Constant direct oral anticoagulants therapy melts away multiple floating thrombi in the aorta
Ryo Ikeda, Arudo Hiraoka

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
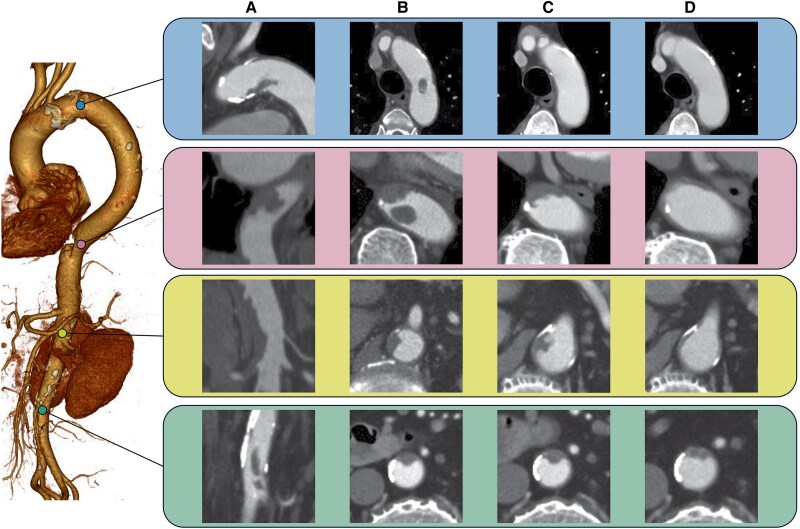 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Thrombus and Embolism · Aortic aneurysm repair treatments · Parathyroid Disorders and Treatments
An 89-year-old man presented to the emergency department with abdominal pain. Computed tomography showed multiple aortic floating thrombi (MAFT) (Panels A and B) and transthoracic echo showed a floating thrombus in the descending aorta (see Supplementary material online, Video S1). Laboratory tests showed a platelet count of 120 × 10^4^/μL and bone marrow aspiration revealed primary myelofibrosis leading to abnormal thrombocytosis. Direct oral anticoagulants (DOACs) and antiplatelet agents were administered for MAFT and thrombocytosis. We followed the process of MAFT resolution for 4 weeks (Panel C) and 8 weeks (Panel D) without visceral branches and peripheral arterial emboli. MAFT is a rare disease that can be catastrophic due to visceral branches and peripheral arterial embolism.
The aetiology of MAFT is often unclear, however many of the cases have been associated with atherosclerosis of the aorta and abnormal coagulation function is reported to be one of the risk factors for MAFT.^1^ There are several reports of surgical thrombectomy and TEVAR for aortic floating thrombus,^2,3^ which are highly invasive and can result in the spread of thrombus to the visceral branches and lower limbs. In addition, these procedures for MAFT have a risk of spinal code injury. On the other hand, there are only a few reports on the conservative treatment of MAFT with DOACs. We chose a DOAC instead of warfarin or LMWH, since DOACs have a rapid onset of therapeutic effect and do not require dose control until they are effective. Additionally, DOACs are also superior in terms of adherence to long-term anticoagulation therapy. We have successfully managed MAFT conservatively with DOACs, which can be a useful option to avoid excessive invasiveness and complications when the aortic condition is not abnormal and the culprit disease is known and treatable.
Supplementary Material
ytaf244_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Weiss S, Bühlmann R, von Allmen RS, Makaloski V, Carrel TP, Schmidli J, et al Management of floating thrombus in the aortic arch. J Thorac Cardiovasc Surg 2016;152:810–817.27160939 10.1016/j.jtcvs.2016.03.078 · doi ↗ · pubmed ↗
- 2Giovanni N, Daniela M, Giovanni M, Maria Teresa O, Silvia S, Davide F, et al Endovascular treatment of thoracic aortic floating thrombus in patients presenting with acute lower limb ischemia. Int J Vasc Med 2011;2011:604362.21331173 10.1155/2011/604362 PMC 3034922 · doi ↗ · pubmed ↗
- 3Scott DJ, White JM, Arthurs ZM. Endovascular management of a mobile thoracic aortic thrombus following recurrent distal thromboembolism: a case report and literature review. Vasc Endovascular Surg 2014;48:246–250.24347279 10.1177/1538574413513845 · doi ↗ · pubmed ↗