Cerebral Amyloid Angiopathy Related Inflammation: A Single-Center Case Series Analysis
Syed Zahid Ali, Hanah Alley, James Johnson, Harshini Sirvisetty, Michael Sowell, Alex Glynn, Peter Hedera

TL;DR
This paper presents three cases of a rare brain condition called CAA-RI and emphasizes the importance of early diagnosis and treatment for better outcomes.
Contribution
The study contributes a detailed case series and literature review on the rare condition CAA-RI, emphasizing diagnostic and treatment insights.
Findings
CAA-RI can present with a wide range of symptoms, leading to frequent misdiagnosis.
Immunosuppressive therapy shows variable but beneficial outcomes when initiated early.
MRI findings often overlap with other conditions, complicating diagnosis without biopsy.
Abstract
Background: Cerebral amyloid angiopathy-related inflammation (CAA-RI) is a rare subtype of cerebral amyloid angiopathy (CAA), which presents mostly as a subacute and reversible encephalopathy. Primary symptoms include behavioral changes and cognitive decline in the form of rapidly progressive dementia, headache, seizures, and focal neurological deficits. It can also manifest as a varied range of typical and atypical presentations. Misdiagnosis is common because it shares symptoms with other infectious, ischemic and autoimmune pathologies and there is also a significant overlap of MRI findings. Methods: Gold standard diagnosis requires brain biopsy in appropriate clinical setting, but diagnostic criteria is established for probable and possible CAA-RI using clinical symptoms and MRI findings in the absence of other inflammatory, infectious or autoimmune processes. Immunomodulatory…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
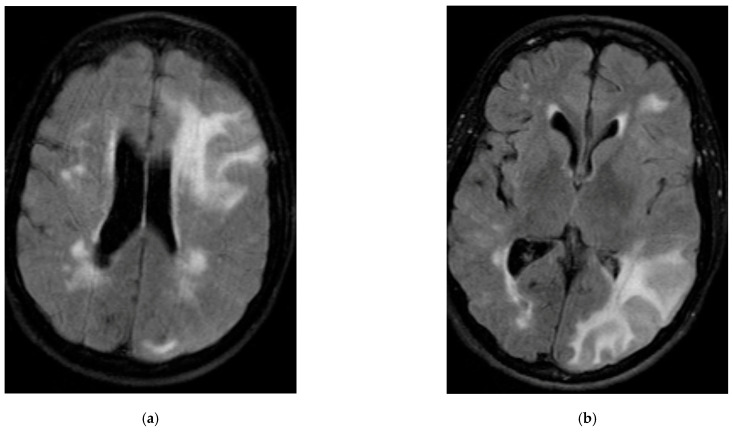 Figure 1
Figure 1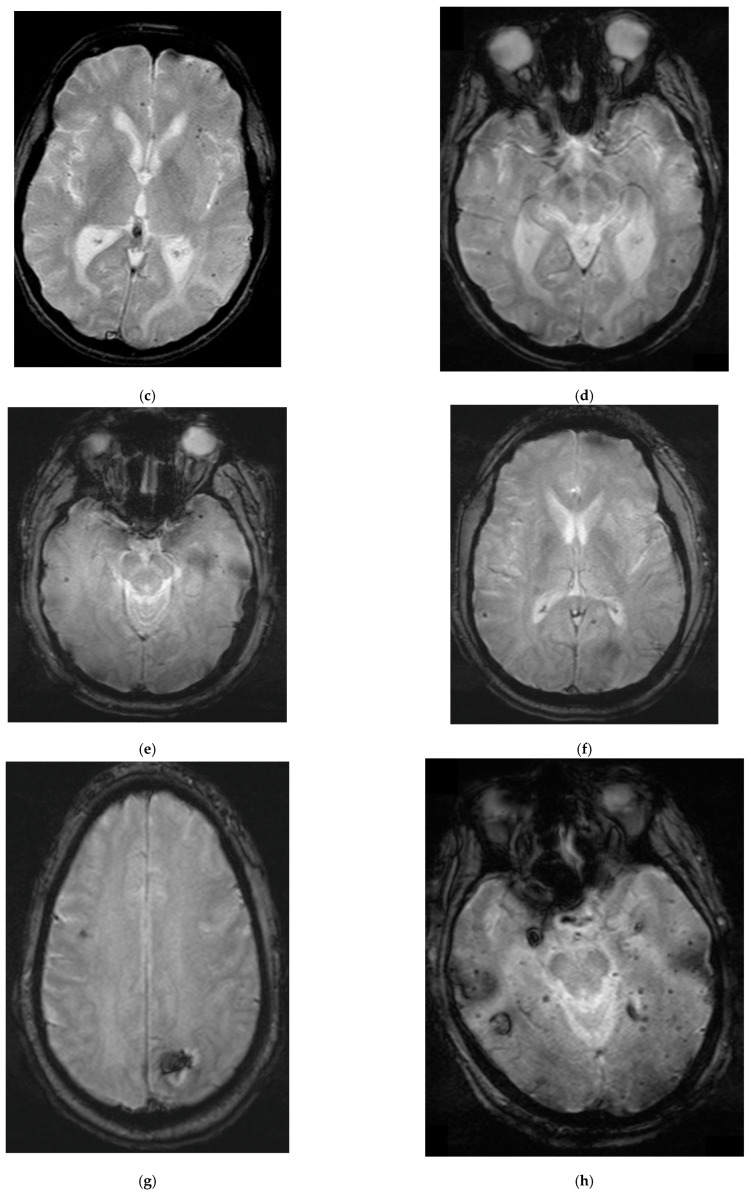 Figure 2
Figure 2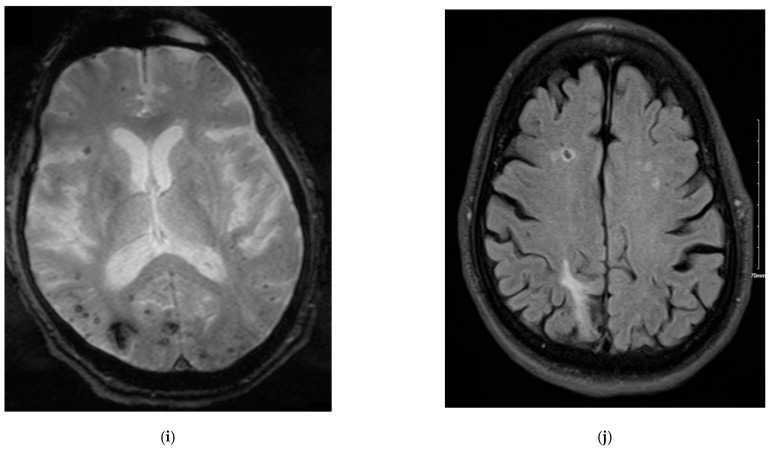 Figure 3
Figure 3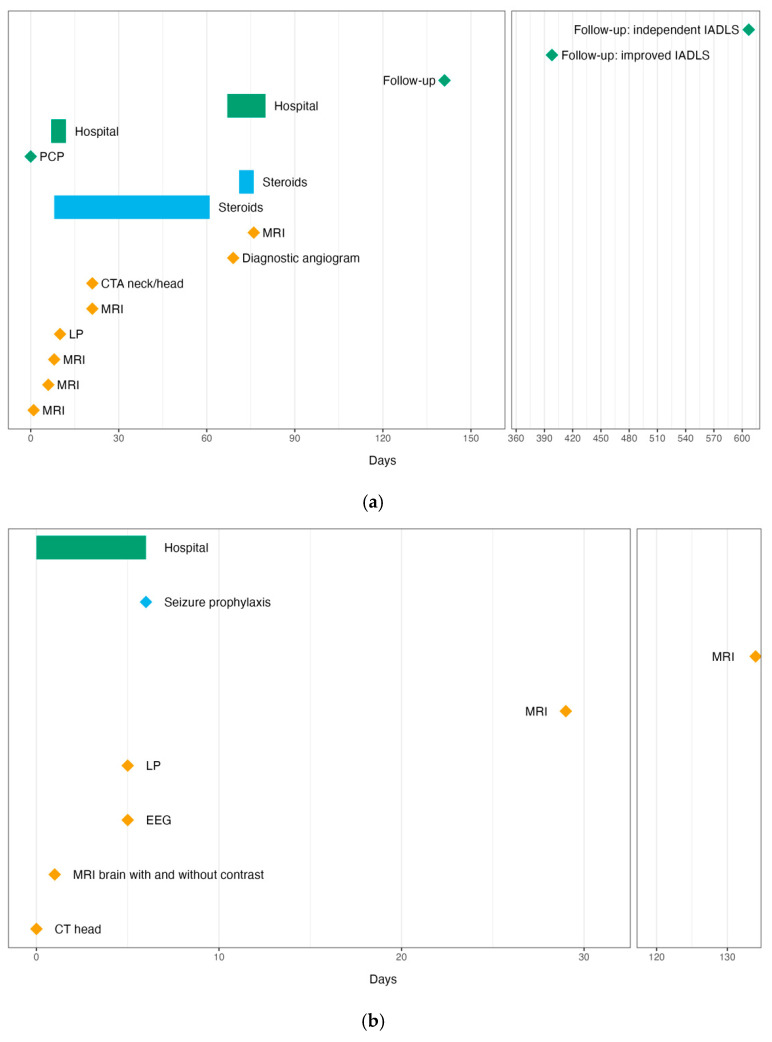 Figure 4
Figure 4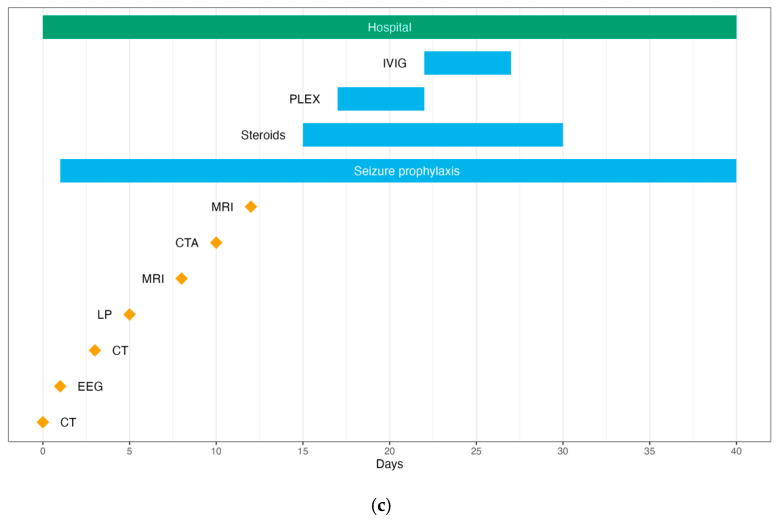 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracerebral and Subarachnoid Hemorrhage Research · Cerebrovascular and genetic disorders · Alzheimer's disease research and treatments
1. Background and Rationale
Cerebral Amyloid Angiopathy-related inflammation (CAA-RI) is a less common, inflammatory variant of Cerebral Amyloid Angiopathy (CAA). CAA-RI is a reversible encephalopathy syndrome most commonly presenting with subacute encephalopathy and complaints of cognitive decline along with headache, seizure, and focal neurologic deficits [1,2]. The definitive diagnosis of CAA-RI requires pathology-confirmed brain biopsy. However, in recent years, criteria only requiring clinical and radiographic evidence has been validated to diagnose either probable or possible CAA-RI without biopsy [3]. Prompt recognition and diagnosis is essential as patients’ symptoms due to CAA-RI tend to respond to immunosuppressive agents, most commonly intravenous high-dose corticosteroid pulse with oral taper of steroids [4,5,6].
CAA-RI is described in the literature as most commonly being monophasic but relapsing courses have been described and are likely more common than previously documented [7,8]. Relapsing symptoms tend to occur when immunosuppression is discontinued or tapered [4,7,9].
We present three cases of probable CAA-RI who were admitted to our hospital with various symptoms. Two of these patients received IV steroids followed by oral taper and had significant improvement in symptoms. One patient had mild symptoms at presentation and did not require any immunomodulatory therapy.
2. Case Summaries
2.1. Patient 1
A 75-year-old female with a history of hypertension, hyperlipidemia, diabetes mellitus type 2, hypothyroidism and fibromyalgia presented as a transfer from an outside hospital with word finding progressive difficulty and cognitive decline. Her MRI showed diffuse edema scattered more prominently in the left cerebral hemisphere, confluent bilateral white matter hyperintensities, and susceptibility-weighted imaging concerning amyloid angiopathy (Figure 1a,b). Lumbar puncture was performed, and showed normal cell count and metabolites without any evidence of infection or autoimmune process. She met diagnostic criteria for probable CAA-RI and was treated with high-dose oral dexamethasone. She initially responded to this therapy with subjective improvement in cognition. During the tapering schedule of dexamethasone, she deteriorated, with worsening of her cognitive dysfunction six weeks after starting initial treatment. On repeat imaging, she was found to have had an acute stroke. The patient started on antithrombotic and statin for secondary prevention. Her mental status failed to improve. She was subsequently treated with another course of high-dose intravenous methylprednisolone, and she had significant improvement in cognitive symptoms on day 4 of treatment. Formal neuropsychiatric evaluation was performed five months post-steroid-pulse therapy and significant improvement in cognitive function was noted. At the follow-up appointment one-year post-steroid pulse (about 17 months after discharge), she continues to endorse cognitive improvement in performing independent activities of daily living.
2.2. Patient 2
Patient is a 46-year-old male without any significant past medical history who presented as a transfer from outside hospital after having a motor vehicle accident secondary to a prolonged seizure while driving. His imaging showed a left occipital hemorrhage and confluent symmetric bilateral white matter hyperintensities (Figure 1c,d). Subsequent MRI confirmed hemorrhage on GRE sequence but also showed multiple areas of lobar cerebral microbleeds. EEG demonstrated polymorphic background seen over both posterior head regions, worse on the left, suggestive of a structural lesion in the left hemisphere. Lumbar puncture was performed, and did not show any obvious abnormality. He was started on seizure prophylaxis. He did not receive any steroids as his seizures were controlled and his clinical status improved rapidly.
2.3. Patient 3
A 72-year-old male with prior medical history significant for cerebral amyloid angiopathy, hypertension, hyperlipidemia and prostate cancer treated with prostatectomy, presented with confusion, and intermittent periods of staring and lip smacking. Patient was initially started on anti-seizure medications because of suspicion for epileptiform events. EEG monitoring was consistent with non-epileptic events and showed diffuse dysfunction without active seizure-like activity. He remained severely altered and encephalopathic and his level of consciousness declined. His MRI showed areas of gliosis, encephalomalacia, confluent white matter hyperintensities and numerous bilateral cerebral microbleeds (Figure 1e,f). Lumbar puncture did not show any sign of infectious or autoimmune processes. He underwent PLEX therapy followed by IVIG therapy because of suspicion for an autoimmune encephalitis. He did not improve, so the diagnosis of probable CAA-RI was also considered. He was treated with five days’ course of high-dose steroids. His condition improved with high-dose IV steroids, followed by oral steroids taper. Goals of care were changed by the family, and referral to an outpatient palliative care program was placed.
Bloodwork and cerebrospinal fluid analysis for all three patients are provided in Table 1. Timelines of each patient’s clinical course are provided in Figure 2.
3. Discussion
Cerebral amyloid angiopathy-related inflammation is a rare disorder characterized by inflammatory reaction to deposits of Aβ (amyloid-β) in cerebral blood vessels, specifically in tunica media and adventitia [10]. It commonly occurs in elderly patients. Typical clinical features include cognitive impairment, stroke-like focal neurological deficits, seizures, altered mental status, and headache. Cognitive impairment is usually mild but, in some cases, it can be rapidly progressive with severe mental decline occurring in a matter of days to weeks [1].
Diagnosis of CAA-RI is challenging as there are no definite differences in neuroimaging findings seen in CAA and CAA-RI. Frequent neuroimaging findings in CAA include multiple lobar cerebral microbleeds (CMBs), cortical superficial siderosis (CSS) or subarachnoid hemorrhage (SAH), white matter hyperintensities (WMHs), enlarged perivascular spaces (EPVs) commonly in the centrum semiovale (CSO), and cortical atrophy. All these neuroimaging abnormalities can be also seen in CAA-RI. Evidence of inflammation solely based on neuroimaging is very difficult to establish [11,12].
Thus, original diagnostic criteria mandate neuropathological evidence of inflammation [13]. Considering the risk-to-benefit ratio, performing biopsy in an elderly population, in which brain parenchyma is prone to hemorrhages, is a difficult decision for patients and physicians. Due to increased recognition of CAA-RI cases, and extensive review of neuroimaging findings, it is now feasible to manage these cases with increased diagnostic certainty, while avoiding the risks of brain biopsy [3]. When biopsy is not a safe consideration, in the right clinical setting, MRI is extremely helpful in diagnosing CAA-RI cases and monitoring treatment response.
As mentioned earlier, most frequent neuroimaging findings in cases of CAA-RI include widespread CMBs, WMH, EPVs, and CSS. CSF analysis may help in the right clinical settings to rule out other infectious, autoimmune, or paraneoplastic condition, which can present in a similar fashion [14,15].
None of our patients underwent biopsy for neuropathological examination, but all of them met the diagnostic criteria for probable CAA-RI (Table 2). Patients 1 and 3 received IV steroids followed by oral taper with significant improvement of symptoms. Patient 2 was relatively young and had no known medical history. There was no family history of dementia, and his symptoms improved even without use of anti-inflammatory agents.
Other options for immunosuppression are also available, but the majority of cases respond very well to readily available intravenous and oral corticosteroids. Therefore, these options are reserved only for those cases which do not show improvement. These options include methotrexate, mycophenolate–mofetil, cyclophosphamide, immunoglobulins and azathioprine [16,17,18].
Our reported cases demonstrate the importance of early diagnosis of CAA-RI based on a high index of suspicion, and further support administration of high-dose steroids as an effective treatment for this condition.
The limitations of this case series include the small number of patients and length of follow-up. While one patient was followed up to 17 months post-discharge, the other two patients have been out of the hospital less than 6 months at time of writing. A longer observation period will be necessary to characterize recovery patterns and treatment efficacy. While a definitive diagnosis of CAA-RI would require histopathology, given its invasive nature, it is generally avoided and not preferred by patients or families; this occurred with all patients in our case series analysis.
4. Conclusions
Our personal experience of diagnosis and treatment of a case of CAA-RI and extensive review of the available literature indicate that lobar CMBS and white matter hyperintensities are the most frequent neuroimaging findings in CAA-RI. The most frequent symptom is cognitive impairment and behavioral changes, but new onset seizure can be the first symptom to present. Diagnosis is challenging. If untreated, disease can be aggressive and fatal. Immunosuppression is the mainstay of treatment, and treatment response varies in different patients. Early diagnosis and prompt initiation of immunosuppressive therapy is beneficial in most cases. Treatment becomes more challenging in cases of other concomitant pathologies, like stroke, epilepsy, systemic and central nervous system infections. We recommend close follow-up of these patients after treatment to see long-term complications and monitor cognitive decline. Future research projects should include extensive search for preventable risk factors for this condition if any exist. There is also a dire need to look for early serum biomarkers in CAA-RI which can raise clinical suspicion, and aid in diagnosis and monitoring disease course and treatment response.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Castro Caldas A. Silva C. Albuquerque L. Pimentel J. Silva V. Ferro J.M. Cerebral Amyloid Angiopathy Associated with Inflammation: Report of 3 Cases and Systematic Review J. Stroke Cerebrovasc. Dis.2015242039204810.1016/j.jstrokecerebrovasdis.2015.04.01526163888 · doi ↗ · pubmed ↗
- 2Li D. Qin W. Guo Y. Xia M. Li S. Zhang J. Zang W. Clinical, laboratory, and radiological features of cerebral amyloid angiopathy-related inflammation (CAA-ri): Retrospective, observational experience of a single centre Neurol. Sci.20234463163810.1007/s 10072-022-06436-736207650 · doi ↗ · pubmed ↗
- 3Auriel E. Charidimou A. Gurol M.E. Ni J. Van Etten E.S. Martinez-Ramirez S. Boulouis G. Piazza F. Di Francesco J.C. Frosch M.P. Validation of Clinicoradiological Criteria for the Diagnosis of Cerebral Amyloid Angiopathy-Related Inflammation JAMA Neurol.20167319720210.1001/jamaneurol.2015.407826720093 · doi ↗ · pubmed ↗
- 4Kozberg M.G. Perosa V. Gurol M.E. van Veluw S.J. A practical approach to the management of cerebral amyloid angiopathy Int. J. Stroke 20211635636910.1177/174749302097446433252026 PMC 9097498 · doi ↗ · pubmed ↗
- 5Regenhardt R.W. Thon J.M. Das A.S. Thon O.R. Charidimou A. Viswanathan A. Gurol M.E. Chwalisz B.K. Frosch M.P. Cho T.A. Association Between Immunosuppressive Treatment and Outcomes of Cerebral Amyloid Angiopathy-Related Inflammation JAMA Neurol.2020771261126910.1001/jamaneurol.2020.178232568365 PMC 7309570 · doi ↗ · pubmed ↗
- 6Szalardy L. Fakan B. Maszlag-Torok R. Ferencz E. Reisz Z. Radics B.L. Csizmadia S. Szpisjak L. Annus A. Zadori D. Identifying diagnostic and prognostic factors in cerebral amyloid angiopathy-related inflammation: A systematic analysis of published and seven new cases Neuropathol. Appl. Neurobiol.202450 e 1294610.1111/nan.1294638093468 · doi ↗ · pubmed ↗
- 7Kinnecom C. Lev M.H. Wendell L. Smith E.E. Rosand J. Frosch M.P. Greenberg S.M. Course of cerebral amyloid angiopathy-related inflammation Neurology 2007681411141610.1212/01.wnl.0000260066.98681.2e 17452586 · doi ↗ · pubmed ↗
- 8Martucci M. Sarria S. Toledo M. Coscojuela P. Vert C. Siurana S. Auger C. Rovira A. Cerebral amyloid angiopathy-related inflammation: Imaging findings and clinical outcome Neuroradiology 20145628328910.1007/s 00234-014-1330-624493378 · doi ↗ · pubmed ↗