Stent-Assisted Coiling in a Nickel-Allergic Patient
Shoichiro Tsuji, Yoji Kuramoto, Shinichi Yoshimura

TL;DR
A woman with a nickel allergy successfully underwent a brain aneurysm treatment using a nickel-containing stent without allergic reactions.
Contribution
Demonstrates safe use of nickel-containing stents in patients with confirmed nickel allergy.
Findings
No hypersensitivity reactions occurred after using a nickel-containing stent in a nickel-allergic patient.
The procedure was completed without neurological complications or need for allergy-suppressing medication.
Abstract
We report the case of a woman in her fourth decade of life with a known nickel allergy. She visited the previous clinic complaining of a headache. Head MRI was performed, which showed a right internal carotid artery aneurysm, and she was referred to our hospital for further treatment. We planned treatment using coiling embolization with a balloon catheter because we were afraid of allergic reactions against the nickel device. However, recused stenting was done during the procedure to prevent coil migration. After the treatment, there were no post-procedure neurological complications or hypersensitivity reactions due to nickel allergy. No medication was given to suppress the hypersensitivity reaction. The patient was discharged from the hospital with no complications. This case demonstrates that nickel-containing stents can be safely used in selected patients with confirmed nickel…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1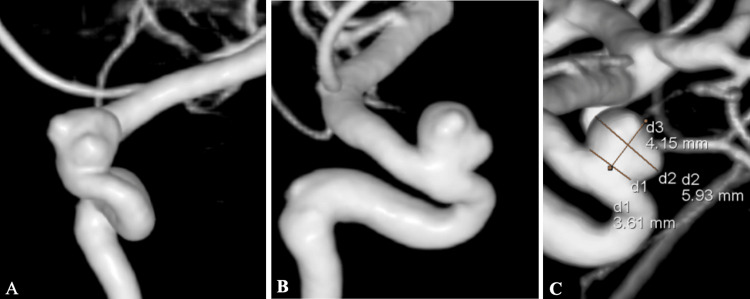 Figure 2
Figure 2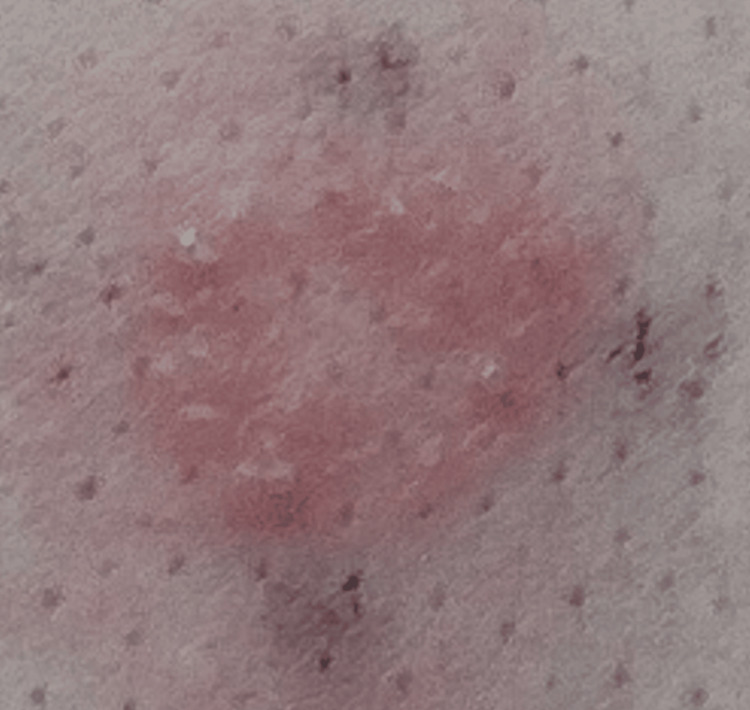 Figure 3
Figure 3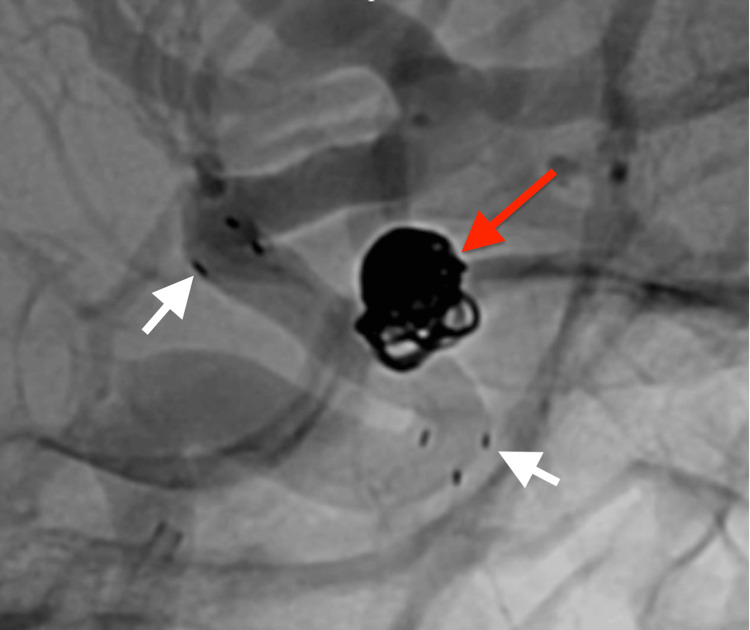 Figure 4
Figure 4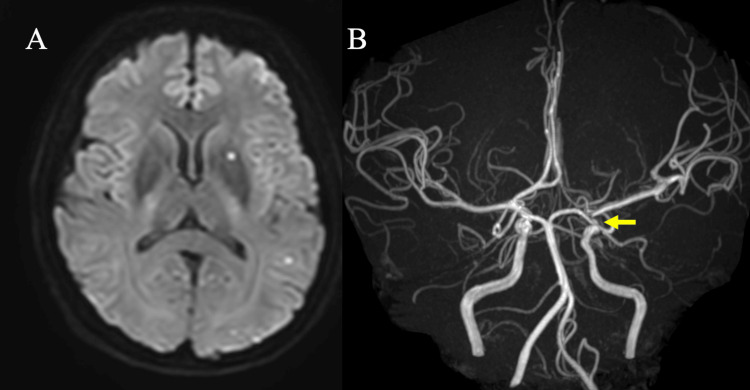 Figure 5
Figure 5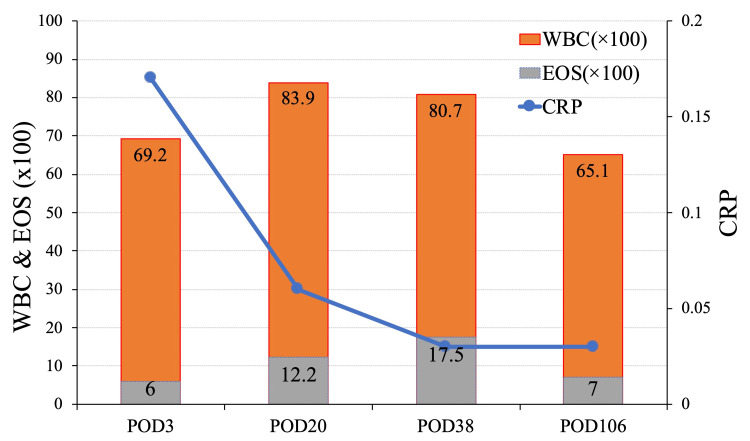 Figure 6
Figure 6| Study | Device | Location | Symptom-related nickel allergy | MRI findings | Treatment |
| Park et al. [ | Enterprise (Codman Neurovascular, Raynham, MA, USA) | Lt ICA C3 | Right-hand weakness | Multifocal white matter lesion | Steroid |
| Enterprise | Rt VA | Abducens nerve palsy, right facial palsy, dysphagia, sensory disturbance | Multifocal white matter lesion | Steroid | |
| Nakagawa et al. [ | Enterprise | Rt VA | Lt lower motor weakness, dizziness | Multifocal white matter lesion | Steroid |
| Neuroform EZ (Stryker Neurovascular, Fremont, CA, USA) | Lt ICA C2 | Convulsion | Multifocal white matter lesion | Steroid | |
| Ulus et al. [ | Enterprise | Lt MCA | Headache, visual disturbance | Multifocal white matter lesion | None |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsContact Dermatitis and Allergies
Introduction
Endovascular treatment of intracranial aneurysms has spread rapidly in the last 20 years, with typical treatment devices such as coils and Woven EndoBridge devices implanted in the aneurysm and stents such as vascular reconstruction devices (VRDs) to prevent coil deviation and flow diverters (FDs), which are made from a variety of metals. Therefore, metal allergy is one of the obstacles to the endovascular treatment. Nickel is one of the most common allergens for metal allergies and is used in stents such as VRDs and FDs, which are used intracranially to maintain strength with shape memory and flexibility. Patients with metal allergies should be warned to avoid using instruments containing the offending metal in their treatment. However, if any troubles happen during the endovascular procedure, we have no choice but to use devices containing the metal to avoid serious complications, even for patients with metal allergies. We report our experience with a patient with a metal allergy who underwent coil embolization and was assisted with a metal stent to avoid complications. We report this case because we believe that sharing this case may be helpful in the future for treating aneurysms in patients with metal allergy, especially nickel allergy.
Case presentation
A female patient in her 40s visited a local clinic complaining of a headache. There was no identifiable cause of headache on MRI. However, a left paraclinoid aneurysm was incidentally found (Figure 1), and she was referred to our hospital for treatment. She had a past medical history of allergic rhinitis and hyperlipidemia. The aneurysm was located at the left internal carotid artery (ICA)’s anterior side of the supraclinoid portion. It had blebs; the maximum size was 5.62mm, the neck was 4.55mm, and the dome neck ratio was 1.4 (Figure 2).
Initial MRA at previous hospitalOblique view of initial MRA showing a left paraclinoid aneurysm (white arrow).MRA, magnetic resonance angiography
Pre-treatment 3D-RAs. (a) Frontal view. (b) Lateral view. (c) The size of the aneurysm.The neck was 3.61mm, the dome was 5.93mm, and the height was 4.15mm.3D-RA, three-dimensional rotation angiogram
The left ophthalmic artery did not originate from the left ICA but from the middle meningeal artery (MMA), and this might be the cause of blindness during craniotomy surgery.
The patient also had some allergic reactions to shellfish, including crab, kiwi fruit and pineapple, and certain metals. Before the treatment, patch testing against several metals, including nickel, chromium, stannum, iridium, silver, and cobalt, was performed. Apart from nickel, there was no reaction, but a strong positive result for nickel was observed (Figure 3).
Patch test for nickel.The patient exhibited a cutaneous hypersensitivity to nickel.
Therefore, we decided to avoid using nickel devices, and a balloon-supported technique was selected for this wide-neck aneurysm.
The patient had been taking aspirin 100 mg and prasugrel 3.75 mg for two weeks prior to this treatment. In the evaluation using the LTA method, platelet aggregation was effectively suppressed. Additionally, the VerifyNow™ system (Instrumentation Laboratory, Bedford, MA, USA) was used to assess antiplatelet effects. The aspirin response unit was 403 and the P2Y12 response unit was 100, meaning they adequately inhibited platelet activity. Under local anesthesia, we set the guiding sheath to the left ICA from her right femoral artery. A balloon catheter navigated around the aneurysm. Next, a microcatheter was navigated in the aneurysm with an intermediate catheter. Then, coil embolization was started with a dilated balloon. Good obliteration was achieved until the second coil was inserted. The microcatheter dislodged while inserting the third coil. We then exchanged the microcatheter and continued after reinserting a new one into the aneurysm. However, the sixth coil protruded to the ICA and wobbled. We were concerned that the coils might migrate distally, and thus we deployed a stent (Neuroform Atlas, Stryker Neurovascular, Fremont, CA, USA) to prevent the coils from migrating. After deploying the stent, we got acceptable obliteration (Raymond-Roy occlusion classification 1; Figure 4), and there was no missing branch among the intracranial arteries. After the treatment, we followed up on the patient’s condition at our High Care Unit overnight. As there were no symptoms or abnormal findings on the final angiogram, the patient was followed up without a steroid or an anti-allergic agent. Three days after endovascular treatment, MRI showed only scattered small asymptomatic infarcts, acceptable as post-treatment, and magnetic resonance angiography showed no intracranial arterial occlusion (Figure 5).
Post-treatment digital angiogramThe final digital angiogram after stent-assisted coiling. The distal and proximal tips of the stent are indicated by white arrows, and the embolized aneurysm is indicated by a red arrow. Raymond-Roy occlusion score was class 1.
Post-operative MRI imagesThe MRI performed three days post-treatment revealed only several hyperintensity spots on the DWI (A). There were no findings indicative of vessel occlusion due to stent placement, and a left-paraclinoid aneurysm was not identified on the magnetic resonance angiography (B, yellow arrow).
There were no abnormal findings in the brain suggestive of an allergic reaction. She was discharged with no neurological deficit or any other symptoms. On blood examination, transient elevation of white blood cells (WBC) and eosinophils (EOS) was observed but gradually decreased, and the C-reactive protein (CRP) increased slightly postoperatively but remained within a normal range (Figure 6).
Time course of blood sampling testsOn blood examination, transient elevation of WBC and EOS increased transiently, and CRP remained within normal range.WBC, white blood cell; EOS, eosinophil; CRP, C-reactive protein
Over a 24-month outpatient follow-up period, the patient's condition had not changed, and there was no edema or recurrence of the aneurysm on MRI.
Discussion
Due to nickel allergy, balloon-assisted coil embolization of a paraclinoid ICA aneurysm was planned. However, during the procedure, the coil protruded into the ICA, necessitating stent placement. Fortunately, the patient was asymptomatic, with only mildly elevated WBC, EOS, and CRP, and no abnormalities were observed on the MRI over a 24-month follow-up period.
Nickel is a rare metal with stable corrosion resistance in a variety of harsh environments. Pure nickel is difficult to handle, and it is used as stainless steel composed of iron, chromium, and nickel in a wide range of products, from cookware to construction, military, and aerospace applications.
Nickel allergy affects nearly 10-15% of the world's population [1]. Nickel allergy is the most common metal allergy worldwide, is more common in women, and is increasing [2,3]. It has been reported that the incidence rate is 5-20% for women and 2-4% for men [4]. Women have higher risks because of ear piercing, the most common cause of sensitization [5]. Despite this, there are only five reported cases of nickel-related adverse events after intracranial aneurysm endovascular treatment [1]. Such cases are infrequent, and there is a discrepancy between the prevalence of nickel allergy and the incidence rate of allergic reactions after treatment.
Although no postoperative allergy was observed in this case, nickel-induced delayed hypersensitivity reactions have been reported to cause stent restenosis, stent thrombosis, and reversible intraparenchymal changes in allergic patients [6-8]. Diffuse cerebral edema with allergic spasms or focal neurological deficits such as hemiplegia and visual impairment may occur after the implantation of nickel-containing metal in cerebral vessels in patients with nickel allergy, and these symptoms occur one month after treatment [9]. These are treated with high-dose methylprednisolone and improved finally (Table 1) [2,7,9-11].
Moreover, there are no reports of dermatological symptoms after stent-assisted coil embolization. Extracranially, several months after implantation of nitinol-containing stents in lower limb arteries or knee prostheses in patients with nickel allergy, there have been reports of marked skin symptoms and swelling, as well as increased CRP, WBC, and EOS [12]. The stent we used had the largest stent strut among VRDs, i.e., the smallest contact area with the vessel. Again, the intracranial stent had a very low absolute amount of metal compared to stents used in other places, which may have prevented a strong allergic reaction. The use of nickel-containing alloys in intracranial devices is essential for endovascular procedures, and most devices are composed of nitinol. This is due to nitinol's exceptional elasticity and shape memory effect. Nickel is one of nitinol's significant components, accounting for 55%, which supports its shape memory with intracranial VRDs [2].
Generally, paraclinoid aneurysm is treated with surgical clipping or endovascular therapy. An alternative treatment for patients with nickel allergy, where the use of stents or other devices made of various alloys containing nickel other than platinum coils is contemplated, is craniotomy clipping. Clips and bone fixation plates used in clipping procedures are made of titanium and, therefore, do not contain nickel. When treated by surgical clipping for aneurysms with a pterional approach, including IC paraclinoid aneurysms, ophthalmic arteries branching ectopically from the MMA should be noted, as they account for 3.5% of cases [13]. Surgical clipping has a high risk of intraoperative injury to the MMA, and there have been reports of blindness [14]. In this situation, endovascular therapy is often favorable. In contrast, thromboembolic complications of endovascular treatment of paraclinoid aneurysms have been reported to range from 2.8% to 5.4%, with no postoperative neurological symptoms [15].
Our case has a limitation. According to the previous report, some reactions due to nickel allergy happened one month after endovascular procedures, but there is also a report that it came 12 months later [2]. In our case, follow-up MRI two years post-procedure demonstrated no abnormal findings, and the patient remained asymptomatic. However, the potential for a delayed allergic reaction exists, and thus we need to observe the patient's condition continuously to check whether the patient has some complications.
Conclusions
We reported the case of unavoidable stent-assisted coiling for a patient who had a nickel allergy. There were no complications, including MRI, except for transient elevation of EOS. Furthermore, the patient presented with an ophthalmic artery branching off the middle meningeal artery, which could have resulted in a reduction in ophthalmic artery blood flow and subsequent blindness following craniotomy. While severe nickel allergic complications may not be confirmed in every nickel allergy patient, it is of the utmost importance that careful observation be conducted on a consistent long-term basis in the future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nickel-related adverse reactions in the treatment of cerebral aneurysms: a literature review World Neurosurg Tsang AC Nicholson P Pereira VM 14715311520182968451710.1016/j.wneu.2018.04.073 · doi ↗ · pubmed ↗
- 2Epidemiology of nickel sensitivity: retrospective cross-sectional analysis of North American Contact Dermatitis Group data 1994-2014 J Am Acad Dermatol Warshaw EM Zhang AJ De Koven JG 7017138020193034216010.1016/j.jaad.2018.09.058 · doi ↗ · pubmed ↗
- 3The epidemiology of contact allergy in the general population--prevalence and main findings Contact Dermatitis Thyssen JP Linneberg A MennéT Johansen JD 2872995720071793774310.1111/j.1600-0536.2007.01220.x · doi ↗ · pubmed ↗
- 4Blue jean button dermatitis. Nickel allergy presenting as a periumbilical rash Postgrad Med Cerveny KA Jr Brodell RT 798379-80, 8311220021246218710.3810/pgm.2002.11.1354 · doi ↗ · pubmed ↗
- 5Nickel sensitization in adolescents and association with ear piercing, use of dental braces and hand eczema. The Odense Adolescence Cohort Study on Atopic Diseases and Dermatitis (TOACS)Acta Derm Venereol Mortz CG Lauritsen JM Bindslev-Jensen C Andersen KE 3593648220021243073510.1080/000155502320624096 · doi ↗ · pubmed ↗
- 6Stent thrombosis caused by metal allergy complicated by protein S deficiency and heparin-induced thrombocytopenia: a case report and review of the literature Thromb J Konishi T Yamamoto T Funayama N 251320152620709710.1186/s 12959-015-0055-z PMC 4512022 · doi ↗ · pubmed ↗
- 7Reversible intracranial parenchymal changes in MRI after MCA aneurysm treatment with stent-assisted coiling technique; possible nickel allergy Neuroradiology Ulus S Yakupoğlu A Kararslan E Işlak C Siva A Koçer N 8978995420122265348110.1007/s 00234-012-1048-2 · doi ↗ · pubmed ↗
- 8Nickel and molybdenum contact allergies in patients with coronary in-stent restenosis Lancet Köster R Vieluf D Kiehn M 1895189735620001113038710.1016/S 0140-6736(00)03262-1 · doi ↗ · pubmed ↗