Ultra-High-Frequency Ultrasound Mapping of the Superficial Circumflex Iliac and Superficial Inferior Epigastric Vessels: An Anatomical Study
Spencer Chia-Hao Kuo, Ryo Karakawa, Hirofumi Imai, Shintaro Kagimoto, Yukio Seki, Nobuko Suesada, Hidehiko Yoshimatsu, Tomoyuki Yano

TL;DR
This study uses ultra-high-frequency ultrasound to map blood vessels in the lower abdomen for better surgical planning in breast reconstruction.
Contribution
The study demonstrates the effectiveness of ultra-high-frequency ultrasound in reliably detecting superficial vessels for reconstructive surgery.
Findings
UHFUS reliably detects SCIA and SCIV in most patients.
SIEA is less consistently identified compared to SCIA and SCIV.
UHFUS provides precise vessel localization and sizing for safer surgeries.
Abstract
Background: The superficial vessel system in the lower abdomen, including the superficial circumflex iliac artery (SCIA) and superficial inferior epigastric artery (SIEA), is widely used in reconstructive microsurgery. Preoperative ultrasonography, particularly ultra-high-frequency ultrasound (UHFUS), enhances surgical planning by providing high-resolution imaging. This study aimed to utilize UHFUS to examine the SCIA, SCIV, SIEA, and SIEV for reconstructive surgery planning. Methods: This prospective study included 25 patients undergoing free DIEP flap breast reconstruction. Patients with horizontal lower abdominal scars were excluded. Preoperative UHFUS, using a 48 MHz transducer, was performed to map and measure the superficial branch of SCIA (sSCIA), SCIV, SIEA, and SIEV. The vessel location, diameter, depth, and course were documented and analyzed. Results: Twenty-five female…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
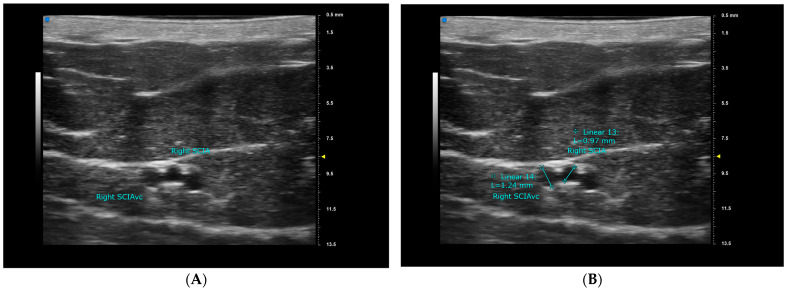 Figure 1
Figure 1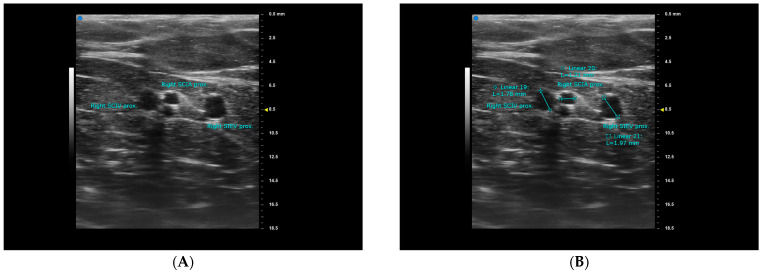 Figure 2
Figure 2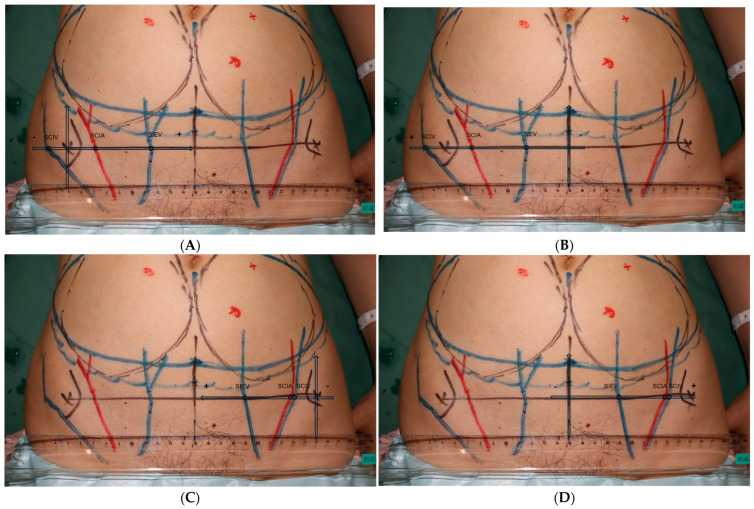 Figure 3
Figure 3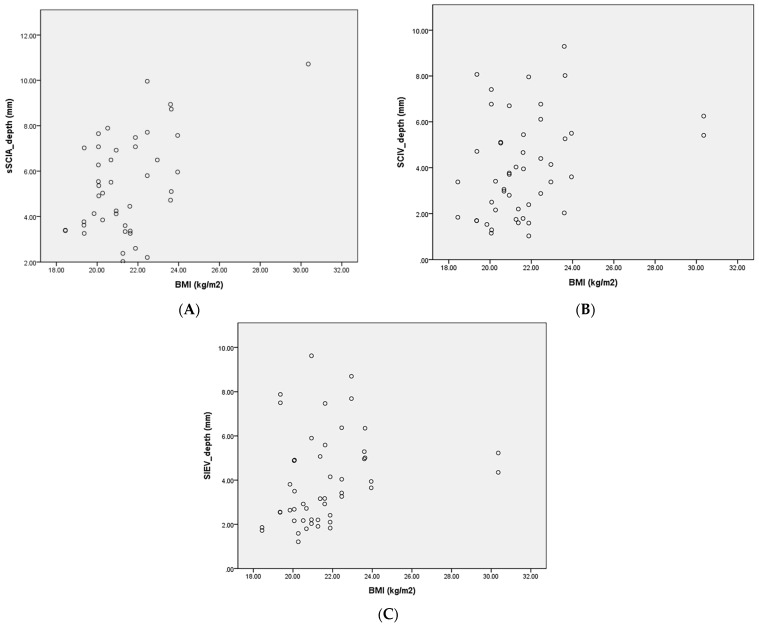 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReconstructive Surgery and Microvascular Techniques · Body Contouring and Surgery · Surgical site infection prevention
1. Introduction
The superficial vessel system of the lower abdomen has gained popularity and is now widely used in reconstructive microsurgery. The superficial circumflex iliac artery perforator (SCIP) flap is supplied by the superficial circumflex iliac artery (SCIA) and vein (SCIV), and has been applied in the reconstruction of the upper and lower extremities, head and neck, trunk, and even the breast [1,2,3,4,5,6,7,8,9]. The SCIA can arise from the femoral artery, the superficial femoral artery, the deep femoral artery, or the lateral circumflex artery. It generally runs parallel to the inguinal ligament and bifurcates into the superficial branch (sSCIA), which gives off perforators to the groin skin, and the deep branch (dSCIA) which gives off branches to the sartorius muscle, the iliac bone and perforators to the skin around the ASIS.
A similar flap from the lower abdomen can also be harvested based on the superficial inferior epigastric artery (SIEA) [10,11,12]. The SIEA can originate independently from the common femoral artery, or form a common trunk with the SCIA. It generally runs superiorly and medially, passing superficial to the inguinal ligament and traveling within the subcutaneous tissue of the lower abdominal wall. The superficial inferior epigastric vein (SIEV) has also been widely recognized as the main drainer of the superficial system dominated deep inferior epigastric perforator (DIEP) flap.
Ultrasonography has been widely utilized in the surgical planning of reconstructive microsurgery. Conventional high-frequency ultrasound devices typically operate at frequencies of 15–18 MHz, which are highly operator-dependent, making it challenging to obtain precise imaging of small anatomical structures [13]. The ultra-high-frequency ultrasound (UHFUS) system, with frequencies up to 48 MHz and even as high as 70 MHz, provides a resolution as fine as 30–50 μm, allowing for the more precise imaging of small structures. It is frequently used in the planning of lymphatic surgeries and in the detailed assessment of vasculature in reconstructive microsurgery [14].
The aim of this study was to utilize UHFUS in the anatomical examination of the sSCIA, SCIV, SIEA, and SIEV. With the aid of UHFUS, we are able to obtain high-resolution images of the lower abdominal vasculature, allowing for a comprehensive study that covers the location, diameter, depth, and course of the superficial vessels in the lower abdomen.
2. Materials and Methods
This study was approved by the ethical review board of the Cancer Institute Hospital of the Japanese Foundation for Cancer Research. We conducted a prospective study involving patients who underwent free DIEP flap breast reconstruction between 1 January 2024 and 30 July 2024. Patients with horizontal scars over the lower abdomen were excluded from this study. UHFUS examinations were performed during the surgical design and marking process the day before the operation. Patient information, including age, sex, BMI, and smoking status, was retrieved from medical records.
All UHFUS exams were performed by the first author, S.C. Kuo, using the Vevo MD machine (FUJIFILM VisualSonics, Inc., Toronto, ON, Canada). On the day before surgery, the primary surgeon completed the DIEP flap design and recipient site design for all patients. Following the design, each patient was placed in a supine position and evaluated with the Vevo MD machine using a 48 MHz transducer. First, the vertical midline and the horizontal line at the level of the anterior superior iliac spine (ASIS) were marked. We then searched for the sSCIA, its vena comitans (VC), SCIV, SIEA, VC of SIEA, and SIEV at the ASIS level. The vessels were traced proximally and distally until they became too deep or too small to be captured with clear images. If neither the sSCIA nor the SIEA could be identified, a second staff member (R. Karakawa) would repeat the exam and verify the results. Images were captured for further measurements at the ASIS level and at the most proximal point possible (Figure 1A and Figure 2A). The locations of the vessels were marked with marking pens, and by connecting the most proximal point of each vessel to its location at the ASIS level, we were able to determine the vessel’s course. The course was classified as either superior-lateral, superior, or superior-medial. Finally, the vessel diameter was measured after completing the entire exam (Figure 1B and Figure 2B). All measurements were taken three times and then averaged to minimize bias. All images with mapped vessels were processed using Image J v.1.4 (National Institutes of Health, Bethesda, MD, USA) to measure the distances from the vessels to the ASIS and the midline (Figure 3). Data were processed and analyzed using SPSS v.22 statistical software (IBM, Armonk, NY, USA). The normality of the data was evaluated using the Shapiro–Wilk test, and the data were presented as mean ± standard deviation (SD) or median ± interquartile range (IQR) accordingly.
3. Results
Table 1 summarizes the general information of the patients included in this study. A total of 25 patients, representing 50 hemiabdomens, were included. The patients ranged in age from 41 to 66 years, and all were female. The mean BMI was 21.6 kg/m^2^, with a range from 18.4 kg/m^2^ to 30.4 kg/m^2^. Five patients (20%) were smokers. All patients had at least one detectable superficial artery in the lower abdomen, and 96% of the patients had at least one detectable superficial artery on both sides of the lower abdomen.
Table 2 shows the anatomical characteristics of the superficial branch of the superficial circumflex iliac artery, the VCs, and the superficial circumflex iliac vein, as measured using UHFUS. The sSCIA was detectable in 48 hemiabdomens (96%). The average diameter of the vessel at the ASIS level and when traced proximally was 0.76 ± 0.25 mm and 0.97 ± 0.25 mm, respectively. The average depth of the vessel at the ASIS level was 5.42 ± 2.13 mm (Figure 4A). Correlation analysis between BMI and the sSCIA depth at the ASIS level showed a weak to moderate positive correlation: as BMI increases, the vessel depth tends to increase (Spearman’s rho (ρ) = 0.306; p-value = 0.046). A total of 43 VC (86%) were detected running alongside the sSCIA, with an average diameter of 0.94 ± 0.37 mm at the ASIS level and 1.34 ± 0.58 mm when traced proximally. The average distance from the sSCIA to the ASIS (“hot zone”) and to the midline was 18.71 ± 15.44 mm and 91.02 ± 15.89 mm, respectively, at the ASIS level. Most sSCIAs (98%) followed a superior lateral pedicle course. At least one dominant SCIV was detectable in 48 hemiabdomens (96%). The average diameter of the SCIV at the ASIS level and when traced proximally was 1.72 ± 0.60 mm and 2.07 ± 0.48 mm, respectively. The average depth of the SCIV at the ASIS level was 3.66 ± 3.29 mm (Figure 4B). Correlation analysis between BMI and the SCIV depth at the ASIS level also showed a weak to moderate positive correlation (Spearman’s rho (ρ) = 0.319; p-value = 0.027). The average distance between the SCIV and the ASIS (“hot zone”) was 10.46 ± 14.71 mm, and the distance between the sSCIA and the SCIV was 15.47 ± 19.10 mm. All SCIVs followed a superior lateral pedicle course.
Table 3 shows the anatomical characteristics of the superficial inferior epigastric artery, the VCs, and the superficial inferior epigastric vein, as measured using UHFUS. The SIEA was detectable at the ASIS level in only 11 hemiabdomens (22%). The diameter of the vessel at the ASIS level and when traced proximally was 0.63 ± 0.22 mm and 1.05 ± 0.20 mm, respectively. The average depth of the vessel at the ASIS level was 4.94 ± 3.60 mm. Eight accompanying veins were detected running alongside the SIEA, with an average diameter of 0.64 ± 0.28 mm at the ASIS level and 1.35 ± 1.06 mm when traced proximally. The average distance from the SIEA to the ASIS and to the midline was 51.32 ± 20.57 mm and 50.92 ± 22.26 mm, respectively, at the ASIS level. About half of the SIEAs (6/11, 55%) followed a superior medial pedicle course. At least one dominant SIEV was detectable in all hemiabdomens. The average diameter of the SIEV at the ASIS level and when traced proximally was 2.18 ± 0.48 mm and 2.39 ± 0.57 mm, respectively. The average depth of the vessel at the ASIS level was 3.46 ± 2.80 mm (Figure 4C). Correlation analysis between BMI and the SIEV depth at ASIS level showed a moderate positive correlation (Spearman’s rho (ρ) = 0.375; p-value = 0.007). The average distance between the SIEV and the midline (“hot zone”) was 47.94 ± 10.11 mm. A total of 38 out of 50 SIEVs (76%) followed a superior medial pedicle course.
The vessel diameter was compared between smokers and non-smokers (Table 4). The p-values were 0.78 and 0.96, respectively, for sSCIA at the ASIS level and proximal. For SIEA at the ASIS level and proximal, the p-values were 0.08 and 0.93, respectively. No significant difference was found between smokers and non-smokers.
4. Discussion
The first vascularized iliac bone flap based on the SCIA was reported by Taylor and Watson in 1978 [15]. In 2004, Koshima et al. introduced the SCIP flap, which has gradually become more commonly used in reconstructive microsurgery [7,8,16,17,18,19]. According to anatomical studies based on intraoperative findings and computed tomographic angiography (CTA), the SCIA arises from the femoral artery, the superficial femoral artery, the deep femoral artery, or the lateral circumflex artery [20]. It then bifurcates into the sSCIA, which gives off perforators to the groin skin, and the deep branch (dSCIA), which gives off branches to the sartorius muscle, the iliac bone and perforators to the skin around the ASIS [20,21,22]. A cadaveric dissection study published by Yoshimatsu et al. suggested that the bifurcation point of the sSCIA and the dSCIA could be identified within 2 cm of a fixed site—6 cm from the pubic tubercle to the ASIS and 3 cm caudal from that point—in 85% of the specimens [16]. In the current study, the “hot zone” for locating the sSCIA pedicle is 3.27 to 34.15 mm medial to the ASIS (Table 2). Today, the SCIP flap, whether based on the sSCIA, the dSCIA, or both superficial and deep branches in a chimeric design, is widely used in the reconstruction of various anatomical regions.
A similar flap from the lower abdomen can also be harvested based on the SIEA, commonly referred to as the SIEA flap [10,11,12]. Compared to the workhorse DIEP flap for breast reconstruction, the SIEA flap or the SIEA-SCIA combined flap spares the fascia and rectus muscle dissection, leaving only an abdominoplasty scar, which minimizes donor site morbidity. An anatomical study of the SIEA system, based on CTA studies published by Kita et al., confirmed that the SIEA was present in 92.4% of the hemiabdomens they reviewed [23]. It originated independently from the common femoral artery in 59.7% of the hemiabdomens, and it formed a common trunk with the SCIA in 32.6% of the cases. The SIEV was present in 99.3% of the hemiabdomens [23]. In the current study, the SIEA was detectable by Vevo MD at the ASIS level in only 22% of the hemiabdomens. This detection rate differs from the previous CTA study published by Kita et al., likely due to the design of Vevo MD, which is optimized for examining superficial body structures. As a result, some SIEAs may be too deep to be detected at the ASIS level. In contrast, CTA studies trace the vessels starting from their point of origin. Additionally, the examination was conducted while the patient was awake in the outpatient clinic, so the examination time was not unlimited. Although the result differs from that of the prior CTA study, we believe this number reflects the real-time condition of living Asian women in the clinical setting, which is a strength of this prospective study on living human subjects.
In the current study, the sSCIA was detectable by Vevo MD at the ASIS level in 96% of the hemiabdomens, and at least one set of detectable superficial arteries and veins was found in the lower abdomen of all patients. The superficial arteries detected at the ASIS level typically had an average diameter of over 0.5 mm, which, based on our experience, often measures greater than 1 mm when dissected proximally near their origin. With the help of Vevo MD, we can map out sizable superficial arteries and include one of the arteries in our flap. On the other hand, venous drainage is often the primary concern when planning a flap based on the superficial vessel system of the lower abdomen. Since the average distance between the dominant artery and vein is usually not large, we tend to include and position the dominant superficial vein at the center of the flap. Although there is ongoing debate regarding the necessity and value of preoperative imaging, we believe that this methodology can provide additional guidance when planning an sSCIA-based or SIEA-based flap.
One specific strength of our study is its prospective design and the use of the UHFUS system on living human subjects, which allowed us to generate the “hot zone” for detecting vessels at the ASIS level based on these data. Ultrasonography holds an indispensable role as it provides real-time evaluation, allowing us to assess the vessels directly on the patient in different positions. The UHFUS enhances this capability by offering a high resolution, which enables the more precise measurement of vessel diameter. However, there are some limitations to this study. First and foremost, the absence of a comparison with a gold-standard modality such as computed tomography angiography limits our ability to evaluate diagnostic performance metrics, including sensitivity, specificity, the positive predictive value, negative predictive value, and overall accuracy. Future studies should aim to address the diagnostic accuracy of UHFUS through a direct comparison with established imaging techniques. Second is the operator-dependent nature of ultrasonography, which can introduce some measurement bias. To mitigate this, we repeated each measurement three times using the Vevo MD machine. Thirdly, the Vevo MD is designed to examine superficial body structures, making precise diameter measurements for structures deeper than 20 mm somewhat challenging. Tiny structures located deeper than 25–30 mm may go undetected. Therefore, vessel evaluation may become more challenging in very obese patients. Lastly, this is a single-center study with a study population limited to a single race and gender. Further studies with larger and more diverse populations are needed to obtain more comprehensive data.
5. Conclusions
In conclusion, all patients in the current study had at least one sizable set of superficial arteries and veins in the lower abdomen. When a free lower abdominal skin flap transfer is indicated, preoperative ultrasonography enables the precise mapping of the flap’s pedicle vessels, confirmation of the pedicle diameter, and the design of a well-vascularized flap. This approach simplifies flap harvest and enhances patient safety during free flap transfer surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yoshimatsu H. Yamamoto T. Hayashi N. Kato M. Iida T. Koshima I. Reconstruction of the ankle complex wound with a fabricated superficial circumflex iliac artery chimeric flap including the sartorius muscle: A case report Microsurgery 20173742142510.1002/micr.2251826513645 · doi ↗ · pubmed ↗
- 2Yano T. Yoshimatsu H. Karakawa R. Fuse Y. Kuramoto Y. Shibata T. Suesada N. Miyashita H. Use of a combined SIEA and SCIP based double pedicled abdominal flap for breast reconstruction Microsurgery 20214131932610.1002/micr.3072733682221 · doi ↗ · pubmed ↗
- 3Yamamoto T. Saito T. Ishiura R. Iida T. Quadruple-component superficial circumflex iliac artery perforator (SCIP) flap: A chimeric SCIP flap for complex ankle reconstruction of an exposed artificial joint after total ankle arthroplasty J. Plast. Reconstr. Aesthetic Surg. JPRAS 2016691260126510.1016/j.bjps.2016.06.01027423250 · doi ↗ · pubmed ↗
- 4Yamamoto T. Daniel B.W. Rodriguez J.R. Kageyama T. Sakai H. Fuse Y. Tsukuura R. Yamamoto N. Radical reduction and reconstruction for male genital elephantiasis: Superficial circumflex iliac artery perforator (SCIP) lymphatic flap transfer after elephantiasis tissue resection J. Plast. Reconstr. Aesthetic Surg. JPRAS 20227587088010.1016/j.bjps.2021.08.01134756554 · doi ↗ · pubmed ↗
- 5Ou C.L. Li J. Zhou X. Luo X.C. Zou Y.G. Repair of multiple hand defects with superficial circumflex iliac artery perforator flap Injury 20235494094610.1016/j.injury.2023.01.01636669944 · doi ↗ · pubmed ↗
- 6Lichtenberg N.J. Taylor D.M. Pedicled chimeric superficial circumflex iliac artery perforator (SCIP) flap with external oblique fascia for vesicocutaneous bladder fistula repair: A case report and literature review on the utility of pedicled chimeric SCIP Microsurgery 202444 e 3113810.1002/micr.3113838343009 · doi ↗ · pubmed ↗
- 7Hong J.P. Sun S.H. Ben-Nakhi M. Modified superficial circumflex iliac artery perforator flap and supermicrosurgery technique for lower extremity reconstruction: A new approach for moderate-sized defects Ann. Plast. Surg.20137138038310.1097/SAP.0b 013e 3182503 ac 523187712 · doi ↗ · pubmed ↗
- 8Goh T.L.H. Park S.W. Cho J.Y. Choi J.W. Hong J.P. The search for the ideal thin skin flap: Superficial circumflex iliac artery perforator flap--a review of 210 cases Plast. Reconstr. Surg.201513559260110.1097/PRS.000000000000095125357163 · doi ↗ · pubmed ↗