Presumed Bartonella-Associated Spondylodiscitis in a 3-Year-Old Child: A Case Report and Review of the Literature
Hadi El Assaad, Eckehard Schumann, Christian Klemann, Nadine Dietze-Jergus, Christoph-Eckhard Heyde, Philipp Pieroh

TL;DR
A 3-year-old child with back pain and fever was diagnosed with Bartonella-associated spondylodiscitis after initial treatments failed, highlighting the need to consider this rare cause in children.
Contribution
This case report adds to the limited literature on pediatric Bartonella henselae spondylodiscitis and emphasizes its diagnostic challenges.
Findings
The child showed rapid improvement after switching to azithromycin and rifampicin following a positive Bartonella henselae IgM test.
A literature review identified 28 pediatric cases with significant variation in diagnosis and treatment approaches.
The case highlights the importance of considering Bartonella in the differential diagnosis of pediatric vertebral osteomyelitis.
Abstract
With an incidence of 0.3 per 100,000, spondylodiscitis is a rare condition in children. It is typically bacterial in origin and most commonly caused by Staphylococcus aureus. Bone involvement in cat-scratch disease (CSD) due to Bartonella henselae is exceedingly rare, occurring in only 0.17–0.27% of cases. We present the case of a 3-year-old boy with a two-week history of intermittent back pain and a recent onset fever. Initial laboratory findings were unremarkable, and MRI revealed spondylodiscitis at L3/4 without abscess formation. Empirical antibiotic treatment with ampicillin/sulbactam showed no clinical response. Serologic testing revealed a positive Bartonella henselae IgM (IgG negative), leading to a change in antibiotic treatment to azithromycin and rifampicin for three weeks, resulting in rapid clinical improvement. Follow-up at nine weeks showed marked clinical and radiologic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
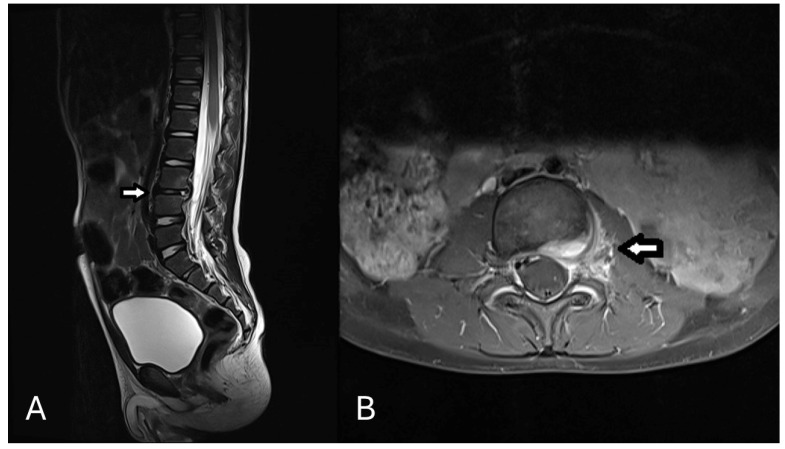 Figure 1
Figure 1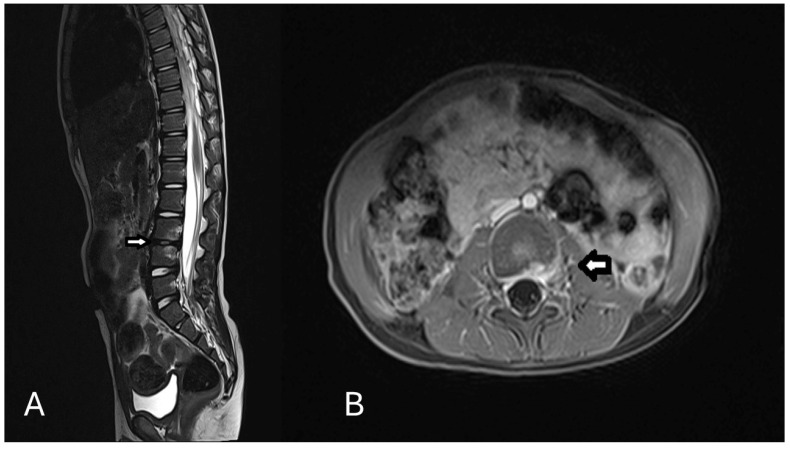 Figure 2
Figure 2- —Open Access Publishing Fund of Leipzig University
- —German Research Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBartonella species infections research · Infectious Diseases and Tuberculosis · Rabies epidemiology and control
1. Introduction
Spondylodiscitis is the infection of the intervertebral disc and the adjacent vertebrae [1,2]. Compared to adults, it is rare in children with an incidence of 0.3 versus 2.4 per 100,000 patients, respectively. Moreover, it accounts for only 3% of osteoarticular infections in pediatric hospitals [1,3].
In children, spondylodiscitis is primarily bacterial, with Staphylococcus aureus as the most common pathogen. Kingella kingae has also been recognized as a significant pathogen in pediatric patients, along with Streptococci [4]. Rare causes of pediatric spondylodiscitis include fungal pathogens such as *Candida *spp. and *Aspergillus *spp., parasitic infections like *Echinococcus *spp. [4] as well as cat-scratch disease, caused by Bartonella henselae.
Members of the genus Bartonella are fastidious, pleomorphic, Gram-negative rods belonging to the α2 subgroup of Proteobacteria, closely related to genera such as Brucella, Agrobacterium, and Rhizobium [5]. The species responsible for most human infections are Bartonella henselae, B. quintana, and B. bacilliformis [6].
Cat-scratch disease (CSD) is primarily characterized by subacute, localized, self-limiting lymphadenitis, typically preceded by a local cutaneous reaction at the scratch site. In 90% of cases, symptoms resolve within 2–4 weeks without antibiotic treatment [7]. However, about 10% of cases present with atypical manifestations such as prolonged fever, erythema nodosum, and granulomas in the liver or spleen. Bone involvement in CSD is extremely rare, reported in only 0.17–0.27% of cases [7,8]. Additionally, vertebral involvement accounts for 42% of bone-related CSD cases [9].
We present a pediatric case of spondylodiscitis caused by CSD, an exceptionally rare condition, along with a review of the literature. This case contributes valuable insight to the limited body of knowledge on CSD-induced vertebral involvement [4,10].
2. Case Presentation
A 3-year-old male patient without a previous medical history was admitted to the hospital with a two-week history of intermittent back pain. Before pain onset he sustained a spinal contusion at kindergarten, and a fracture was ruled out. He reported a mild decrease in pain. Since then, the patient was occasionally observed limping while walking. In addition, the parents reported episodes of fever (up to 39 °C) that started three days before admission. His pediatrician could not determine the site of infection. The patient resides in the eastern region of Germany, and the parents denied recent travel. According to the parents, the patient had contact with cats 6–10 weeks prior to presentation but has not sustained any open wounds or scratches. On clinical examination, he had normal posture with no spinal deformities or other abnormal findings. Routine blood investigations revealed normal levels of C-reactive protein (CRP) at 1.78 mg/L (reference value < 5 mg/L) and non-pathological leucocytes count of 8 × 10^9^/L (reference: 5–12 × 10^9^/L). A hip ultrasound examination bilaterally revealed no fluid collection or other joint abnormalities. A lumbar spine and pelvis magnetic resonance imaging (MRI) showed a focal spondylodiscitis L 3/4 without evidence of abscess formations (Figure 1). An abdominal sonography was performed without evidence for infectious focus or organomegaly.
Other infectious foci were excluded. An intravenous broad spectrum antibiotic therapy with ampicillin and sulbactam as well as analgesic therapy was initiated. The initial blood cultures were negative. Extensive infectious diagnostic workup including serology for Borrelia and Bartonella and an Interferon Gamma Release Assay (IGRA)-Test for tuberculosis were performed. On day 8 of hospitalization, Bartonella henselae serology was positive for IgM (IgG negative) through immunofluorescence assay, while all other infectious tests were negative, prompting a change in antibiotic treatment to the combination of azithromycin (75 mg daily) and rifampicin (150 mg daily). Oropharyngeal sample collection was initially planned to test for Kingella kingae. However, after receiving positive serology results for Bartonella henselae established the microbiological diagnosis, the Kingella kingae PCR was not performed. Furthermore, a corset to immobilize the spine was fitted and worn by the patient during the hospitalization. After starting antibiotic therapy and the spine immobilization, the patient showed a rapid clinical improvement, and the pain quickly subsided.
On day 12 of hospitalization, the patient was discharged on oral antibiotics (azithromycin and rifampicin). Antibiotic treatment was administered intravenously for one week, followed by two weeks orally. Spinal immobilization using the corset was recommended for a further six weeks, and a control MRI was planned after 8–12 weeks. Serology was repeated two weeks after initial diagnosis and showed IgM positivity further without evidence for IgG. In accordance with current recommendations, we performed an additional PCR on blood, which was negative.
After nine weeks, the follow-up MRI showed marked regression of inflammatory changes and a substantial reduction in disease activity (Figure 2). Serology testing was repeated without evidence of IgG and IgM positivity. Although this serological course does not fulfil classical criteria for confirmed infection, it has been previously described in Bartonella infections and does not exclude the diagnosis. Due to the mild clinical course, a biopsy or PCR from tissue was not performed. The laboratory, radiological and clinical examination all indicated a rapid improvement.
3. Literature Review
We conducted a literature review in PubMed for other case reports or case series of pediatric cases with Bartonella henselae vertebral osteomyelitis (Table 1). We found a total of 18 publications (2 case series, 16 case reports). We excluded non-pediatric and non-vertebral osteomyelitis cases. In those papers overall 28 patients were reported.
The median age was 7 years (range: 2–15), and regarding the location of osteomyelitis, 7 cases had cervical, 15 had thoracic, 10 had lumbar, and 6 had sacral involvement. Nearly all cases used Bartonella henselae serology (27 cases) and MRI (25 cases) for the diagnosis. Biopsies and aspirates were used in 12 cases followed by PCR of the specimen. Biopsies did not reveal additional information. Regarding the antibiotic treatment, it varied between the cases. Rifampicin was the most commonly used (17 cases), followed by azithromycin (10 cases), doxycycline (8 cases), trimethoprim/sulfamethoxazole (TMP/SMZ; 6 cases), ciprofloxacin (5 cases), and gentamycin (4 cases). Surgery was needed in two cases where antibiotic treatment did not lead to improvement. (atlantoaxial fusion [13], surgical drainage of the abscess and a laminectomy at C3–C5 [21]).
4. Discussion
We present a case of a 3-year-old boy who presented with back pain and fever diagnosed with Bartonella henselae-induced spondylodiscitis. The diagnosis was established after a series of tests, including MRI, blood cultures and serology. The diagnosis was supported by serology and MRI. The patient was treated with an antibiotic regimen and responded well.
Bone involvement is a rare manifestation of Bartonella henselae, with spondylodiscitis being even more uncommon [7,9].
The patient’s initial symptoms of fever and back pain are non-specific. Though MRI remains the gold standard for the radiological visualization of spondylodiscitis (92% sensitivity and 96% specificity), it does not identify the underlying cause [28].
Blood cultures are performed first to detect the most common infectious causes of spondylodiscitis, including Staphylococcus aureus [28]. Tuberculosis can be ruled out using the tuberculin skin test or the Interferon Gamma Release Assay (IGRA) [29]. In our case, the IGRA was used. When the results of these initial tests were negative, a more extensive infectious disease.
There are many diagnostic tools to detect Bartonella henselae. Blood cultures are usually negative. PCR is highly specific and sensitive for detecting Bartonella henselae DNA in pus or lymph node specimens. In the case of spondylodiscitis, obtaining such samples is not always feasible [30,31].
Immunofluorescence assays (IFA), enzyme-linked immunosorbent assays (ELISA), and chemiluminescence immunoassays (CLIA) can all be used to detect Bartonella from serological samples [32,33,34]. In our case, chemiluminescence immunoassay was performed using VirClia^®^ (which has a specificity of 98.2% for predicting IgM results [34]), and detected the infectious agent, as IgM was positive for Bartonella henselae on presentation and again after 2 weeks. In the serology follow-up after 9 weeks IgM was negative probably due to the regression of the infection, while IgG remained negative possibly because of a delayed or absent seroconversion [32,35].
In our case, the exact mechanism by which Bartonella henselae led to spondylodiscitis was not clear. Previous case reports on Bartonella henselae with bone involvement suggested that it may occur as a direct extension from an infected lymph node [36] or via hematogenous spread from the initial inoculation site (mainly skin) or infected lymph node [37]. But in our patient, no affected lymph node or skin injury was detected.
The patient was treated with a prolonged course of azithromycin, the standard therapy for Bartonella henselae infections [38]. Rifampicin was added to the regimen based on its frequent use in reported cases of Bartonella henselae vertebral osteomyelitis and its demonstrated efficacy. A retrospective study of 268 patients with mild to severe cat-scratch disease found rifampicin to be among the most effective agents, alongside ciprofloxacin, gentamicin, and TMP/SMZ [39]. Considering these findings and given the potential synergistic effect of rifampicin and azithromycin in treating osteomyelitis [40], we opted for this combination.
Moreover, no surgical intervention was needed in this case, and the patient responded well to non-operative management. As outlined in our literature review, the majority of cases responded well to non-operative antibiotic treatment. We acknowledge that antibiotic therapy was initiated empirically before the completion of all microbiological investigations, which is generally not recommended according to adult guidelines [41]. However, no pediatric-specific spondylodiscitis guidelines currently exist. Although the Pediatric Infectious Diseases Society (PIDS) and the Infectious Diseases Society of America (IDSA) recommend invasive diagnostics to establish a microbiological diagnosis, they also emphasize that the decision must consider factors such as procedural and sedation risks [42]. In this case, the patient was clinically stable, had not received prior antibiotics, and non-invasive diagnostic tests were still pending. Given these considerations, we decided to initiate empirical antibiotic therapy. Although cephalosporins are recommended as first-line therapy in regions with low MRSA prevalence, we selected ampicillin/sulbactam based on our institutional antibiotic guidelines, which consider rising resistance rates, particularly among E. coli, and regional susceptibility patterns [43].
Bartonella henselae systemic involvement is a very rare presentation. The few pediatric cases that do exist describe diagnostic delays due to the unusual presentation, though successful outcomes were reported with appropriate antibiotics [44]. Bone involvement is not the only systemic involvement of CSD. In fact, it has also been described that CSD can affect the eyes [45], heart [46], nervous system [47] and hepatosplenic system [48,49]. Therefore, if there is no pathogen detected, Bartonella henselae should be considered.
The patient had a favourable prognosis following treatment, with resolution of symptoms. The overall prognosis for pediatric spondylodiscitis is, in general, good, particularly when treated early [9]. However, Bartonella-induced spondylodiscitis requires careful follow-up to monitor for potential complications as mentioned above, which were fortunately not observed in this patient [28].
In conclusion, this case highlights a presumed Bartonella henselae -associated spondylodiscitis in a young child and underscores the importance of considering Bartonella species in the differential diagnosis of atypical osteoarticular infections in children—even in the absence of lymphadenopathy or serologic confirmation—particularly when classical pathogens do not respond to standard therapy. A rapid clinical response to targeted antibiotic therapy can support the presumptive diagnosis in the absence of confirmatory biopsy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cavalieri S. Pessina B. Indolfi G. Galli L. Trapani S. Spondylodiscitis in Pediatric Age: A Retrospective Cohort Study Pediatr. Infect. Dis. J.20224153053610.1097/INF.000000000000353435675524 PMC 10826916 · doi ↗ · pubmed ↗
- 2Principi N. Esposito S. Infectious Discitis and Spondylodiscitis in Children Int. J. Mol. Sci.20161753910.3390/ijms 1704053927070599 PMC 4848995 · doi ↗ · pubmed ↗
- 3Grammatico L. Baron S. Rusch E. Lepage B. Surer N. Desenclos J.C. Besnier J.M. Epidemiology of vertebral osteomyelitis (VO) in France: Analysis of hospital-discharge data 2002–2003 Epidemiol. Infect.200813665366010.1017/S 095026880700885017568478 PMC 2870846 · doi ↗ · pubmed ↗
- 4Gouliouris T. Aliyu S.H. Brown N.M. Spondylodiscitis: Update on diagnosis and management J. Antimicrob. Chemother.201065(Suppl. S 3)iii 11iii 2410.1093/jac/dkq 30320876624 · doi ↗ · pubmed ↗
- 5Jacomo V. Kelly P.J. Raoult D. Natural History of Bartonella Infections (an Exception to Koch’s Postulate)Clin. Diagn. Lab. Immunol.2002981810.1128/cdli.9.1.8-18.200211777823 PMC 119901 · doi ↗ · pubmed ↗
- 6Angelakis E. Raoult D. Pathogenicity and treatment of Bartonella infections Int. J. Antimicrob. Agents 201444162510.1016/j.ijantimicag.2014.04.00624933445 · doi ↗ · pubmed ↗
- 7Carithers H.A. Cat-scratch disease. An overview based on a study of 1200 patients Am. J. Dis. Child.19851391124113310.1001/archpedi.1985.021401300620314061408 · doi ↗ · pubmed ↗
- 8Margileth A.M. Cat scratch disease Adv. Pediatr. Infect. Dis.199381218216999 · pubmed ↗