One-Year Follow-Up of Non-Healing Socket in Hodgkin’s Lymphoma Patient: Case Report and Literature Review on Management Strategies
Ahmed Ata Alfurhud

TL;DR
A Hodgkin’s lymphoma patient experienced a non-healing socket after dental treatment involving sodium hypochlorite, highlighting risks in immunocompromised individuals.
Contribution
This case report adds to the understanding of NaOCl-related complications in immunocompromised patients and suggests potential management strategies.
Findings
NaOCl exposure led to bone necrosis in a Hodgkin’s lymphoma patient with a history of chemotherapy.
The patient’s healing was prolonged due to immunocompromised status, requiring long-term follow-up and antimicrobial therapy.
Adjunctive treatments like L-PRF, PENTO, and HBOT were proposed for managing non-healing sockets in similar cases.
Abstract
Background and Clinical Significance: Sodium hypochlorite (NaOCl) is widely used in root canal treatment for its potent antiseptic and antibacterial effects. However, its cytotoxicity—particularly at higher concentrations and in patients with low immune status—has been associated with serious postoperative complications. This case report describes the risks associated with NaOCl exposure in a medically compromised patient and reviews the relevant literature on NaOCl-related injuries, offering insights into potential current management strategies. Case Presentation: This case report describes a challenging scenario of a 25-year-old male with a history of Hodgkin’s lymphoma who developed a non-healing bone in the lower right first molar (LR6) region after NaOCl exposure. Several months after undergoing root canal treatment and an extraction of the LR6, the patient presented with exposed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3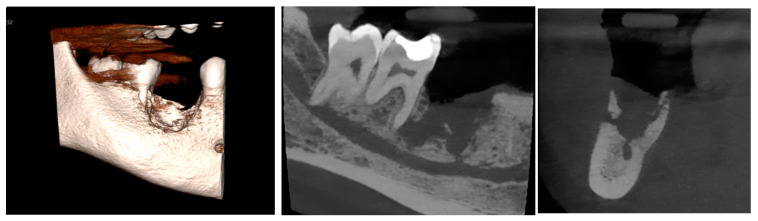 Figure 4
Figure 4 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral and Maxillofacial Pathology · Endodontics and Root Canal Treatments · Oral health in cancer treatment
1. Introduction
Sodium hypochlorite (NaOCl) has been extensively utilized in dentistry for many years. Its use is critical for achieving successful root canal treatment, functioning as an effective antiseptic and antibacterial irrigating solution to significantly eliminate bacterial populations within the canal system [1]. The clinical technique centers on thorough cleaning and debridement, ensuring the removal of bacteria, necrotic tissue, and residual organic material, which is essential for optimizing treatment outcomes [1]. Nevertheless, concerns have been raised regarding the cytotoxicity of NaOCl, particularly at higher concentrations, with occasional reports of postoperative complications. Several studies have reported both temporary and permanent complications associated with the potential toxicity of NaOCl [1]. Serious complications have been documented in the literature, including unilateral facial swelling, persistent paresthesia in the affected region, and partial paralysis of the facial muscles [2]. Moreover, weakness of the buccal branch of the facial nerve has also been observed, leading to the loss of the nasolabial angle and a downward deviation of the right corner of the mouth [3].
The medical history of a patient is a critical factor in assessing the risk of complications. Medically compromised individuals are particularly at risk of experiencing severe adverse effects from NaOCl compared with healthy patients, as pre-existing systemic conditions may enhance its cytotoxicity, impair tissue repair mechanisms, and increase the likelihood of nerve damage and soft-tissue necrosis. Lymphoma is a diverse malignant condition of the lymphatic system, marked by the abnormal growth of lymphoid cells. Hodgkin’s lymphoma predominantly affects the lymph nodes, with more than 90% of cases occurring in these areas, while only 1–4% involve extranodal sites, usually presenting as a nodal disease with a preference for the neck and mediastinal nodes [4].
Diagnosing oral lymphomas can be difficult, as their symptoms often mimic those of other conditions like periodontal disease, osteomyelitis, and other cancers, which may result in delayed treatment and a poorer prognosis [4]. The current case presents significant diagnostic challenges due to the complexity of the patient’s medical history. Pre-existing conditions and underlying health factors complicate the identification of symptoms, making it difficult to distinguish between the primary disease, other potential comorbidities, and local complications, thereby complicating the diagnostic process.
2. Case Presentation
A 25-year-old male was referred to the Oral and Maxillofacial Surgery Department (OMFS) at the Royal London Dental Hospital (RLDH) with exposed necrotic bone in the lower right first molar (LR6) region. The patient had previously undergone root canal treatment on the LR6 in Romania several months ago. He later presented to a general dental practice in the United Kingdom with exposed bone in the LR6 area, reporting no pain but experiencing an unpleasant taste. Concerned about the exposed necrotic bone in the LR6 socket and the patient’s complex medical history, the general dentist referred him to the OMFS Department for further evaluation and management. The patient’s medical history included a diagnosis of Hodgkin’s lymphoma (stage 2), for which he underwent a six-month course of chemotherapy, completed in September 2020. Additionally, he experienced an endodontic irrigation material-related incident in the LR6 region, which may have contributed to the development of complications in the area.
2.1. Clinical Examination
Intraorally, a preoperative photograph (Figure 1), provided by the general dentist who initially examined the patient, revealed a temporary restoration on the LR6. Additionally, there was an area of exposed, non-healing bone on the buccal aspect, extending from the mesial surface of the LR6 to the distal surface of the lower right second molar. A relative blood clot was observed on the mesial surface of the LR6, with no identifiable cause.
A few weeks later, the patient was evaluated by a specialist at the OMFS Department at the RLDS. A clinical examination revealed non-healing exposed necrotic bone in the LR6 region, as illustrated in Figure 2. Additionally, signs of infection were evident, including pain, purulent discharge at the LR6 site, and mild extraoral swelling on the lower right side of the face.
2.2. Differential Diagnosis
The clinical findings were suggestive of a differential diagnosis, as follows: the most likely diagnosis in this case was bone necrosis due to a sodium hypochlorite incident, as the patient had a history of an endodontic irrigation-related incident in the LR6 region. Sodium hypochlorite is known for its cytotoxic effects, and accidental extrusion beyond the root canal system can lead to severe tissue damage, necrosis, and delayed healing, which aligns with the patient’s clinical presentation of exposed necrotic bone.
However, other differential diagnoses could not be excluded at this stage. Chronic osteomyelitis remains a possibility, as persistent infection in the LR6 area may lead to necrotic bone, purulent discharge, and localized swelling. Additionally, primary or secondary malignancy, such as lymphoma or metastatic carcinoma, should be considered. Lastly, traumatic bone sequestration could also be a contributing factor, particularly if prior dental procedures caused localized trauma, leading to devitalized bone fragments and subsequent exposure.
2.3. Management and Intervention
The patient was advised on improving oral hygiene practices to help prevent the progression of bone necrosis, which included proper brushing techniques, antimicrobial mouth rinses, and regular dental check-ups to maintain oral health and minimize the risk of further complications. Given the clinical evidence of infection, a 14-day course of oral 500 mg of amoxicillin, three times a day, was prescribed to control the infection and reduce the bacterial load in the affected area. As the LR6 was deemed non-restorable due to its fragility after the root canal treatment and the presence of a large, mobile, fractured fragment, a simple extraction was performed under local anesthesia to eliminate the source of infection and promote healing, with careful attention to minimizing trauma. A biopsy of the necrotic bone and surrounding mucosa was undertaken to exclude malignancy. Additionally, an ostectomy of the buccal plate of bone (buccal cortex) was performed, followed by curettage of the necrotic bone. The patient was placed on a long-term follow-up protocol to monitor their healing, assess for any recurrence of necrotic bone, and ensure no signs of persistent infection or malignancy, with regular clinical and radiographic evaluations scheduled to track progress and intervene if necessary.
2.4. Microscopic Description
Gross examination of the biopsy specimen revealed both hard and soft tissues, with irregular, discolored, and friable bone and mucosa. Histopathological analysis showed acellular necrotic bone, characterized by empty lacunae and loss of osteocytes, surrounded by bacterial aggregates and a mixed inflammatory infiltrate. The bacteria were interspersed with neutrophilic infiltrates and fragments of granulation tissue, with collections of multinucleated osteoclast-type giant cells also observed. The adjacent mucosal biopsy consisted of tissue fragments covered by hyper-parakeratinized epithelium, exhibiting variable hyperplasia, fibrin deposits, and chronic inflammatory cell infiltration. The epithelium demonstrated neutrophilic trafficking and spongiosis, with no significant cytological atypia. Dense infiltrates of neutrophils, lymphoplasmacytic cells, and histiocytes were present, along with scattered hemosiderin deposits. No evidence of epithelial dysplasia or malignancy was identified. The findings are consistent with chemically induced necrosis due to sodium hypochlorite exposure.
2.5. Follow-Up and Outcomes
The initial radiographic assessment was conducted a few weeks after the surgery. As shown in Figure 3, the orthopantomograph (OPG) revealed a non-healing bony defect within the extraction socket. This defect extended inferiorly, encroaching upon the inferior alveolar canal, which may suggest the potential involvement of the nerve. Notably, there was an increase in the bony density adjacent to the socket, consistent with sclerosing osteitis. These findings necessitate further radiographic evaluation and monitoring to assess the progression of healing and any potential complications.
A cone-beam computed tomography (CBCT) scan of the posterior mandible revealed a bony sequestrum in the region of the missing LR6 socket, as shown in Figure 4. There was a subtle periosteal bone reaction on both the buccal and lingual aspects of the socket, along with a marked increase in the adjacent bony density. The bony defect extended inferiorly to involve the inferior alveolar canal, with a small dehiscence of its superior cortex. Additionally, the defect extended mesially to the root of the LR7, with apical periodontal ligament space widening at both LR7 apices. The inferior alveolar canal was in contact with the buccal aspect of the radiolucency associated with the distal apex of the LR7, and there was partial loss of the canal’s cortical outline in this region.
Although the definitive diagnosis, confirmed by the histopathological examination, was necrosis due to sodium hypochlorite exposure, the patient required ongoing regular follow-up to monitor the healing process. Given the patient’s complex medical history, including prior chemotherapy, there was an increased risk of delayed healing, secondary infection, and potential complications, such as osteomyelitis. Regular clinical and radiographic assessments are essential to evaluate bone regeneration, soft-tissue healing, and any signs of persistent inflammation or further necrosis.
The primary objective in this case was to achieve primary closure to minimize the risk of infection at the surgical site. However, this was not possible due to the compromised healing process, likely resulting from the patient’s history of chemotherapy. Chemotherapy can impair wound healing by affecting cellular regeneration, reducing vascular supply, and compromising immune response, increasing the risk of delayed epithelialization and secondary infection. As a result, the open wound remained vulnerable to bacterial colonization and further necrosis.
As can be seen in Figure 5, the healing process in this case was prolonged and complex. During follow-up, the surgical site showed minimal progress, with no complete healing observed. Despite nearly a year of monitoring, primary closure was not achieved, likely due to impaired tissue regeneration and delayed healing associated with the patient’s medical history. This necessitated continued follow-up and potential adjunctive interventions to support tissue repair and minimize the risk of further complications.
The clinical findings, as shown in Figure 5, were recorded during the patient’s last attended appointment, one year after the surgery. Unfortunately, the patient did not return for the remaining follow-up appointments for unknown reasons, making it challenging to assess the long-term healing progress and any potential complications.
2.6. Review of the Literature
Several case reports identified in the literature review, summarized in Table 1, describe a wide range of complications associated with NaOCl exposure. Most of these complications are typically uncomplicated and resolve within a few days to weeks; however, some complications may persist for a prolonged period or even become permanent. Accidental exposure to NaOCl during endodontic procedures typically results in mild to moderate complications, including pain and swelling, which generally resolve within a period ranging from several days to weeks. However, some severe symptoms, such as skin discoloration, chemical burns, and mucosal or bone necrosis, may require a prolonged healing period, with full recovery potentially taking up to months. Accidental NaOCl exposure can result in severe, long-lasting, or permanent complications, such as sensory impairment, paresthesia, facial nerve dysfunction and facial muscle weakness potentially persisting for years or even becoming permanent. Therefore, most NaOCl-related injuries are self-limiting, with the majority healing completely within a few weeks. However, in severe cases involving extensive nerve tissue damage, the healing period may extend for a long time. A summary of the included case reports is provided in Table 1.
3. Discussion
Identifying the risk factors that predispose individuals to prolonged bone necrosis following NaOCl exposure is essential for both prevention and effective management. The presented case led to bone necrosis and a non-healing extraction socket, with the complication persisting for a much longer period than expected. This extended healing time exceeded the typical duration described in the literature, indicating that there may be additional factors influencing wound healing and tissue repair, which likely contributed to the prolonged nature of the complication. Individuals with impaired immune function or those undergoing immunosuppressive treatment are at a significantly higher risk of developing severe complications following NaOCl injuries [17]. In immunocompromised patients, such as those with Hodgkin’s lymphoma, a usually localized area of tissue necrosis may progress more rapidly or show delayed healing.
The clinical outcome of a NaOCl accident is largely influenced by patient-related factors, such as medical history. This factor determines whether the injury remains a self-limiting or transient event in otherwise healthy patients or progresses into more severe complications, such as persistent osteonecrosis, as demonstrated in the presented case.
In patients with a healthy immune status, NaOCl injuries typically present with acute pain and swelling, which generally resolve with conservative management [5,7,9,10,11,13,14,15,16]. In contrast, the presence of a high-risk factor, particularly immunocompromised states, such as in patients with Hodgkin’s lymphoma, can dramatically alter the clinical trajectory. In such individuals, a compromised inflammatory response and impaired ability to contain secondary infection may lead to more extensive soft-tissue destruction and involvement of the alveolar bone [17], even when procedural guidelines are followed and predisposing conditions and risk factors are carefully considered [18]. These complex cases often require surgical intervention, such as debridement of the necrotic bone, along with prolonged wound care and monitoring to aid healing, as was performed in the presented case. However, despite these efforts, the desired outcomes were not achieved.
Notably, no clinical cases documenting NaOCl injuries in patients with Hodgkin’s lymphoma have been identified in the existing literature. Consequently, there is no specific management protocol designed for this patient group. This poses a clinical challenge, as extended monitoring in such an individual may increase the risk of secondary infection over time, while early surgical intervention, such as debridement of the necrotic bone, could potentially worsen the condition by causing further bone damage.
Therefore, as the conventional management approach failed, this patient should be managed according to the most up-to-date treatment strategies, as suggested in situations similar to those involving Hodgkin’s lymphoma patients, where individuals exhibit a low immune status.
One of the recently established therapies for managing non-healing sockets, particularly in the context of medication-related osteonecrosis of the jaw (MRONJ) [19], is leukocyte–platelet-rich fibrin (L-PRF). This treatment has demonstrated promising outcomes in addressing non-healing sockets in non-malignant conditions, such as osteoporosis, and oncology patients, offering a potential solution for enhancing healing and improving clinical outcomes.
A retrospective observational study [19] was conducted to evaluate the effectiveness of L-PRF as an adjunct to surgical intervention in the treatment of patients at risk of MRONJ development. The study included 22 participants, who were allocated into two groups: Group A, which received surgery alone, and Group B, which received both surgery and L-PRF. Treatment success was determined based on complete soft-tissue healing and the absence of infection, inflammation, fistula formation, or exposed bone. The results demonstrated that 100% of patients in Group B achieved complete healing, in contrast with 54.5% of patients in Group A. The study concluded that L-PRF is a promising adjunct to the surgical management of MRONJ, providing favorable treatment outcomes and enhanced healing potential. A similar study [20] found that none of the patients in the L-PRF group developed established MRONJ, while five high-risk patients in the control group presented with MRONJ during follow-up. The study concluded that L-PRF may be effective in preventing MRONJ following dental extractions and also introduced a management protocol for these individuals.
Another group of bone necrosis and non-healing sockets is observed in osteoradionecrosis of the jaws (ORNJ), a severe and complex complication that arises following head and neck radiation therapy. In the management of ORNJ, one promising therapeutic option is the combination of pentoxifylline and tocopherol (PENTO). A systematic review [21] was conducted to assess the efficacy of PENTO in the treatment of ORNJ. The review revealed that PENTO treatment resulted in complete mucosal coverage with no exposed bone in patients, with success rates ranging from 16.6% to 100%, depending on the study. Additionally, clinical improvement or disease stabilization was reported in 7.6% to 66.6% of patients, while disease progression occurred in 7.6% to 32% of cases across five studies. The findings of the review suggest that PENTO may effectively achieve complete disease control in a significant proportion of patients.
Another treatment approach for ORNJ involves addressing radiation tissue injury. Hyperbaric oxygen therapy (HBOT) has been proposed as a potential treatment for such complications, owing to its ability to enhance blood flow to irradiated tissues. A Cochrane systematic review [22] was conducted to evaluate the effectiveness and risks of HBOT in treating or preventing late radiation tissue injury. The review found that HBOT is associated with improved outcomes in managing osteonecrosis. Additionally, it appears to reduce the risk of osteoradionecrosis following tooth extraction, indicating its potential benefit as an adjunctive therapy for patients with radiation-induced complications.
These adjunctive management strategies have been utilized in the treatment of various medical conditions, such as MRONJ and ORNJ, which share similar underlying pathophysiologies of NaOCl injury. Additionally, these conditions exhibit notable parallels to the present case, particularly in the manifestation of bone necrosis and delayed wound healing in immunocompromised patients.
The pathophysiology of NaOCl injury is predominantly attributed to its potent cytotoxic effects on living tissues. When NaOCl is accidentally extruded beyond the confines of the root canal during endodontic procedures, it comes into direct contact with surrounding vital tissues, leading to a cascade of harmful biological responses. NaOCl induces hemolysis by disrupting the integrity of red blood cells and releasing their intracellular contents into the surrounding tissues, thereby contributing to the disruption of the local tissue environment [14]. Additionally, NaOCl causes the ulceration of the affected tissue, leading to a compromised mucosal barrier [14]. The resultant disruption of the mucosal integrity creates a vulnerable site where microorganisms can more easily penetrate the exposed underlying bone, potentially leading to secondary infection. One of the key mechanisms of injury is the inhibition of neutrophil migration, which diminishes the immune response and compromises the body’s ability to combat infection and initiate the healing process [14]. Furthermore, NaOCl inflicts damage to endothelial cells, disrupting vascular integrity, and fibroblast cells, hindering tissue repair and collagen synthesis [14].
As outlined in the 2022 update of the Position Paper by the American Association of Oral and Maxillofacial Surgeons on MRONJ, the pathophysiology of MRONJ is supported by several evidence-based theories. The pathophysiology of MRONJ is multifactorial, involving several interrelated mechanisms. One major factor is the inhibition of bone remodeling due to antiresorptive medications, which directly affect osteoclast formation, differentiation, and function, particularly following bone injury. Additionally, pre-existing inflammation or infection contributes significantly, with elevated levels of pro-inflammatory cytokines—especially at MRONJ lesion sites—supporting the pivotal role of inflammation in disease progression. Inhibition of angiogenesis also plays a key role, characterized by osteocyte death, secondary to reduced blood flow, and a notable decrease in the microvessel density during the early stages of bone healing. Immune dysfunction, such as that caused by chemotherapy, further exacerbates the condition by altering the number and distribution of T-cell populations. Lastly, genetic predisposition has been implicated, with specific single-nucleotide polymorphisms identified as being associated with an increased risk of developing MRONJ [23].
The pathogenesis of ORNJ is primarily driven by the progressive changes induced by radiation therapy. A key mechanism involves the development of hypovascularity, hypocellularity [24], and hypoxia [21] in the irradiated bone. These changes compromise the tissue’s ability to regenerate and resist injury, initiating a chronic fibro-atrophic process characterized by fibrosis, reduced tissue elasticity, and impaired wound healing [24]. This leads to the bone and surrounding soft tissues becoming fragile and highly susceptible to necrosis, particularly following trauma, such as tooth extractions [24]. While microorganisms do play a role in exacerbating the condition, their contribution is relatively minor compared with the primary causes of hypovascularity and hypocellularity. Infection can worsen the clinical manifestation of ORNJ [25].
Therefore, the management strategies for MRONJ and ORNJ may be considered applicable in the present case, given the shared elements in their underlying pathophysiological mechanisms. L-PRF [26,27], one of the proposed strategies in the present case, is an autologous platelet concentrate, and regenerative biomaterial composed of a dense fibrin matrix containing high concentrations of platelets and leukocytes. It demonstrates considerable potential in promoting tissue repair through the gradual release of key growth factors, such as platelet-derived growth factor (PDGF), transforming growth factor (TGF), vascular endothelial growth factor (VEGF), and epithelial growth factor (EGF). These molecules collectively enhance angiogenesis, bone regeneration, and soft-tissue healing while also supporting hemostasis and tissue maturation without eliciting an inflammatory response. The fibrin matrix of L-PRF, with its tetra-molecular structure, serves as a biodegradable scaffold containing cytokines and stem cells, facilitating microvascularization and directing epithelial cell migration during the healing process.
Pentoxifylline, a methylxanthine derivative, exerts its antifibrotic effect through multiple mechanisms, including the inhibition of tumor necrosis factor-alpha (TNF-α), promotion of vasodilation, enhancement of erythrocyte deformability, and suppression of fibroblast proliferation [21]. Additionally, it increases the activity of collagenase enzymes, thereby facilitating extracellular matrix degradation [21]. Tocopherol (vitamin E), a potent antioxidant, complements these effects by inhibiting oxidative stress and downregulating the expression of procollagen genes, which contributes to the reduction in fibrotic tissue formation [21]. Together, pentoxifylline and tocopherol (PENTO) demonstrate a synergistic interaction, enhancing their overall antifibrotic efficacy.
HBOT has been proposed as a modality to enhance tissue quality, facilitate wound healing, and prevent the breakdown of irradiated tissues. It is defined as the medical use of 100% oxygen delivered at pressures exceeding 1 atmosphere absolute. The procedure involves placing the patient within a sealed hyperbaric chamber, where the ambient pressure is elevated while the patient breathes pure oxygen [22]. This results in a substantial increase in the partial pressure of oxygen in the lungs, bloodstream, and tissues. One of the key therapeutic outcomes of HBOT is the stimulation of angiogenesis, thereby promoting neovascularization within previously irradiated and hypoxic tissues [22].
Although no studies to date have directly investigated the use of these adjunctive management strategies in the context of NaOCl injuries, their therapeutic objectives—particularly the promotion of mucosal coverage over exposed bone—suggest potential applicability in such cases, especially when the patient is immunocompromised due to underlying medical conditions or ongoing treatment, as demonstrated in the presented case.
The dental management of patients with compromised immune systems presents unique challenges. These challenges arise not from the procedures themselves but from the complexities of managing complications in these patients. The current case emphasizes the necessity of careful consideration and expertise in treating such patients. Inexperienced clinicians should exercise caution when managing these cases, as complications could lead to long-term issues without effective management solutions. Hodgkin’s lymphoma, in particular, requires specialized attention due to the significant immune compromise associated with the condition. Therefore, a comprehensive and well-coordinated approach is crucial for the successful management of dental complications in this patient group. In this context, it may be advisable to consider the adjunctive management strategies discussed, as they could potentially aid in resolving the complications and promoting optimal healing. However, further well-designed research is required to evaluate the effectiveness of the proposed adjunctive management approaches and determine their suitability for use in such cases as Hodgkin’s Lymphoma.
4. Conclusions
This case report highlights a challenging clinical scenario commonly encountered in dental practice. While many dental procedures are straightforward, the medical history, particularly in immunocompromised patients, can present significant challenges. It is recommended that such patients be referred to specialists rather than managed by less-experienced clinicians in order to avoid potential long-term complications. The management approaches employed in other conditions, such as MRONJ, may offer valuable insights for managing similar cases to the presented case. Furthermore, a standardized management protocol should be established for handling such cases to ensure optimal patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fedorowicz Z. Nasser M. Sequeira-Byron P. de Souza R.F. Carter B. Heft M. Irrigants for non-surgical root canal treatment in mature permanent teeth Cochrane Database Syst. Rev.20122012 CD 00894810.1002/14651858.CD 008948.pub 222972129 PMC 11635403 · doi ↗ · pubmed ↗
- 2Pelka M. Petschelt A. Permanent mimic musculature and nerve damage caused by sodium hypochlorite: A case report Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod.2008106 e 80e 8310.1016/j.tripleo.2008.05.00318602848 · doi ↗ · pubmed ↗
- 3Witton R. Brennan P.A. Severe tissue damage and neurological deficit following extravasation of sodium hypochlorite solution during routine endodontic treatment Br. Dent. J.200519874975010.1038/sj.bdj.481241415980834 · doi ↗ · pubmed ↗
- 4Silva T.D.B. Ferreira C.B.T. Leite G.B. Pontes J.R.M. Antunes H.S. Oral manifestations of lymphoma: A systematic review Ecancermedicalscience 20161066510.3332/ecancer.2016.66527594910 PMC 4990057 · doi ↗ · pubmed ↗
- 5Serper A. Özbek M. Çalt S. Accidental sodium hypochlorite-induced skin injury during endodontic treatment J. Endod.20043018018110.1097/00004770-200403000-0001315055439 · doi ↗ · pubmed ↗
- 6Gatot A. Arbelle J. Leiberman A. Yanai-Inbar I. Effects of sodium hypochlorite on soft tissues after its inadvertent injection beyond the root apex J. Endod.19911757357410.1016/S 0099-2399(06)81725-51812208 · doi ↗ · pubmed ↗
- 7Akay N. Şimşek G. TaşB.M. KılıçR. Inadvertent injection of sodium hypochlorite to oral mucosa Eur. J. Rhinol. Allergy 20192323410.5152/ejra.2019.57969 · doi ↗
- 8Faras F. Abo-Alhassan F. Sadeq A. Burezq H. Complication of improper management of sodium hypochlorite accident during root canal treatment J. Int. Soc. Prev. Community Dent.2016649349610.4103/2231-0762.19293927891318 PMC 5109866 · doi ↗ · pubmed ↗