Prosthetic Hip Dislocations After Total Hip Replacement: A Retrospective Study
Bratati Bandyopadhyay, Sunandan Datta, Mohammed Hussain, Muhammad Raza, Maham Mansoor, Rachala Madhu, Sudipta Kar

TL;DR
This study examines hip dislocations after total hip replacement, finding that noncompliance with post-surgery guidelines is a major cause.
Contribution
The study provides insights into the causes and management of prosthetic hip dislocations through a retrospective analysis.
Findings
Posterior dislocations were most common, occurring in 60% of cases.
Noncompliance with hip positioning guidelines was the main cause of dislocation.
36.67% of dislocated hips required revision surgery.
Abstract
Introduction Total hip replacement (THR) dislocation occurs when the prosthetic joint components completely separate, indicating a failure in the intended mechanics of the hip joint established by the prosthesis. This complication poses significant challenges for patients and surgeons and financially burdens healthcare systems. Methods This retrospective observational study evaluated cases of prosthetic hip dislocation within our health board that required manipulation under anesthesia (MUA) from January 1, 2021, to March 5, 2024. A total of 60 patients met the inclusion criteria. Patient data were collected from hospital records using dedicated clinical software platforms. Results The patients were divided into two groups based on the treatment received: MUA and revision THR. The Mann-Whitney U test showed no significant difference in the time to dislocation between the groups,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
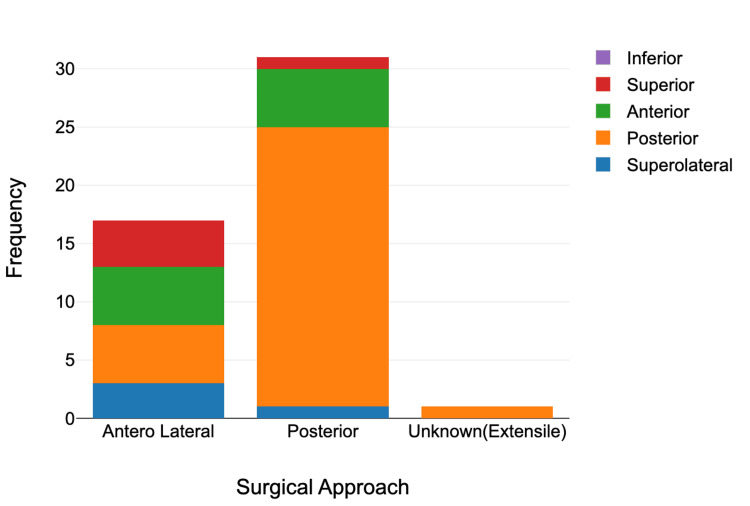 Figure 1
Figure 1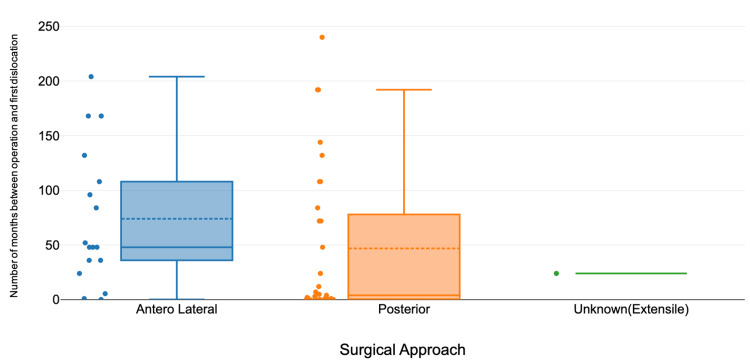 Figure 2
Figure 2| Surgical approach | Most common type of dislocation (count) | Average number of dislocations | Chi-square value | F statistic | Chi-square p-value | ANOVA p-value |
| Anterolateral | Anterior (5) | 2.118 | 12.961 | 0.298 | 0.044 | 0.744 |
| Posterior | Posterior (24) | 2 | ||||
| Unknown (extensile) | Posterior (1) | 1 |
| Procedure | N (total number) | Median (months) | Mean (months) | SD (months) | Test statistic (U value) | p-value |
| MUA | 38 | 24 | 70.66964865 | 89.65504502 | 381 | 0.909 |
| THR revision | 22 | 36 | 67.04114286 | 84.39297966 |
| Procedure | N (total number) | Median | Mean | SD | Test statistic (U value) | p-value |
| MUA | 38 | 1 | 1.789474 | 1.473329 | 240.5 | 0.00351 |
| THR revision | 22 | 2.5 | 2.954545 | 1.758714 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopaedic implants and arthroplasty · Total Knee Arthroplasty Outcomes · Orthopedic Infections and Treatments
Introduction
Total hip replacement (THR) dislocation is defined as the complete separation of prosthetic joint components, indicating a failure of the mechanical function intended by the prosthesis [1]. This complication presents substantial challenges for both patients and surgeons and imposes a considerable financial burden on healthcare systems [2]. The incidence of post-THR dislocation is influenced by multiple factors, including surgical technique, patient-specific characteristics, and the type of implant used. Studies conducted at major institutions report dislocation rates ranging from 0.3% to 3% following primary THR for osteoarthritis [3]. In comparison, revision procedures and implant exchanges demonstrate significantly higher dislocation rates, reaching up to 28% [4].
Dislocation after THR has profound implications, contributing to both physical and emotional distress and substantially reducing patients’ quality of life. Furthermore, it is one of the leading causes of early revision surgeries [5,6].
The primary objective of this study was to analyze cases of prosthetic hip dislocation within our health board that required manipulation under anesthesia (MUA) following both primary and revision THR. Our study also takes a look at the difference in dislocation episodes and timing following both primary and revision THR. Additionally, this study aimed to assess the proportion of these cases that necessitated revision surgery as a definitive intervention and to identify the most common causes of dislocation in order to develop effective prevention strategies.
Materials and methods
This retrospective observational study was conducted as an audit to evaluate cases of prosthetic hip dislocation within our health board requiring MUA. The study covered the period from January 1, 2021, to March 5, 2024, identifying 60 patients who met the inclusion criteria.
Patient data were obtained from electronic hospital records using Clinical Workstation, Ormis, and the Welsh Clinical Portal, which provided detailed information on patient presentations, surgical histories, and procedures.
Inclusion criteria were prosthetic hip dislocation following THR managed with MUA during either an emergency department visit or inpatient stay. Exclusion criteria included dislocations after hip hemiarthroplasty, native hip dislocations, and cases with incomplete data.
Study population
A total of 60 consecutive patients with prosthetic hip dislocation requiring MUA were included. Of these, 42 were male and 18 were female.
Data analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows, Version 22.0 (Released 2013; IBM Corp., Armonk, NY, USA). Continuous variables were summarized with means, medians, and IQRs; categorical variables were expressed as percentages. Mann-Whitney U and Kruskal-Wallis tests were used to assess nonparametric data. Categorical variables were compared using the chi-square test, and continuous variables using the one-way ANOVA test. Logistic regression analyzed associations with dislocation outcomes.
Results
The study population was divided into two groups based on definitive treatment: MUA or revision THR. A total of 60 patients experienced prosthetic hip dislocation requiring MUA. Of these, 48 dislocations followed primary THR, and 12 occurred after revision procedures. The mean patient age was 66.5 years, with a female predominance (42 females and 18 males). No significant sex-based differences in outcomes were observed.
Dislocation characteristics
Posterior dislocations were the most common, occurring in 37 cases (61.67%), followed by anterior in 11 cases (18.33%), superior in six cases (10%), superolateral in five cases (8.33%), and inferior dislocation in one case (1.67%). The posterior surgical approach was most frequently documented (32 cases), followed by anterolateral (17 cases). In 11 cases, the approach was unspecified, and in one case, the approach was mentioned extensile approach without any more details. There was no statistically significant association between surgical approach and dislocation type (Table 1, Figure 1). A chi-square test was used to evaluate the association between surgical approach and type of dislocation, both categorical variables. A one-way ANOVA compared the mean number of dislocations, a continuous variable, across different surgical approach groups.
Proportion and frequency of dislocation types by surgical approachA stacked bar chart illustrates both the proportion and frequency of prosthetic hip dislocations, categorized by dislocation type and surgical approach. Posterior dislocations were the most common, predominantly following the posterior approach. Fewer cases of anterior, superior, and superolateral dislocations were observed across all approaches. Dislocation types are color-coded as follows: green for anterior, orange for posterior, red for superior, and blue for superolateral.
The types of prostheses varied: 28 hips had uncemented implants, 10 were cemented, and 22 were hybrids. Dislocations were most commonly associated with femoral head sizes of 28 mm and 36 mm, while the 32 mm head size was associated with the fewest dislocations.
Dislocation episodes and timing
Of the 60 patients, 30 had a single dislocation episode, 12 had two, seven had three, and two patients experienced six and seven episodes, respectively. The mean time from index surgery to first dislocation was 69.3 months. The average age at first dislocation in the MUA group was 64.9 years (SD: 15.5), compared to 69.2 years (SD: 11.5) in the revision group. The mean time to first dislocation was 70.7 months in the MUA group and 67.0 months in the revision group. The average number of dislocations was 1.79 in the MUA group versus 2.95 in the revision group. The Mann-Whitney U test revealed no significant difference in the time to dislocation between primary and revision THR groups (p = 0.91); however, there was a statistically significant difference in the number of dislocations between the two groups (p = 0.004), as illustrated in Table 2 and Table 3.
Revision surgery was required in 22 cases (36.7%), while 38 patients (63.3%) were managed successfully with MUA. The Kruskal-Wallis test showed no statistically significant differences in time to first dislocation (H statistic: 4.582, p-value: 0.101) or number of dislocations (H statistic: 0.812, p-value: 0.666) across surgical approaches (Figure 2). Noncompliance with hip precautions was the most common cause of dislocation, followed by trauma and excessive range of motion.
Time to dislocation (from operation to first dislocation) in months according to surgical approachA boxplot comparing the time interval (in months) between index surgery and the first dislocation across different surgical approaches in patients undergoing THR. The anterolateral approach shows a broader IQR and a higher median time to dislocation compared to the posterior approach, suggesting greater variability and potentially a later onset of instability. Several outliers are observed in both groups, indicating cases of delayed dislocation. Dashed lines represent group means, while solid lines within the boxes indicate medians.THR, total hip replacement
Discussion
Dislocation is a leading cause of revision THR in the United States and ranks fourth in the United Kingdom [7,8]. Aseptic loosening is the most common cause of revision THR worldwide, followed by dislocation [9].
Dislocation risk factors can be categorized as patient specific, procedure specific, or implant related. Patient-related factors include advanced age, neurological conditions, and poor adherence to postoperative care [10,11]. Procedure-specific risks involve surgical approach, component positioning, soft tissue tension, and surgeon experience [12,13]. Implant-related factors - such as small head-neck ratios, over-hemispheric acetabular cups, and extended prosthetic heads - may predispose patients to impingement and subsequent dislocation. While larger femoral heads (≥36 mm) improve range of motion and stability, they may also cause secondary impingement between the femoral neck and pelvic bone. In our cohort, 28 mm and 36 mm heads were most frequently associated with dislocations [14,15].
Consistent with Christensen et al., who reported that 68% of hip dislocations were posterior [16], our study found that posterior dislocations comprised 61.67% of cases. Woolson and Rahimtoola reported a 3.2% dislocation rate across 10,500 THRs [17]. Notably, dislocation rates are higher after revision THR, with some studies reporting rates as high as 25% [18].
Dislocation timing is a key consideration. Fessy et al. observed that over 50% of dislocations occur within three months postoperatively [19], while Ali Khan et al. reported that 66% occurred within five weeks [20]. In contrast, our data showed only 20.7% of dislocations occurred within the first five weeks, possibly reflecting improvements in early rehabilitation and patient education. Late dislocations accounted for 36.2% of our cases. These are often attributed to polyethylene wear. Huten and Langlais estimated that 32% of dislocations occurred on average 11.3 years post-THR [21]. In our study, the mean time to late dislocation was 14.2 years, emphasizing the need for long-term follow-up.
Although Taunton et al. reported that the posterior approach was associated with the highest dislocation rates after primary THR [22], our study did not find a statistically significant association between surgical approach and number of dislocations. This suggests that patient factors and implant design may play a more prominent role. Our cohort had a mean of 2.22 dislocations per patient, consistent with the 2.81 reported by Blom et al. [23], underscoring the complexity of managing recurrent hip dislocations and the need for individualized treatment strategies.
Our study has several limitations due to its retrospective design. The modest sample size (n = 60) reduces statistical power and generalizability. Data extracted from multiple clinical systems may impact accuracy, depending on documentation consistency. Missing surgical approach data in 11 cases introduces potential bias, while unexamined factors such as implant positioning, surgeon-specific variables, patient comorbidities, rehabilitation compliance, and socioeconomic factors further limit the study’s conclusions on dislocation outcomes.
Conclusions
Prosthetic hip dislocation remains a challenging complication following both primary and revision THR surgeries. Our retrospective analysis of 60 patients reveals several important insights for future management and prevention. It was observed that the average number of dislocations was higher in the revision THR group as compared to the MUA group. Posterior dislocations were the most prevalent (60%), consistent with literature linking the posterior approach to greater instability; however, no statistically significant association was identified between the surgical approach and number of dislocations in our cohort. These findings reinforce the multifactorial nature of dislocation risk. Patient-related factors were frequently implicated, with noncompliance with postoperative precautions identified as the leading cause of early dislocation, followed by trauma and excessive range of motion. These findings support the critical role of patient education, structured rehabilitation, and adherence to movement restrictions in mitigating dislocation risk in the first few months after surgery. Discharge planning should include reinforcement of postoperative instructions and the provision of assistive devices where appropriate. Future multicenter studies are warranted to validate our findings and support the development of standardized protocols to minimize dislocation risk.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dislocation following total hip replacement Dtsch Arztebl Int Dargel J Oppermann J Brüggemann GP Eysel P 88489011120142559736710.3238/arztebl.2014.0884 PMC 4298240 · doi ↗ · pubmed ↗
- 2Hospital cost of treating early dislocation following hip arthroplasty Hip Int de Palma L Procaccini R Soccetti A Marinelli M 62672220122236250410.5301/HIP.2012.9059 · doi ↗ · pubmed ↗
- 3The dislocating hip: what to do, what to do J Arthroplasty Bourne BB Mehin R 1111141920041519056410.1016/j.arth.2004.02.016 · doi ↗ · pubmed ↗
- 4Risk factors for dislocation after revision total hip arthroplasty Clin Orthop Relat Res Wetters NG Murray TG Moric M Sporer SM Paprosky WG Della Valle CJ 41041647120132295623610.1007/s 11999-012-2561-7PMC 3549187 · doi ↗ · pubmed ↗
- 5Quality of life after dislocation of hip arthroplasty: a prospective cohort study on 319 patients with femoral neck fractures with a one-year follow-up Qual Life Res Enocson A Pettersson H Ponzer S Törnkvist H Dalén N Tidermark J 117711841820091971448610.1007/s 11136-009-9531-x · doi ↗ · pubmed ↗
- 6The National Joint Registry 18th Annual Report 2021 [Internet] Ben-Shlomo Y Blom A Boulton C London National Joint Registry 2021 http://pubmed.ncbi.nlm.nih.gov/35072993/35072993 · pubmed ↗
- 7Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030 J Bone Joint Surg Am Kurtz S Ong K Lau E Mowat F Halpern M 7807858920071740380010.2106/JBJS.F.00222 · doi ↗ · pubmed ↗
- 8The epidemiology of revision total knee and hip arthroplasty in England and Wales: a comparative analysis with projections for the United States. A study using the National Joint Registry dataset Bone Joint J Patel A Pavlou G Mújica-Mota RE Toms AD 1076108197-B 20152622482410.1302/0301-620X.97B 8.35170 · doi ↗ · pubmed ↗