Outcomes of cemented taper slip versus composite beam femoral stems in total hip arthroplasty: A systematic review and meta-analysis
Loay A. Salman, Harman Khatkar, Jawad Derbas, Mohammed F.A. Radi, Jehad Feras AlSamhori, Wael Al-Atout, Osama Z. Alzoubi, Ghalib Ahmed

TL;DR
This study compares two types of hip implants and finds that one has better outcomes in avoiding certain complications.
Contribution
The study provides a systematic review and meta-analysis comparing cemented collared composite beam and collarless taper slip femoral stems in hip replacement surgery.
Findings
The collarless taper slip stems had significantly lower aseptic loosening and periprosthetic joint infection rates compared to collared composite beam stems.
Other outcomes like periprosthetic fractures, revision rates, and dislocation were similar between the two stem types.
The results suggest that taper slip stems may offer better performance in specific failure modes.
Abstract
The aim of this systematic review and meta-analysis was to compare the outcomes of cemented collared composite beam (CB) and collarless taper slip (TS) femoral stems in total hip arthroplasty (THA). Four databases were searched from inception to August 2023 for original studies that compared the outcomes of cemented CB and TS femoral stems following THA. The primary outcome was aseptic loosening, and the secondary outcomes were periprosthetic fractures, instability, dislocation, revision, survivorship, and periprosthetic joint infection (PJI). This review was conducted in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A total of 11 studies with 730,769 hips were included, with a mean follow-up period of 8.48 ± 6.07 years and average MINORS (Methodological Index for Non-Randomized Studies) score of 17.36 ± 1.86. There was a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
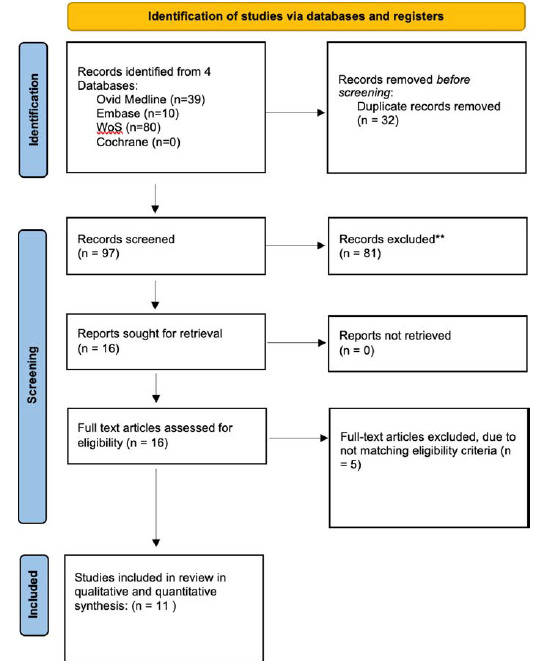 Figure 1
Figure 1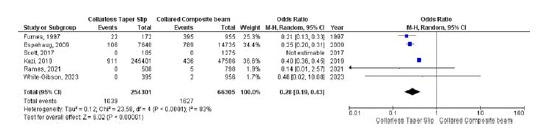 Figure 2
Figure 2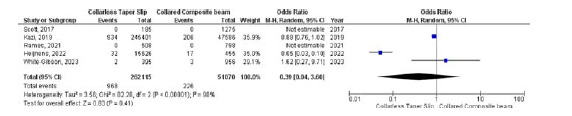 Figure 3
Figure 3 Figure 4
Figure 4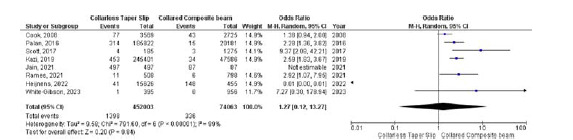 Figure 5
Figure 5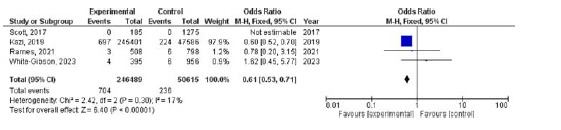 Figure 6
Figure 6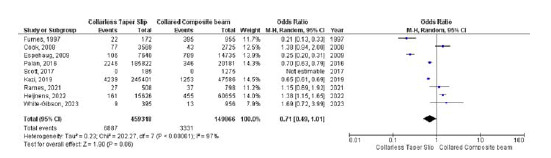 Figure 7
Figure 7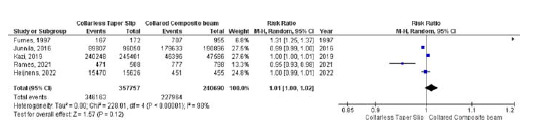 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopaedic implants and arthroplasty · Orthopedic Infections and Treatments · Total Knee Arthroplasty Outcomes
Introduction
Total hip arthroplasty (THA) is a commonly performed orthopedic surgery, with more than 500,000 and 95,677 THA performed annually in the USA and UK, respectively.^ 1,2 ^ Understanding the underlying biomechanical and inflammatory nature of osteoarthritis (OA) is crucial,^ 3 ^ with THA considered as the treatment of choice for end-stage hip osteoarthritis.^ 4 ^
There are various designs and fixation methods for total hip prosthesis. In cemented THA, the design of the femoral stem follows one of two biomechanical principles to ensure stability in the femoral canal under constant axial load. The first design follows the “force-closed” or “polished-taper slip” (TS) principle, while the second uses the “shape-closed” or “composite beam” (CB) principle.^ 5 ^ The most popular example on the CB is the original Charnley (DePuy International) stem, while examples of TS stem designs include Exeter V40 (Stryker), CPT stem (Zimmer), and C-Stem (DePuy International).
Several studies have shown equivalent results in both types of stems with excellent overall implant survivorship and different failure modes in both groups. Therefore, the choice between a CB and a tapered slip stem remains controversial.^ 6,7 ^ The Charnley stem provided excellent outcomes with long survival rates due to its low friction properties.^ 8 ^ The Exeter and Exeter V40 stems also showed favorable long-term survival rates.^ 9,10 ^ However, limitations included low statistical power and short duration of the follow-up period. Therefore, robust evidence is required to thoroughly compare outcomes between the two groups.
The aim of this study was to compare the clinical outcomes, including aseptic loosening, dislocation, instability, periprosthetic fracture, periprosthetic joint infection (PJI), revision rate, and survivorship between cemented CB and TS femoral stems. We hypothesize that there is no significant difference in outcomes and complication rates between the two groups.
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.^ 11 ^ The protocol was pre-registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD42023458881.
Search strategy
Four online databases (Ovid MEDLINE, Embase, Web of Science and Cochrane Library databases) were searched from inception to August 1, 2023 to identify all studies that compared collared CB versus collarless TS femoral stems in THA. The following keywords and their derivatives were included: Taper Slip OR Exeter AND Composite Beam OR Charnley AND Femoral Stem AND Cemented AND Total hip arthroplasty.
Eligibility criteria
Studies were considered eligible if they met the following criteria: (1) comparison of any of the clinical outcomes of interest between the CB and TS groups, (2) all types of cemented femoral stems (regardless of the design or manufacturer), (3) primary THA, and (4) published in the English language.
Exclusion criteria included the following: (1) failure to compare outcomes of both femoral stem types, (2) cementless or revision THA, (3) studies with incomplete or unextractable data for review, and (4) review articles and preclinical and case reports.
Study screening
Two authors conducted the screening process independently and blindly by screening the titles and abstracts of the retrieved articles. Full-text review was performed for studies that met the pre-specified eligibility criteria. Any disagreements between the two authors were resolved by a third senior author. The references of the included articles were manually searched to ensure that all relevant studies were included.
Data extraction
Two authors independently extracted the data from the included articles. The following data were collected: study characteristics, patient demographics, study year, design and location, mean patient age, number of participants and hips, age, type of total hip replacement, type of femoral stem, manufacturer, type of prosthesis and bearings used, mean follow-up period, number of revisions, survivorship, complications, mode of revisions, patient-reported outcomes (if any), statistical tests used, and the conclusion of each study.
Quality assessment
Two authors conducted the methodological quality assessment blindly and independently using the methodological index for non-randomized studies (MINORS) criteria.^ 12 ^ According to the MINORS criteria, comparative and non-comparative studies can achieve a maximum score of 24 and 16, respectively. Comparative studies are graded as very low quality (0–6), low quality (7–10), fair quality (11–16), good quality (16–20), and high quality ( ≥ 20). Non-comparative studies are grade as very low quality (0–4), low quality (5–7), fair quality (8–12), and high quality ( ≥ 13).^ 12 ^
Results
Study selection
The search across multiple databases yielded a total of 129 articles. After removing 32 duplicates, 97 records underwent initial screening based on their titles and abstracts, excluding 81 records. Ultimately, 16 papers were eligible for full-text review. As a result, 11 studies met the eligibility requirements and were included in both qualitative and quantitative analyses. The process is shown in Figure 1 using the PRISMA flowchart.
Characteristics of the included studies
A total of 11 research papers were included. These studies were published between 1997 and 2023 and originated primarily from various regions, including the UK (three articles), the USA (two articles), Norway (two articles), and Scotland, Finland, the Netherlands, and Ireland (one article each). Of the 11 included studies, 10 were retrospective and one was prospective. The total number of hips examined across the studies was 730,769. The mean follow-up duration was 8.48 ± 6.07 years. Table 1 summarizes the characteristics of the studies.
Quality assessment (level of evidence and risk of bias)
We evaluated the methodological quality of the included studies using the MINORS criteria, reflecting how well each study adhered to predefined methodological quality standards. Higher scores indicate more robust methodological rigor. The MINORS criteria scores of the included studies ranged from 14 to 20, with an average of 17.36 ± 1.86 (out of 24), indicating an overall low risk of bias. A summary of the quality assessment according to the MINORS criteria is presented in Table 2.
Aseptic loosening
Six studies compared the occurrence of aseptic loosening between the collarless TS and collared CB groups. The odds of aseptic loosening were significantly lower in the collarless TS group than in the collared CB group (OR 0.28, 95% CI 0.19–0.43, p < 0.001). Due to significant heterogeneity (I ^ 2 ^ = 83%, p < 0.001), a random-effects model was used (Figure 2).
Dislocation
Five studies were included to assess any differences in dislocation between the collarless TS and collared CB arms. Due to the high heterogeneity (I ^ 2 ^ = 98%, p < 0.001), a random-effects model was used. No significant differences were found in dislocation rates between the two groups (OR 0.39, 95% CI 0.04–3.60, p < 0.001) (Figure 3).
Recurrent instability
Three studies were included to examine the differences in the occurrence of instability between collarless TS and collared CB stems. No significant differences in instability were observed between the two groups (OR 1.86, 95% CI 0.04–4.24, p = 0.14). The heterogeneity was low (I ^ 2 ^ = 0.0%, p = 0.77) (Figure 4).
Periprosthetic fracture
Eight studies evaluated the odds of periprosthetic fracture occurring between collarless TS and collared CB groups, with no significant differences between the two groups (OR 1.27, 95% CI 0.12–13.27, p = 0.84). However, there was significant heterogeneity (I ^ 2 ^ = 99%, p < 0.001), leading to the use of a random-effects model (Figure 5).
Periprosthetic joint infection
Four studies were included to examine the differences in the occurrence of PJI between the two femoral stem types. The use of a collarless TS was associated with a significantly lower likelihood of PJI compared to a collared CB (OR 0.61, 95% CI 0.53–0.71, p < 0.001). The heterogeneity was low (I ^ 2 ^ = 17%, p = 0.30) (Figure 6).
Revision rate
Nine studies were analyzed to assess the differences in revision rates between the two groups. No significant differences were observed between the two groups (OR 0.71, 95% CI 0.49–1.01, p = 0.06). High heterogeneity was found (I ^ 2 ^ = 97%, p < 0.001) (Figure 7).
Implant survivorship
Five studies reported implant survival rates. No difference in the implant survival rates was found between collarless TS and collared CB stems (RR 1.01, 95% CI 1.00–1.02, p = 0.12) (I ^ 2 ^ = 98%, p < 0.001) (Figure 8).
Publication bias
The Egger bias test revealed insignificant publication bias in the assessment of aseptic loosening (p = 0.5701), dislocation (p = 0.2393), instability (p = 0.4860), periprosthetic fracture (p = 0.2080), PJI (p = 0.0756), revision (p = 0.1726), and implant survivorship (p = 0.2609).
Discussion
This systematic review represents the most comprehensive evaluation of the two types of cemented stems available in the current literature, with the use of registry-level data allowing for a high number of included cases. The use of registry data facilitates comparison and detection of subtle statistical signals within the dataset. However, understanding the clinical relevance of such signals sometimes remains unclear.^ 6,23,24 ^
The main finding of this analysis supports the notion that CB stems are at higher risk of aseptic loosening than TS stems. Although no definitive mechanism for this can be theorized, CB stems are considered to be less involving in terms of surgical technique, relying on an adequately thick cement mantle that binds the bone to the cement and the cement to the stem.^ 5,6,22 ^ In order for the stem to function as a CB construct, a perfect bonding between the implant and the cement mantle must always be maintained.^ 6,22,25 ^ If a perfect bond is maintained, shear forces at the cement–bone interface promotes the production of third-body wear particles, thereby accelerating wear particle-induced periprosthetic osteolysis.^ 25 ^ Furthermore, the study by Kärrholm et al. demonstrated that CB stems exhibit subsidence, thus negating the underpinning design philosophy of a CB-type stem.^ 26,27 ^ The need for meticulous cementing when using CB stems may increase the propensity for loosening, but there are no clinical studies that support this notion. To fully evaluate this finding, implant retrieval-based studies examining the mechanism of CB stem failure are needed.
The associated difference in the rate of aseptic loosening between stem types cannot be easily explained by biomechanical principles, as the underlying mechanism currently remains unclear. Focused research is required to further evaluate this discrepancy.
The consensus in the literature supports the notion that TS stems have a higher rate of periprosthetic fracture than CB stems.^ 18,28–33 ^ This is due to a purported mechanism whereby the polished stem does not remain fixed to the cement mantle, as the stem is designed to subside in a controlled manner within the mantle during loading.^ 19 ^ This then leads to the formation of hoop stresses and subsequent long spiral fracture patterns.^ 18,19,30 ^ The results of this review did not support this conclusion, with no significant differences being found. This finding reinforces the notion that concern about TS stems and periprosthetic fractures may currently be unfounded, with further basic scientific work required to evaluate whether the fracture mechanism in TS stems conforms to the current hypothesis.
Equivalence between the parameters of dislocation rate, instability, all-cause revision, and survivorship was determined from the findings of this review. This supports the notion that either the CB or TS stem can be considered a viable long-term option, with both guiding principles of design providing a reliable, repeatable femoral stem for patients.The work of this study has elicited a finding that has not been previously reported in the current literature. The PJI rate was significantly lower in TS stems than in CB stems. Given the current understanding of the philosophy of stem design, implantation, and implant performance, no clear explanation for this finding can be definitively hypothesized. Principally, PJI is multifactorial, with host, surgical, and implant factors all contributing to an eventual diagnosis. Isolating the role of stem choice within this area may improve the overall understanding of PJI etiology.^ 34,35 ^ The influence of stem design does not appear to be a current area of PJI-related research. However, given the possible discrepancy in infection rates, further work may be required to evaluate this difference.
This review lacked specific data on specific stems, with a focus on the philosophy of stem design. For each individual TS or CB stem, the design philosophy, stem dynamics, and implantation technique vary between manufacturers. Although the design philosophy is useful at the basic science level, it should be evaluated along with specific stem designs. This could enable a more crystallized performance of specific stems in the future. To date, two randomized trials have been performed, directly comparing the Charnley stem with double- and triple-tapered TS designs (Exeter and C-stem) and both studies demonstrating equivalence between stem types at 2 and 5 years.^ 1,5,25 ^ It clear that future analysis building on the work of this study should include appropriate analysis of individual stem types to more clearly define any differences between specific CB/TS stem types. This should be performed at the registry level to ensure a sufficiently significant sample size and to correctly identify any discrepancies between stem types.
Additionally, beyond the design of the femoral stem, the outcomes and long-term performance of implants in THA are influenced by various other factors. These include surgical elements such as the cementing technique and specific surgical approach, as well as patient-related factors such as age, activity level, and the underlying reason for undergoing THA.^ 36,37 ^ These factors have been associated with implant survivorship and the overall risk of complications, as well as can play a confounding role in outcome assessment.
Conclusion
This study found a significantly higher incidence of aseptic loosening and PJI in the CB stem type compared to the TS group. However, no differences were observed between the groups in terms of periprosthetic fracture, revision rate, survivorship, instability, or dislocation. These findings should be considered cautiously due to potential confounding factors.
Competing interests
The authors have no conflicts of interest to declare.
Authors’ contributions
All authors contributed to the conception and design of the study. LAS and MFAR performed material preparation, literature review, data collection, and quality assessment. JS performed the statistical analysis. LAS, HK, WA, JS, and OZA wrote the first draft of the manuscript and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American Join. Replacement Registry (AJRR): 2022 Annual Report.Rosemont, IL:America Academy of Orthopaedic Surgeons (AAOS)[online]. 2022. [Accessed 1 June 2023]Available from: https://www.aaos.org/registries/publications/ajrr-annual-report/
- 2Registry NJ National Joint Registry 17th Annual Report. [online]. 2020. [Accessed 1 June 2023]Available from: https://www.njrcentre.org.uk
- 3Salman LA Ahmed G Dakin SG Kendrick B Price A Osteoarthritis: a narrative review of molecular approaches to disease management Arthritis Res Ther 2023 Feb 1825127 doi: 10.1186/s 13075-023-03006-w 36800974 PMC 9938549 · doi ↗ · pubmed ↗
- 4Hussein IH Zalikha AK Tuluca A Crespi Z El-Othmani MM Epidemiology of obese patients undergoing revision total knee arthroplasty: understanding demographics, comorbidities, and propensity weighted analysis of inpatient outcomes J Am Acad Orthop Surg Glob Res Rev 2022 Feb 1662 e 21.00263 doi: 10.5435/jaaosglobal-d-21-00263 PMC 885362335171855 · doi ↗ · pubmed ↗
- 5Scheerlinck T Casteleyn PP The design features of cemented femoral hip implants Bone Joint Surg Br 2006 Nov 88111409–1418 doi: 10.1302/0301-620x.88b 11.1783617075082 · doi ↗ · pubmed ↗
- 6Kazi HA Whitehouse SL Howell JR Timperley AJ Not all cemented hips are the same: a register-based (NJR) comparison of taper-slip and composite beam femoral stems Acta Orthop 2019 May 6903214–219doi: 10.1080/17453674.2019.158268030838914 PMC 6534220 · doi ↗ · pubmed ↗
- 7Espehaug B Furnes O Engesæter LB Havelin LI 18 years of results with cemented primary hip prostheses in the Norwegian Arthroplasty Register: concerns about some newer implants Acta Orthop 2009 Aug 1804402–412doi: 10.3109/1745367090316112419857178 PMC 2823190 · doi ↗ · pubmed ↗
- 8Berry DJ Harmsen WS Cabanela ME Morrey BF Twenty-five-year survivorship of two thousand consecutive primary Charnley total hip replacements: factors affecting survivorship of acetabular and femoral components JBJS 2002 Feb 1842171–17710.2106/00004623-200202000-0000211861721 · doi ↗ · pubmed ↗