Therapeutic drug monitoring for antimicrobial agents for people living with HIV (TAP)
Christine Sekaggya-Wiltshire, Eva Agnes Laker Odongpiny, Francis Williams Ojara, Isabella Kyohairwe, Reuben Kiggundu, Hope Mackline, Catriona Waitt, Aida N Kawuma, Allan Buzibye, Noela Owarwo, Francis Kakooza, Andrew Kambugu, Lambert Assoumou, Isabella Kyohairwe

TL;DR
This study aims to measure antibiotic concentrations in people living with HIV to improve treatment effectiveness through drug monitoring and dose adjustments.
Contribution
The study introduces therapeutic drug monitoring for antimicrobial agents in HIV-positive individuals, focusing on optimizing dosing for tuberculosis treatment.
Findings
Antibiotic concentrations will be measured in PLWH using validated analytical methods.
Dose adjustments based on drug monitoring will be tested for TB treatment in a subset of participants.
Abstract
Antimicrobial resistance (AMR) is a growing health concern, particularly in Africa, and is predicted to be the leading cause of death after cancer by 2050. Factors like overuse or inappropriate use of antibiotics, contribute to this crisis. People living with HIV (PLWH) are particularly vulnerable to AMR with potential drug-drug interactions between antiretroviral and antimicrobial agents against common organisms like Mycobacterium tuberculosis. There is limited data on the concentrations of commonly used antimicrobial agents in people living with HIV in resource-limited settings. Therapeutic Drug Monitoring (TDM) offers a promising approach to optimize antibiotic dosing and improve treatment outcomes for those with sub-optimal drug concentrations. TDM has been recommended for PLWH on anti-tuberculosis treatment due to sub-optimal drug concentrations found in a significant proportion of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
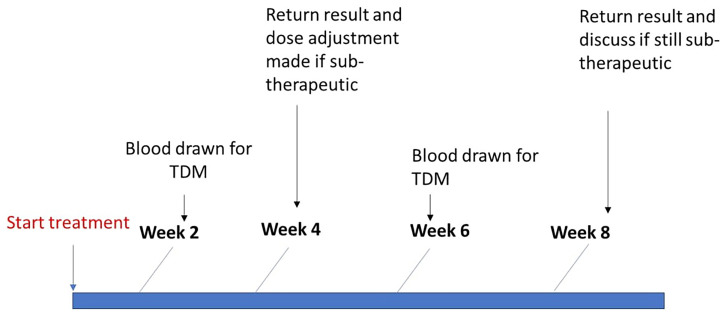 Figure 1
Figure 1| Protocol Activity | Screen and enrolment | Day 2 +/-3days | End antibiotic Treatment | Week 2 | Week 4 | Week 6 | Week 8 |
|---|---|---|---|---|---|---|---|
| Informed Consent | x | ||||||
| Clinical evaluation | x | x | x | x | x | x | X |
|
| |||||||
| Serum creatinine | x | ||||||
| ALT, total Bilirubin**** | x
| ||||||
| PK blood draw* | x | x
| x
| ||||
| Sputum cultures | x | x
| x
| x
| x
|
| Drug | Administration | Time of blood draw |
|---|---|---|
| Amoxycillin (+/- clavulanic acid) | Oral | Pre-dose, 6 hours post dose |
| Azithromycin | Oral | Pre-dose (trough), |
| Ciprofloxacin | Oral | Pre-dose (trough), |
| Weight band | Normal drug levels | Sub-target INH <3mg/dl Normal RIF | Normal INH Sub-target RIF <8mg/dl | Sub-target INH <3mg/dl and Sub-target RIF <8mg/dl |
|---|---|---|---|---|
| <55kg | Continue INH 225 mg and RIF 450 mg (3 FDCs) | Give an additional INH tablet equivalent to: INH 300 mg | Give an additional rifampicin tablet equivalent to 600 mg dose | Give additional rifampicin and isoniazid tablets or FDCs equivalent to 300 mg INH and 600 mg rifampicin |
| 55–69kg | Continue INH 300 mg and RIF 600 mg (4 FDCs) | Give an additional INH tablet equivalent to INH 375 mg dose | Give an equivalent rifampicin tablet equivalent to 750 mg dose | Give additional rifampicin and isoniazid tablets or FDCs equivalent to 375 mg INH and 750 mg rifampicin |
| ≥70kg | Continue INH 375 mg and RIF 750 mg (5 FDCs) | Give an additional INH tablet equivalent to 450 mg dose | Give an additional rifampicin tablet equivalent to 900 mg dose | Give additional rifampicin and isoniazid tablets or FDCs equivalent to 450 mg INH and 900 mg rifampicin |
- —Wellcome Trust
- —Wellcome Trust
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotics Pharmacokinetics and Efficacy · Antibiotic Use and Resistance · Antibiotic Resistance in Bacteria
Introduction
Antimicrobial resistance is on the rise, and it is predicted that by 2050 it will be the leading cause of death after cancer, with Africa having the highest burden ^ 1 ^. This will have huge social and economic consequences. In 2019 there were an estimated 1·27 million deaths due to antimicrobial-resistant infections with the highest burden in Africa with most of these infections being bacterial ^ 1 ^.
Optimal dosing to achieve target drug concentrations of anti-infective drugs for each patient is critical for treatment success. Suboptimal concentrations can lead to the emergence of antimicrobial resistance (AMR), clinical treatment failure, and mortality, while high drug exposures may increase the risk of toxicities, which can result in non-adherence or premature cessation of therapy ^ 2 ^. Defining pharmacokinetic- pharmacodynamic relationships in order to predict clinical cure is of critical importance to optimizing antimicrobial therapeutic dosing ^ 3 ^. There are inadequate models to characterize drug-drug interactions (DDI), co-manage multi-morbid health conditions, and inform dose adjustments when physiological states are altered e.g. during infection or inflammation, and obesity ^ 4 ^. This gap is more pronounced in sub-Saharan Africa. The situation is further complicated when more than one of the above scenarios co-exist in specific subsets of patient populations. People living with HIV (PLWH) are at increased risk of AMR across a range of pathogens and across multiple drug classes ^ 5 ^. Notably, PLWH have increased variability in drug exposure because of multimorbid states, increased rates of drug-drug interactions due to polypharmacy and altered physiological functions and associated adverse events. Many of the antiretroviral drugs are known potent inhibitors and inducers of CYP450 enzymes and these antimicrobials are also substrates. Previous work conducted in the SOUTH study where drug concentrations were measured in Uganda PLWH on TB treatment, demonstrated that patients with TB and HIV co-infection have sub-therapeutic plasma concentrations of rifampicin and isoniazid, and this was associated with delayed sputum conversion from positive to negative ^ 6 ^. This has also been demonstrated to be associated with TB relapse in other studies ^ 7 ^. There are several on-going studies that are evaluating higher doses of anti-TB drugs to optimize treatment outcomes and decrease chances of acquiring drug-resistant TB ^ 8– 10 ^
Limited antibiotic options available in these settings need to be optimized to ensure the best dose is available for patients with multimorbidity. While multiple strategies can be used to prevent AMR, including regimen intensification, selection of individualized drug combinations, appropriate sequencing, appropriate duration, and precision dosing, there is limited understanding on which model will be suitable for wider rollout in low-middle income countries (LMICs) as the burden of AMR increases. Therapeutic drug monitoring involves measuring drug concentrations and is useful for drugs that have a narrow therapeutic window, or where sub-optimal drug concentrations are expected. TDM may or may not be followed by dose adjustment. TDM has been widely used in the routine clinical setting for aminoglycosides including gentamicin and vancomycin, and for anti-tuberculosis drugs used in special populations like PLWH and those with diabetes mellitus. Despite the great need of TDM for monitoring antibacterial use in PLWH especially those with TB, there are hardly any studies that have tested its applicability in ensuring appropriate pharmacokinetic and pharmacodynamic outcomes in PLWH in resource constrained settings.
Protocol
Study objectives
- To determine the concentrations of selected antimicrobial agents in people living with HIV requiring antimicrobial therapy.2. To assess the utility of therapeutic drug monitoring in achieving therapeutic targets for people living with HIV receiving rifampicin and isoniazid for treatment of tuberculosis.3. To develop and validate a population pharmacokinetic-pharmacodynamic model for use during therapeutic drug monitoring for selected antibiotics used among PLWH
Study outcomes
** On antibiotics **
Primary endpoints
Pharmacokinetic parameters
- Trough concentrations (Ctrough) for amoxicillin, ciprofloxacin, azithromycin and ceftriaxone
Pharmacodynamic parameters
Clinical response to antibiotics through the time of treatment will be assessed. Clinical response is either clinical cure (resolution of symptoms) or clinical failure (lack of improvement in signs and symptoms of infection OR recurrence of signs/symptoms of infection after initial improvement.
** On TB treatment **
Pharmacokinetic parameters
- Maximum concentrations (Cmax) and area under the concentration-time curve (AUC) defined as the total exposure for rifampicin, isoniazid
Pharmacodynamic parameters
- Clinical response will be assessed according to the World Health Organization definitions of cure, completed and treatment failure, which will be extracted from the clinic database.- Occurrence of adverse drug reactions
Methods
Study site
The study will be conducted at the Infectious Diseases Institute (IDI) which is an out-patient clinic in Kampala, Uganda, where around 8000 PLWH are currently being provided with care, of whom 250 are initiated on TB treatment annually. Participants who are on intravenous medication will be enrolled at Mulago National Referral Hospital which handles both medical and surgical in-patients.
Study participants
Participants will be included if they fulfil the following criteria:
** Inclusion criteria **
-
A personally signed and dated informed consent document
-
An adult of 18 years and above living with HIV
-
Patients being initiated on or currently receiving antibiotics which may include: amoxicillin (+/- clavulanic acid), azithromycin, ciprofloxacin, rifampicin, isoniazid, ceftriaxone
-
Participants who are willing and able to comply with scheduled visits, treatment plan, laboratory tests, and other study procedures.
** Exclusion criteria **
-
Patients who discontinue antibiotics for any reason following initiation
-
Patients receiving antibiotics only for prophylaxis
Sample size
We conducted a priori stochastic simulation and estimation to determine the appropriate sample size for our study. Assuming a 30% coefficient of variation (%CV) in drug exposure, we estimated that enrolling 40 participants per antibiotic would provide sufficient power to detect a 30% effect of HIV co-treatment on antibiotic exposure. In alignment with the ICH E9 guidelines on statistical principles for clinical trials and considering an anticipated 10–15% attrition rate due to study withdrawal and loss to follow-up, we increased the sample size by 10 participants per antibiotic. This adjustment results in a total of 50 participants per antibiotic, or 150 participants overall.
For intravenous antibiotics (ceftriaxone) and anti-TB drugs (rifampicin and isoniazid), we assumed a lower %CV of 25% in drug exposure. Based on this assumption and accounting for an anticipated 15% withdrawal rate, we estimate that a sample size of 25 participants will be sufficient to maintain the power needed to detect possible significant changes in drug exposure due to concomitant antiretroviral therapy.
Study design
Participants on antimicrobial drugs
This will be a prospective observational study that will include adult patients with suspected or confirmed bacterial infection receiving amoxicillin (+/- clavulanic acid), azithromycin, ciprofloxacin. We will enroll 50 participants on each of the oral antimicrobials (amoxicillin, azithromycin, ciprofloxacin). Patients being initiated on antimicrobial agents will be randomly selected, screened, and enrolled. Prescription of antibiotics will be determined by the managing clinician according to standard clinic guidelines. Participants will be requested to take the antibiotic therapy at the same time daily. At baseline, data will be collected on age, sex, gastrointestinal disorders (e.g., diarrhea and vomiting), weight, height, alcohol use, illicit drug use, and details of concomitant medications, including antiretroviral regimens. A blood sample will be drawn for measurement of serum creatinine at baseline. Table 1 demonstrates all study procedures.
** Participant follow-up **
Study visits will be conducted at enrolment, on day 2 for measurement of drug concentrations and the last day of antibiotic use to determine treatment outcome (after 5 – 7 days).
** Sparse pharmacokinetic sampling for antimicrobial drugs **
Sampling for measurement of antibiotic concentrations will be performed on day 2 of antimicrobial therapy. Directly observed therapy will be performed on the day of the blood draw. For those on oral azithromycin and ciprofloxacin, a pre-dose sample (trough concentrations) will be drawn, while for those on amoxicillin, a pre-dose and 6-hour blood draw will be taken. ( Table 2)
** Intense pharmacokinetic sampling for antimicrobial drugs **
Intensive pharmacokinetic sampling will be conducted after at least 2 days of oral antibiotic use, for 20 randomly selected participants on each of these oral drugs; amoxicillin, ciprofloxacin, and azithromycin. At least 20 participants were chosen based on the target of having less than 20% relative standard error in the estimated coefficient of variation. For amoxicillin, blood will be drawn pre-dose, 0.5 h, 1 h, 1.5 h, 2h, 2.5 h, 3 h, 4h, 6h, and 8 h post-dose. For azithromycin and ciprofloxacin, blood will be pre-dose, and at 1 h, 2 h, 3h, 4h, 5h, 6h, 8h, 12h, and 24h post-dose dosing.
Patients on intravenous antibiotics (Ceftriaxone)
Patients who are acutely ill and admitted in the in-patient wards of Mulago hospital will be enrolled for pharmacokinetic sampling while on ceftriaxone. Blood draws will occur when a patient has received at least 1 dose. A blood draw will be taken prior to dosing (Ctrough) and again, 2 hours after completion of bolus administration for ceftriaxone. Participant will be followed up to determine treatment outcome at the end of treatment or at discharge.
Participants on anti-tuberculosis treatment
The current tuberculosis (TB) treatment involves fixed dose combinations based on weight bands, including an intensive phase of rifampicin, isoniazid, ethambutol, and pyrazinamide (RHEZ) for 2 months, followed by a continuation phase of isoniazid and rifampicin (HR) for 4 months. Dosing is determined by weight bands, with 3, 4, or 5 tablets of RHZE or HR depending on weight (<55, 55–69, ≥70 respectively). Each tablet contains 150 mg of rifampicin and 75 mg of isoniazid for both combinations. Fixed dose combinations in the intensive phase include concomitant pyrazinamide and ethambutol.
Serum rifampicin and isoniazid concentrations (C2hr) will be measured in participants when fasting, and following directly observed therapy, after two weeks of treatment (First TDM). Results of blood concentrations will be received within 24–48 hours and assessed to determine if the C2hr (proxy of the Cmax) is within the therapeutic targets. Sub-therapeutic targets are considered <8mg/dl for rifampicin and less than 3mg/dl for isoniazid). Participants found to have a C2hr less than the therapeutic target will have dose escalation and be asked to take one additional pill of the drug that did not achieve therapeutic target concentrations (rifampicin, isoniazid or both) ( Table 3). A second blood draw for measurement of drug concentrations will be performed after another two weeks (Second TDM) and dose adjustment performed again based on the guidance in Table 3, if concentrations are still below the target. ( Figure 1)
Therapeutic drug monitoring procedure with dose adjustment for participants on TB drugs.
If the participant is still not achieving the therapeutic target concentrations after the second C2hr, a 1hr and 6hr blood draw will be conducted to assess for the presence of fast or delayed absorption. An additional dose adjustment with 1 additional tablet of the respective drug may be prescribed for these patients at the discretion of the study team and with consideration of observed side effects, treatment response, and concentrations attained. Those who attain therapeutic drug concentrations during TDM will revert to the previous dose. The final doses provided will be recorded for all participants.
** Sputum analysis **
For participants with tuberculosis, sputum cultures will be conducted at the Makerere University Microbacteriology laboratory. Cultures using Mycobacterium Growth Indicator tube (MGIT) and Lowenstein-Jensen (LJ) agar will be conducted within 7 days of enrolment and will be conducted every two weeks for the first eight weeks of TB treatment (intensive phase).
Laboratory measurement of drug concentrations and sample handling
After blood sample collection, blood samples will immediately be placed in a dark cooler box and transported to the laboratory within 30 minutes of collection, after which samples will be centrifuged, aliquoted, batched, and frozen at -80ªC until quantification of drug concentrations is done. Quantification of the drug concentrations will be performed using pre-established validated liquid chromatography mass spectrometry (LC-MS) methods and high-performance liquid chromatography with ultraviolet detection (HPLC-UV).
Safety assessment
A creatinine level will be measured in patients who undergo intensive pharmacokinetic blood draws, acutely ill in-patients and out-patients without a recent measurement. All other safety testing will be performed according to standard of care. Participants who are found to be pregnant during follow-up will not be excluded. * ** ** *
Adverse event (AE) assessment and reporting will be conducted for participants undergoing dose adjustments for tuberculosis treatment. All observed or volunteered AEs, regardless of suspected causal relationship, will be reported. Adequate information will be obtained to evaluate the causality and severity of the AE using the Naranjo score and Division of AIDS (DAIDS) table respectively. Following adverse events, follow-up will be conducted until the event or its sequelae resolve or stabilize. Participants who suffer harm will be managed by the study which has provided trial insurance for those receiving dose adjustment.
Statistical analysis
** Analysis of data on antimicrobial drugs: sparse pharmacokinetic data **
Sparse pharmacokinetic data for antimicrobials will be analysed as medians with standard deviations. We assess for the effect of covariates like age, sex, body-mass index, CD4 cell counts on drug concentrations
** Analysis of data on antimicrobial drugs: intensive pharmacokinetic data **
Non-linear mixed-effects models will be used to calculate the pharmacokinetic parameters of the drugs and this will include the maximum plasma concentration (Cmax), time to maximum plasma concentration (Tmax), and area under the plasma concentration-time curve (AUC). We will also explore the effects of covariates like age, sex, concomitant medications, and body-mass index on the pharmacokinetic parameters.
** Pharmacodynamic parameters **
We will use pharmacokinetic and pharmacodynamic models to assess the effect of the pharmacokinetic parameters on clinical response. For sparse pharmacokinetic data, we will use drug concentrations as a covariate in the linear regression models predicting clinical response. Clinical response will be defined as either clinical cure (resolution of symptoms) or clinical failure (lack of improvement in signs and symptoms of infection or recurrence of signs/symptoms of infection after initial improvement or death considered at least possibly due to the infection.
** Analysis of data on anti-tuberculosis drugs **
For participants on anti-tuberculosis drugs, we will evaluate whether dose adjustment leads to the achievement of therapeutic targets.
As an exploratory objective, using Kaplan Meier survival analysis, time to sputum culture negativity will be compared for those who received dose adjustment and those who did not receive dose adjustment within this study. We will also utilize the SOUTH dataset where drug concentrations of rifampicin and isoniazid were measured (without dose adjustment), where 78% and 84% of participants had rifampicin and isoniazid concentrations below the therapeutic targets respectively.
Data Monitoring Committee
A Data Monitoring Board (DMB) will be established to evaluate data for participants undergoing TDM with dose adjustment. The board, consisting of an independent chair and members with expertise in clinical trials, will be responsible for safeguarding participant safety and ensuring study integrity. Periodic data reviews will be conducted by the DMB to monitor toxicities, and any concerns identified will be communicated to the study team. The following events, among others, may prompt a request to analyze available safety data for participants receiving dose adjustment and to generate a recommendation on termination of TDM; 1) three participants receiving dose adjustment experience a grade 4 or 5 adverse event in the same system organ class or considered similar (excluding non-clinically significant laboratory abnormalities) that is assessed as probably related or as related to the experimental treatment and 2) one subject receiving dose adjustment experiences a Grade 5 adverse event that is assessed as related to the experimental treatment.
Dissemination of results
These results will be presented to both local and international stakeholders through meetings and international conferences. The raw dataset can be made available to other researchers upon request and signing data sharing agreements, after final results have been published.
Confidentiality
Clinical data will be entered into the study specific dataset by designated staff on a regular basis. Case Record Forms and other source documents will be kept in locked cabinets. No participant identifying information will be disclosed in any publication or at any conference activities arising from the study.
Discussion
Obtaining optimal drug concentrations is vital in treatment success whereas sub-optimal drug concentrations can lead to consequences such as AMR, treatment failure, and adverse outcomes.
This study will increase our understanding of the concentrations of commonly used antibiotics including amoxicillin, azithromycin, ciprofloxacin, ceftriaxone in PLWH, who are at high risk of recurrent infections such as urinary and respiratory tract infections. Understanding the pharmacokinetics and pharmacodynamics of these drugs will increase our understanding of the rising burden of AMR in PLWH, and possibly pave way for interventions that directly impact drug administration.
Therapeutic drug monitoring is increasingly being used for antibiotic dose optimization in the attempt to improve the attainment of pharmacokinetic and pharmacodynamics targets and outcomes of severe infections including in critically ill patients. Although there is a great need of TDM for monitoring selected antibacterial use, there is limited data on its applicability in ensuring appropriate pharmacokinetic and pharmacodynamics outcomes in resource-limited settings. Data from this study will contribute to informing clinicians and researchers about the practicability of using TDM in real-life settings for monitoring the achievement of target concentrations, and the utility of dose adjustment following TDM in different sub-groups of patients such as those with TB and patients with HIV on ART.
This study has some limitations. We cannot ascertain adherence to all treatment provided since directly observed therapy is not conducted throughout treatment, however, we will conduct directly observed therapy on the days when blood samples are drawn for measurement of drug concentrations. In addition, there are several factors that affect pharmacokinetics that we may not be able to assess during this study, for example pharmacokinetics during pregnancy, drug interactions with unknown medications provided over the counter, and comorbidities that occur less frequently and may lead to physiological changes.
In conclusion, the findings from this study will provide information on drug concentrations of frequently used antimicrobial agents in PLWH and guide clinical practices for optimizing doses of rifampicin and isoniazid in order to work towards appropriate dosing and improved treatment outcomes among PLWH.
Ethics and consent
This study has been approved by the Infectious Diseases Institute Research and Ethics Committee (IDI REC) (IDI-REC-2023-83) on 26th February, 2024 and approvals for these changes will be sought prior to implementation. Written informed consent will be obtained by the study team before any study-related activities are conducted. The study will adhere to the Declaration of Helsink. This publication adhered to the SPIRIT guidelines for reporting study protocols.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Antimicrobial Resistance Collaborators: Global burden of bacterial Antimicrobial Resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. 10.1016/S 0140-6736(21)02724-0 35065702 PMC 8841637 · doi ↗ · pubmed ↗
- 2Märtson AG Sturkenboom MGG Stojanova J : How to design a study to evaluate Therapeutic Drug Monitoring in infectious diseases? Clin Microbiol Infect. 2020;26(8):1008–1016. 10.1016/j.cmi.2020.03.008 32205294 · doi ↗ · pubmed ↗
- 3Póvoa P Moniz P Pereira JG : Optimizing antimicrobial drug dosing in critically ill patients. Microorganisms. 2021;9(7):1401. 10.3390/microorganisms 9071401 34203510 PMC 8305961 · doi ↗ · pubmed ↗
- 4Walson PD : Therapeutic Drug Monitoring in special populations. Clin Chem. 1998;44(2):415–419. 9474053 · pubmed ↗
- 5Olaru ID Tacconelli E Yeung S : The association between Antimicrobial Resistance and HIV infection: a systematic review and meta-analysis. Clin Microbiol Infect. 2021;27(6):846–853. 10.1016/j.cmi.2021.03.026 33813126 · doi ↗ · pubmed ↗
- 6Sekaggya-Wiltshire C von Braun A Lamorde M : Delayed sputum culture conversion in tuberculosis–human immunodeficiency virus–coinfected patients with low isoniazid and rifampicin concentrations. Clin Infect Dis. 2018;67(5):708–716. 10.1093/cid/ciy 179 29514175 PMC 6094003 · doi ↗ · pubmed ↗
- 7Pasipanodya JG Mc Illeron H Burger A : Serum drug concentrations predictive of pulmonary tuberculosis outcomes. J Infect Dis. 2013;208(9):1464–1473. 10.1093/infdis/jit 352 23901086 PMC 3789573 · doi ↗ · pubmed ↗
- 8Boeree MJ Heinrich N Aarnoutse R : High-dose rifampicin, moxifloxacin, and SQ 109 for treating tuberculosis: a multi-arm, multi-stage randomised controlled trial. Lancet Infect Dis. 2017;17(1):39–49. 10.1016/S 1473-3099(16)30274-2 28100438 PMC 5159618 · doi ↗ · pubmed ↗