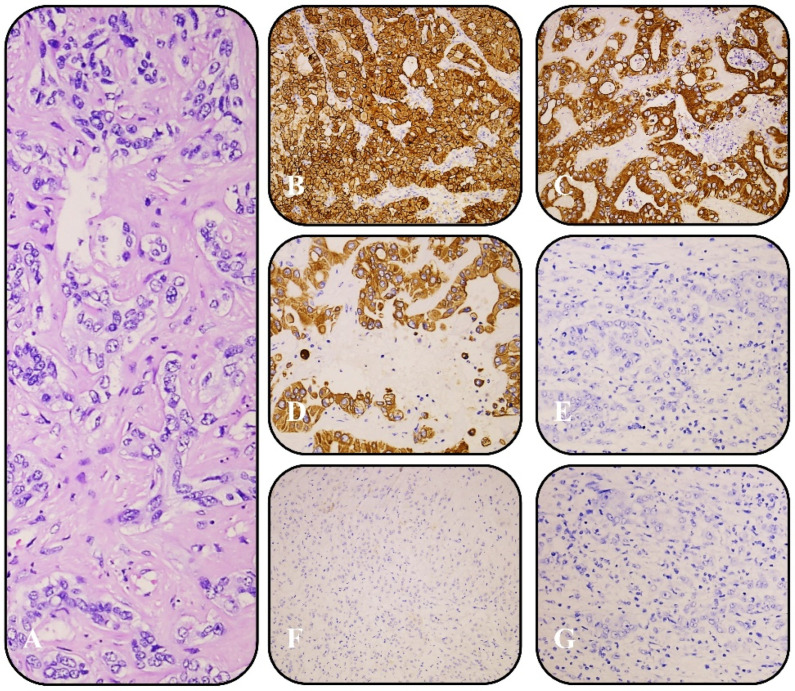 Figure 2
Figure 2- —PRIDST 2021–2027
- —EU
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Genetic factors in colorectal cancer · Pancreatic and Hepatic Oncology Research
1. Introduction
Intrahepatic cholangiocarcinoma (iCCA) is a rare primary liver malignancy that exhibits significant histological and molecular heterogeneity. It is traditionally classified into small-duct and large-duct subtypes, which differ in their molecular landscape, histopathology, clinical behavior, and therapeutic response [1]. However, an emerging subset of cases presents with synchronous small-duct and large-duct iCCA, where both subtypes coexist within the same tumor or patient, further complicating classification and treatment strategies [2].
Small-duct iCCA arises from the peripheral bile ducts and is characterized by a mass-forming growth pattern, non-mucin-producing cuboidal cells, and frequent association with chronic liver diseases, including hepatitis B or C and non-alcoholic fatty liver disease [3]. This subtype is commonly driven by IDH1/2 mutations, FGFR2 fusions, and BAP1 alterations, which provide opportunities for targeted therapy [4]. In contrast, large-duct iCCA originates from larger bile ducts and exhibits an infiltrative, duct-forming growth pattern with mucin-producing columnar cells and a dense fibrotic stroma. It is often associated with primary sclerosing cholangitis and liver fluke infections and is molecularly characterized by KRAS, SMAD4, and TP53 mutations [5].
Molecular profiling has revealed that these subtypes respond differently to therapy. Small-duct iCCA is frequently sensitive to IDH inhibitors and FGFR inhibitors [6,7], while large-duct iCCA, due to KRAS-driven oncogenesis and an immunosuppressive tumor microenvironment, remains more resistant to targeted therapies [8,9]. Furthermore, large-duct iCCA is generally more aggressive, with a higher incidence of lymph node metastasis, vascular invasion, and postoperative recurrence, leading to poorer overall survival compared to small-duct iCCA [10,11].
The presence of synchronous small-duct and large-duct iCCA within the same tumor or patient raises important questions about tumor evolution, molecular crosstalk, and treatment resistance mechanisms. Histopathological examination and immunohistochemical staining can confirm the coexistence of these subtypes, and recent studies suggest that they may exhibit distinct genetic alterations, reinforcing their biological differences [2]. However, molecular and clinical overlaps exist, complicating subclassification and therapeutic decision-making [12].
This case-series aims to analyze the molecular heterogeneity between synchronous small-duct and large-duct iCCA, correlating genomic alterations with histopathology and clinical outcomes.
2. Materials and Methods
2.1. Study Design and Patient Selection
This single-center prospective case series examines the molecular and pathological heterogeneity of synchronous small-duct and large-duct intrahepatic cholangiocarcinoma (iCCA). Among 87 patients diagnosed with iCCA, 6 cases with histopathologically confirmed synchronous small- and large-duct components were prospectively included at the Military Medical Academy, Sofia, between January 2023 and January 2025, with a median follow-up of 15 months.
For the purpose of this study, the term “synchronous small- and large-duct intrahepatic cholangiocarcinoma” was used to define cases in which both histologically distinct subtypes—small-duct and large-duct—were diagnosed concurrently, either within the same tumor in spatially distinct regions or in separate intrahepatic lesions. This classification was based on the identification of two morphologically and immunophenotypically distinct components, each displaying characteristic features consistent with established criteria for small-duct or large-duct iCCA. In contrast, “mixed small- and large-duct iCCA” typically refers to tumors with intermingled or overlapping histological features, where the two subtypes cannot be clearly separated. In this study, only cases with clearly distinguishable and co-existing subtypes were included under the definition of synchronous iCCA.
Diagnosis was established through histopathological evaluation and comprehensive genomic profiling, following the World Health Organization (WHO) tumor classification system, to assess the molecular and clinical significance of these distinct subtypes [13].
Patients were eligible if they had a histologically confirmed diagnosis of synchronous small-duct and large-duct iCCA, identified within the same tumor or at different intrahepatic sites. Tumor classification was based on morphological, immunohistochemical, and molecular criteria, ensuring accurate subclassification. Inclusion required sufficient tumor tissue for immunohistochemical staining and next-generation sequencing (NGS)-based genomic analysis. Patients were excluded if they exhibited only a single histological subtype or had undergone systemic therapy before resection, which could introduce confounding molecular alterations. Cases with insufficient tumor material for genomic sequencing were also excluded.
2.2. Histopathological and Immunohistochemical Analysis
Tumor specimens were obtained from surgical resections and were formalin-fixed and paraffin-embedded (FFPE) for histopathological and immunohistochemical analysis. Hematoxylin and eosin (H&E) staining was performed to classify tumors into small-duct and large-duct subtypes.
Small-duct iCCA was defined by non-mucin-producing cuboidal epithelial cells, duct-like structures, and a mass-forming growth pattern. In contrast, large-duct iCCA was identified by mucin-producing columnar cells, a duct-forming architecture, and a dense desmoplastic stroma. Cases with a mixed morphology were carefully evaluated to confirm the presence of both subtypes within the same tumor or different intrahepatic regions. The predominant component was defined as the histological subtype, occupying more than 50% of the tumor mass, as assessed on H&E-stained slides at x10 magnification. Radiological features were used to support the classification [14].
Immunohistochemistry (IHC) was performed on all cases to characterize tumor subtypes and distinguish iCCA from hepatocellular carcinoma. Small-duct iCCA typically exhibited strong positivity for CK7 (clone RNS, Leica/BOND), CK19 (clone D170, Leica/BOND), and EMA (clone GP1.4, Leica/BOND) (Figure 1), while large-duct iCCA was positive for CK7, CK19, EMA, MOC-31 (clone MOC31, Biocare/BOND), S100P, and Villin (clone 1d2C3, DAKO) (Figure 2). Additional markers, including HepPar-1 (clone OCH1E5, Leica/BOND), Arginase-1, and Glypican-3 (clone 1G12, Leica/BOND), were used to exclude hepatocellular carcinoma. Staining was performed on the Leica BOND and DAKO platforms using pre-diluted, ready-to-use antibodies according to the manufacturers’ protocols. The intensity and percentage of positive tumor cells were assessed by two independent pathologists to ensure diagnostic accuracy and reproducibility.
2.3. Molecular Profiling and Genomic Analysis
Comprehensive genomic profiling was conducted using TruSight™ Oncology 500 (Illumina, San Diego, CA, USA), a hybrid capture-based NGS panel covering 523 cancer-associated genes. DNA and RNA were co-extracted from FFPE tumor samples using the AllPrep^®^ DNA/RNA FFPE Kit (Qiagen, Hilden, Germany). The concentration and quality of the DNA isolates were assessed with the Qubit™ dsDNA HS Assay Kit (Invitrogen, Carlsbad, CA, USA) and the Infinium HD FFPE QC Assay Kit (Illumina, San Diego, CA, USA), respectively. RNA quantification was carried out with the Qubit™ RNA HS Assay Kit (Invitrogen, Carlsbad, CA, USA). Genomic DNA (gDNA) was sheared using a Covaris M220 Focused-ultrasonicator (Covaris, Woburn, MA, USA) in accordance with the manufacturer’s instructions. Libraries were sequenced on a NextSeq 550 instrument (Illumina, San Diego, CA, USA) to assess single nucleotide variants (SNVs), copy number variations (CNVs), structural rearrangements, gene fusions, and gene signatures [tumor mutational burden (TMB) and microsatellite instability (MSI)].
The genomic analysis focused on key alterations associated with cholangiocarcinoma, including IDH1/2, FGFR2, KRAS, TP53, BAP1, NF1, MYCN, BRCA2, and ARID1A mutations. TMB was quantified as the number of somatic mutations per megabase (mut/Mb), and MSI status was determined using an NGS-based MSI assay. Variants were classified according to clinical significance using OncoKB guidelines, where Tier I alterations were those with established clinical utility for targeted therapies, Tier II mutations were considered potentially actionable, and Tier III alterations were of uncertain significance [15].
2.4. Imaging Analysis and Clinical Correlation
All patients underwent contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI) to evaluate tumor morphology, vascular invasion, and intrahepatic tumor distribution. Radiological features were analyzed to assess correlations between tumor growth patterns, molecular alterations, and histopathological classification.
Small-duct iCCA predominantly appeared as a well-defined, mass-forming lesion, whereas large-duct iCCA was more frequently associated with periductal infiltrative growth, biliary obstruction, and a dense fibrotic response. Imaging findings were compared with genomic alterations to identify potential associations between tumor morphology and molecular heterogeneity.
Clinical records were reviewed for tumor staging (TNM classification 8^th^ edition), treatment history, and response to therapy. Follow-up data, where available, were analyzed to assess disease progression and survival outcomes, providing insight into the prognostic differences between synchronous small- and large-duct iCCA. Patients received treatment according to ESMO guideline recommendations [16], based on their respective eligibility criteria.
2.5. Statistical Analysis
Descriptive statistics were used to summarize histopathological, molecular, radiological, and clinical data. Continuous variables, such as age and progression-free survival (PFS), were reported as medians with interquartile ranges (IQRs). Categorical variables, including histological subtype and molecular alterations, were presented as frequencies and percentages.
2.6. Ethical Considerations
This study was approved by the Institutional Ethics Board of the Military Medical Academy, Sofia, and conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Written informed consent was obtained from all patients before participation, and data were anonymized to protect patient confidentiality.
3. Results
3.1. Patient Characteristics
Between January 2023 and January 2025, a total of 87 patients were diagnosed with iCCA at the Military Medical Academy, Sofia. Of these, 38 patients (43.7%) were classified as small-duct type, 43 (49.4%) as large-duct type, and 6 patients (6.9%) were identified as having synchronous small- and large-duct features based on histomorphology and immunohistochemistry. The median age at diagnosis was 72 years (range: 64–78 years), with a female predominance (5 out of 6 patients, 83%). In all cases, both histologically distinct components—small-duct and large-duct—were identified either within the same tumor or at separate intrahepatic sites, confirming the diagnosis of synchronous iCCA.
3.2. Histopathological and Immunohistochemical Findings
All six cases demonstrated distinct small-duct and large-duct histopathological features within the same tumor or different liver regions. Immunohistochemically, the large-duct component expressed CK7, CK19, EMA, MOC-31, S100P, and Villin, while the small-duct component was positive for CK7, CK19, and EMA.
3.3. Genomic Alterations and Molecular Heterogeneity
NGS revealed distinct mutational landscapes in the synchronous small-duct and large-duct components within the same patient (Table 1). Small-duct iCCA was frequently associated with IDH1/2 mutations (2/3 cases, 66%) and FGFR2 fusions (1/3 cases, 33%), supporting its previously established molecular profile. Additionally, BAP1 mutations (1/3 cases, 33%) and MYCN amplifications (1/3 cases, 33%) were observed in small-duct iCCA, potentially indicating alternative oncogenic pathways. Large-duct iCCA exhibited a higher frequency of KRAS mutations (2/3 cases, 66%), TP53 mutations (1/3 cases, 33%), and NF1 alterations (1/3 cases, 33%), consistent with a more aggressive molecular phenotype. Tumor mutational burden (TMB) varied significantly between subtypes, with large-duct iCCA generally exhibiting a higher TMB (range: 3.1–23.5 muts/Mb) compared to small-duct iCCA (range: 1.6–7.8 muts/Mb). One case of large-duct iCCA exhibited high microsatellite instability (MSI-H, 14.8%), suggesting potential sensitivity to immune checkpoint inhibitors, whereas small-duct iCCA cases were predominantly MSI-low (range: 2.3–3.2%).
3.4. Imaging and Clinical Correlation
Initial radiological evaluation revealed distinct imaging patterns between small-duct and large-duct components. In five of the six cases, imaging findings correlated well with histological classification: small-duct predominant cases presented with mass-forming lesions, while large-duct predominant tumors exhibited infiltrative or periductal growth patterns. However, one case showed discordant features—although the radiological appearance suggested a small-duct pattern, histological analysis revealed a predominance of large-duct morphology. Tumor staging varied across the cohort, with two patients classified as Stage II and four as Stage IIIB. Among the six patients included in our study, all underwent curative-intent surgical resection. Three received adjuvant chemotherapy with capecitabine due to high-risk features (i.e., nodal involvement, T4 stage), while the remaining three were managed with active surveillance.
Small-duct iCCA lesions were primarily well-defined, mass-forming tumors with minimal biliary involvement, whereas large-duct iCCA displayed periductal infiltrative growth, biliary obstruction, and vascular invasion. Biliary obstruction and periductal infiltration were exclusive to large-duct components, correlating with KRAS and TP53 mutations in this cohort. Small-duct iCCA tumors with FGFR2 fusions were more likely to present as well-circumscribed, mass-forming lesions without significant ductal involvement. In contrast, patients with MSI-H large-duct iCCA exhibited highly infiltrative tumor morphology, with extensive lymph node involvement. Clinical follow-up revealed worse prognostic outcomes in cases with predominant large-duct components, particularly those harboring KRAS, TP53, and NF1 mutations (Table 2).
4. Discussion
The management of synchronous small- and large-duct iCCA remains challenging due to its histopathological and high molecular heterogeneity. Treatment selection is largely determined by the predominant histological component, disease stage, and molecular profile. In this case series, patients with small-duct-predominant iCCA, particularly those harboring IDH1/2 mutations or FGFR2 fusions, exhibited longer progression-free survival (PFS), supporting the use of targeted therapies such as ivosidenib and pemigatinib, both of which are approved for advanced cholangiocarcinoma [16,17]. In contrast, large-duct-predominant iCCA, frequently associated with KRAS, TP53, and NF1 mutations, demonstrated more aggressive behavior, higher recurrence rates, and shorter PFS. The absence of approved KRAS-targeted therapies in cholangiocarcinoma limits treatment options to gemcitabine/cisplatin chemotherapy, though emerging strategies, including MEK and SHP2 inhibitors, are under investigation [18,19]. Notably, NF1-mutant large-duct iCCA exhibited particularly poor outcomes, suggesting that RAS/MAPK or PI3K inhibitors could be explored in future clinical trials.
Immunotherapy, in the context of precision oncology, has emerged as a promising option for a subset of cholangiocarcinoma patients, particularly those with high tumor mutational burden (TMB-H) or microsatellite instability-high (MSI-H) status. TMB, defined as the total number of mutations per megabase of DNA, serves as an agnostic predictive biomarker for immune checkpoint inhibitor (ICI) response. TMB-H (≥10 mutations/Mb) has been associated with improved outcomes in patients receiving pembrolizumab [20]. Similarly, MSI-H status, which results from deficient mismatch repair (dMMR) mechanisms, enhances tumor immunogenicity and response to ICIs [21]. In the context of iCCA, tumors with TMB-H and/or MSI-H status have demonstrated improved outcomes from ICI-based therapies [22]. Despite this evidence, ICIs remain inaccessible in Bulgaria for TMB-H/MSI-H cholangiocarcinoma due to a lack of reimbursement policies, limiting their real-world application.
In addition to targeted therapy and immunotherapy, systemic chemotherapy remains the cornerstone of treatment for advanced cholangiocarcinoma. First-line therapy consists of gemcitabine and cisplatin, often combined with durvalumab, as demonstrated in the TOPAZ-1 trial [23]. The trial showed that the addition of durvalumab to chemotherapy modestly improved overall survival (OS) and PFS, with a PFS benefit of 1.5 months and an OS improvement of 1.3 months over the control arm. However, subgroup analysis revealed significant benefit primarily in PD-L1-positive and Asian patients, who comprised the majority of the study cohort, raising concerns about the generalizability of these findings and the need for more stringent approval criteria based on biomarker selection. For second-line therapy, FOLFOX (5FU/folinic acid-oxaliplatin) has shown modest survival benefits, but prognosis remains poor, with median survival for advanced disease under one year [16,17].
A key limitation of our study is the relatively short median follow-up period of 15 months, which hinders the ability to make definitive conclusions regarding long-term outcomes. However, this limitation is inherent in the design of our prospective case series, which focuses on a rare iCCA variant within a single specialized center. Given the exceptional rarity of synchronous small- and large-duct iCCA, the current follow-up duration reflects the early phase of patient accrual. For context, the TOPAZ-1 trial, which established current systemic treatment standards, reported a median follow-up of only 23 months [23].
Molecular heterogeneity within individual tumors complicates treatment selection, highlighting the importance of multi-regional tumor sampling and comprehensive genomic profiling [24]. A one-size-fits-all approach is insufficient, as treating iCCA without accounting for the dominant molecular driver may lead to suboptimal therapeutic responses and unnecessary financial burden [25]. Identifying subtype-specific oncogenic drivers is crucial for selecting the most effective targeted therapies and minimizing unnecessary interventions.
Histopathological complexity remains a significant challenge in the diagnosis and treatment of synchronous iCCA. The coexistence of small- and large-duct components within the same tumor complicates classification, requiring detailed histological and immunohistochemical analysis [14]. Radiological growth patterns are often used as non-invasive surrogates for tumor subtype classification in iCCA [26]; however, our findings emphasize the limitations of relying solely on imaging. In five of the six cases, radiological features were concordant with the predominant histological subtype, with mass-forming lesions observed in small-duct iCCA and periductal-infiltrative patterns typical of large-duct disease. Nonetheless, one case demonstrated a discordance between radiological and histological findings, underscoring the potential for misclassification based on imaging alone. This reinforces the critical role of histopathological and immunohistochemical evaluation in accurately identifying the predominant tumor component, particularly in heterogeneous or borderline cases, and in guiding appropriate therapeutic decision-making.
Surgical management also differs between subtypes. Large-duct iCCA frequently requires extensive resection, including lymphadenectomy and biliary reconstruction, due to its higher propensity for lymph node metastasis and vascular invasion. In contrast, small-duct iCCA is often more localized and may be resected with limited hepatectomy [27]. Prognostically, small-duct iCCA is associated with better survival outcomes, whereas large-duct iCCA exhibits early recurrence and poor overall survival, reinforcing the need for subtype-specific treatment strategies [28].
5. Conclusions
This case series underscores the importance of a personalized, multidisciplinary approach to synchronous iCCA, integrating histopathological classification, molecular profiling, and precision therapy to optimize patient outcomes. Expanding access to ICIs for MSI-H and TMB-H cases could significantly improve treatment outcomes for selected patients. Future research should focus on adaptive treatment strategies tailored to tumor heterogeneity and dominant molecular drivers, ensuring that patients receive the most effective therapy based on their tumor’s unique characteristics while simultaneously reducing unnecessary financial burdens.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chung T. Park Y.N. Up-to-Date Pathologic Classification and Molecular Characteristics of Intrahepatic Cholangiocarcinoma Front. Med.2022985714010.3389/fmed.2022.85714035433771 PMC 9008308 · doi ↗ · pubmed ↗
- 2Kinzler M.N. Schulze F. Bankov K. Gretser S. Becker N. Leichner R. Stehle A. Abedin N. Trojan J. Zeuzem S. Impact of small duct- and large duct type on survival in patients with intrahepatic cholangiocarcinoma: Results from a German tertiary center Pathol. Res. Pract.202223815412610.1016/j.prp.2022.15412636137398 · doi ↗ · pubmed ↗
- 3Zen Y. Intrahepatic cholangiocarcinoma: Typical features, uncommon variants, and controversial related entities Hum. Pathol.202313219720710.1016/j.humpath.2022.06.00135697170 · doi ↗ · pubmed ↗
- 4Carotenuto M. Sacco A. Forgione L. Normanno N. Genomic alterations in cholangiocarcinoma: Clinical significance and relevance to therapy Explor. Target. Antitumor Ther.2022320022310.37349/etat.2022.0007936046845 PMC 9400790 · doi ↗ · pubmed ↗
- 5Lee S.-H. Song S.Y. Recent Advancement in Diagnosis of Biliary Tract Cancer through Pathological and Molecular Classifications Cancers 202416176110.3390/cancers 1609176138730713 PMC 11083053 · doi ↗ · pubmed ↗
- 6Zhu A.X. Macarulla T. Javle M.M. Kelley R.K. Lubner S.J. Adeva J. Cleary J.M. Catenacci D.V.T. Borad M.J. Bridgewater J.A. Final Overall Survival Efficacy Results of Ivosidenib for Patients with Advanced Cholangiocarcinoma with IDH 1 Mutation: The Phase 3 Randomized Clinical Clar ID Hy Trial JAMA Oncol.202171669167710.1001/jamaoncol.2021.383634554208 PMC 8461552 · doi ↗ · pubmed ↗
- 7Vogel A. Sahai V. Hollebecque A. Vaccaro G.M. Melisi D. Al Rajabi R.M. Paulson A.S. Borad M.J. Gallinson D. Murphy A.G. An open-label study of pemigatinib in cholangiocarcinoma: Final results from FIGHT-202ESMO Open 2024910348810.1016/j.esmoop.2024.10348838838500 PMC 11190465 · doi ↗ · pubmed ↗
- 8De Santis A. Zhu L. Tao J. Reißfelder C. Schölch S. Molecular subtypes of intrahepatic cholangiocarcinoma Trends Mol. Med.202510.1016/j.molmed.2025.01.00839955217 · doi ↗ · pubmed ↗