Prophylactic Interventions for Heel Pressure Ulcers in Critically Ill Patients Admitted to an Intensive Care Unit: A Systematic Review and Meta-Analysis
Mayumi Koyanagi, Hideaki Sakuramoto, Kohei Kajiwara, Ayako Fukushima, Shun Yoshihara, Megumi Mukoyama, Megumi Horinouchi, Aiko Mihara, Yuta Imamura

TL;DR
This study reviews and combines evidence from multiple trials to assess the effectiveness of interventions in preventing heel pressure ulcers in critically ill ICU patients.
Contribution
The study provides a comprehensive meta-analysis of interventions for heel pressure ulcer prevention in ICU patients.
Findings
Preventive interventions significantly reduced heel pressure ulcers compared to usual care.
Dressings and heel protectors were effective, but oil application was not significantly effective.
More studies are needed to confirm the effectiveness of oil application.
Abstract
Pressure ulcers are one of the most predictable adverse events, and nurses play a major role in their prevention. Patients receiving intensive care are at a particularly high risk of developing pressure ulcers. The heel is a common area for pressure ulcers, but the number of comparative studies on preventing pressure ulcers is small. Therefore, it is important to combine the evidence. This study aimed to investigate the effectiveness of interventions to prevent heel pressure ulcers by comprehensively extracting and quantitatively integrating the results of studies on preventive care for heel pressure ulcers in critically ill patients. Systematic reviews and meta-analyses were performed. This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA) 2020. Eligible criteria were randomized controlled…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
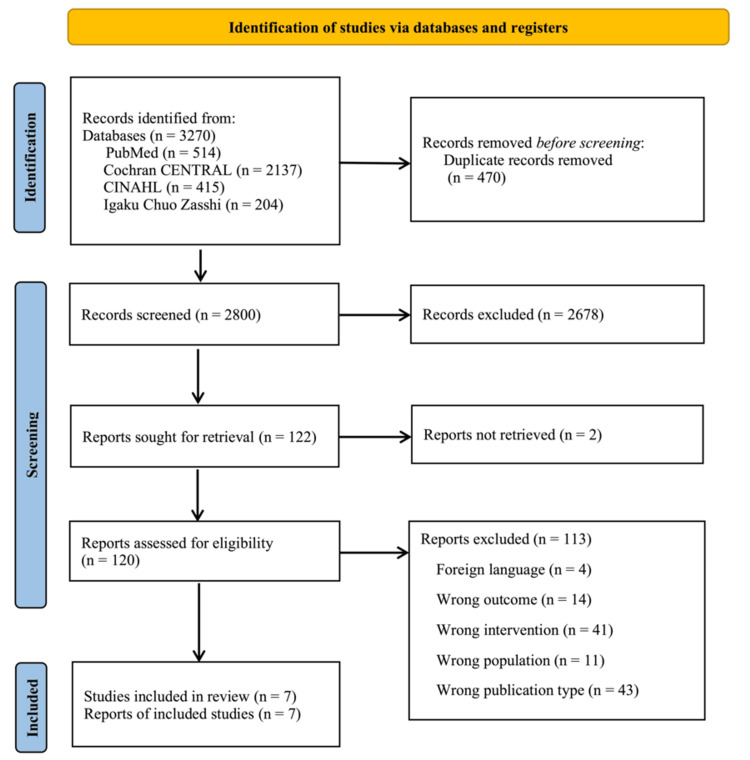 Figure 1
Figure 1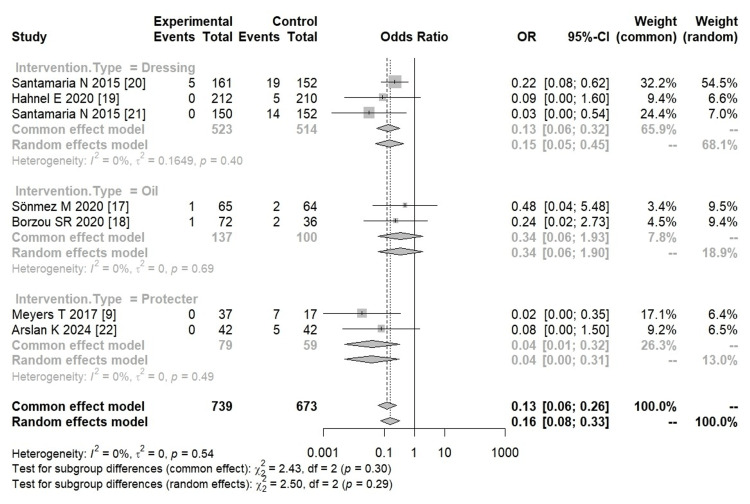 Figure 2
Figure 2| Author (year/country) | Study design | Clinical department/disease | Age, mean (SD) | MV, n (%) | ICU days | Intervention | Control | Measurement | ||
| n | Method | n | Method | |||||||
| Sönmez and Yapucu Güneş [ | RCT | Anesthesia and Neurosurgery ICU | Intervention: 61.4 (17.4); Control: 58.5 (19.2) | Intervention: 14 (25.1); Control: 20 (31.2) | 5 days ≤ | 65 | EVOO was applied to heels (0.5 mL) twice daily for 5 days to 4 weeks, or until a pressure injury developed, ICU stay | 64 | No moisturizing products were used | NPUAP-EPUAP |
| Borzou et al. [ | RCT | Trauma patients, mainly undergoing major surgery | Intervention: 52.7 (19.5); Control: 53.1 (20.0) | NA | NA | 72 | Sweet almond oil or paraffin was applied to pressure-prone heels (1 mL per heel) daily for 7 days | 36 | Standard care | NPUAP-EPUAP |
| Hahnel et al. [ | RCT | ICU in seven departments, including surgery and cardiology | Intervention: 63.8 (15.6); Control: 63.1 (15.2) | Intervention: 199 (93.9); Control: 200 (95.2) | NA | 212 | Mepilex Border Heel dressings were applied to the heels and renewed every 3 days | 210 | Standard care | NPUAP-EPUAP |
| Meyers [ | RCT | SICU, NTICU, MICU | Intervention: 44.6 (17.1); Control: 40.7 (14.9) | NA | NA | 37 | The heel protectors | 17 | Standard care | Via a non-validated heel skin assessment tool |
| Santamaria et al. [ | RCT | Trauma and critically ill patients | Intervention: 54 (20.8); Control: 56 (20.5) | Intervention: 155; Control: 153 | Mean (SD) Intervention: 91 (112); Control: 86 (101) | 161 | Mepilex® Heel dressings were applied to heels with Tubifast® bandages and renewed every 3 days | 152 | Standard care | AWMA |
| Santamaria et al. [ | Prospective cohort study | All major trauma and critically ill patients | Intervention: 55 (19.7); Control: 56 (20.5) | Intervention: 127 (23); Control: 153 (29) | Mean (SD) Intervention: 107 (123); Control: 86 (101) | 150 | Foam heel dressings were applied to both heels and renewed every 3 days | 152 | Standard care | AWMA |
| Arslan and Ates [ | RCT | General and Adult ICUs | Intervention: 72.4 (13.9); Control: 74.5 (13.3) | NA | 5 days ≤ | 42 | Heel protector boots | 42 | Standard care | NPUAP-EPUAP |
| Randomized controlled trials | Methodological quality criteria | Risk score (%) | |||||
| 2.1 | 2.2 | 2.3 | 2.4 | 2.5 | |||
| Santamaria et al. [ | 2015 | Y | Y | Y | C | Y | 20 |
| Meyers [ | 2017 | Y | Y | Y | N | Y | 20 |
| Hahnel et al. [ | 2020 | Y | Y | Y | Y | Y | 0 |
| Sönmez and Yapucu Güneş [ | 2020 | Y | Y | Y | N | Y | 20 |
| Borzou et al. [ | 2020 | Y | Y | Y | C | Y | 20 |
| Arslan and Ates [ | 2024 | Y | Y | Y | C | Y | 20 |
| Non-randomized controlled trials | 3.1 | 3.2 | 3.3 | 3.4 | 3.5 | ||
| Santamaria et al. [ | 2015 | Y | Y | Y | Y | Y | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPressure Ulcer Prevention and Management · Diabetic Foot Ulcer Assessment and Management · Wound Healing and Treatments
Introduction and background
According to the international guidelines, pressure ulcers are defined as localized damage to the skin and/or underlying tissue resulting from pressure, or pressure in combination with shear [1]. That is, it is the result of tissue damage due to inadequate tissue perfusion and is considered one of the preventable adverse events. One in 10 adult patients admitted to the hospital is affected by pressure ulcers, suggesting that the burden of pressure ulcers is large [2].
Patients in intensive care, in particular, are often forced to rest due to their reduced level of consciousness, as well as unstable circulatory dynamics and respiratory status caused by shock and severe circulatory failure. In addition, medical equipment such as ventilators, percutaneous cardiopulmonary support (PCPS), and aortic balloon pumping is often inserted, which restricts body movement. They may also be immobile due to the use of sedatives, often undernourished due to fasting or inability to eat, and have significant edema - making them especially vulnerable to pressure ulcers. Therefore, preventive care is essential [3].
In an international survey of intensive care units (ICUs) conducted in 1,117 facilities across 90 countries, the prevalence of pressure ulcers in ICUs was reported to be 16.2% (95% confidence interval (CI): 15.6%-16.8%) [4]. In addition, the prevalence of pressure ulcers by site was 26.9%-48.0% for the sacrum, 18.5%-38.9% for the heel, 4.1%-46.4% for the buttocks, 10.9%-15.7% for the hip joint, 4.3%-19.7% for the ear, and 0.0%-40.2% for the shoulder [5]. The prevalence of pressure ulcers by site is said to be the second highest in the heel, after the sacrum.
The lower extremities are the furthest from the heart and are susceptible to circulatory failure, such as shock and low blood pressure. The heel has a unique structure, with little subcutaneous tissue for protection and no muscles or fascia, making it vulnerable to pressure, friction, and shear forces. In addition, ICU patients often experience decreased perception and mobility due to sedation and paralysis, are prone to edema, and are frequently subjected to prolonged pressure in a lying position - making them more susceptible to necrosis due to impaired blood flow and embolism. Based on these findings, the heel is an important site for pressure ulcer prevention, and there may be prevention methods specific to ICUs [6].
In a recent meta-analysis [7] conducted in 2021 regarding the prevention of pressure ulcers in ICUs, the effect of applying a prophylactic dressing on the heel showed a risk ratio of 0.31 (95% CI: 0.12-0.80), based on the results of randomized controlled trials (RCTs) up to 2019. In addition, as a direct method to prevent pressure ulcers on the heel, there are approaches such as applying oil to reduce friction and using heel protectors for preventive care. Previous studies have reported the use of oil as a preventive treatment for pressure ulcers in the heel area, but the subjects were not severely ill, and there were no reports of meta-analyses. Meta-analyses of pressure ulcer prevention interventions, including heel protectors, have been conducted for acute care beds [8], but not for ICU patients. However, in 2017, an RCT [9] on pressure ulcer prevention interventions using heel protectors was conducted, but these RCTs were not included in previous meta-analyses. In summary, while intervention studies on the prevention of heel pressure ulcers using dressings have been conducted - and even a meta-analysis exists - the number of systematic reviews remains insufficient, and the evidence base is not well-established. Furthermore, the efficacy of interventions targeting the heel - such as dressings, oil applications, and protectors - remains unclear, despite the high risk of pressure ulcers in ICU patients. To prevent heel pressure ulcers in critically ill patients, improving the quality of care requires a comprehensive review and analysis of prior studies to identify effective interventions.
The aim of the study was to investigate the effectiveness of interventions to prevent heel pressure ulcers by comprehensively extracting the results of research on preventive care for heel pressure ulcers in critically ill patients, and quantitatively integrating them.
Review
Materials and methods
Study Design and Protocol Registration
This was a systematic review and meta-analysis. It was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement (Appendix Table 3) [10]. The study was registered with the Open Science Framework (https://osf.io/r87gc/).
Research Questions
The research questions were set in line with the Population, Intervention, Comparison, and Outcome (PICO) framework. The population was defined as adults aged ≥18 years who were critically ill in all departments, including surgery, internal medicine, and emergency departments. The interventions included receiving direct preventive care for the heel, such as wearing a heel protector, in addition to routine care. The control group included patients who received routine care, such as regular body repositioning, pressure ulcer risk assessment, nutritional support, and bed mattress selection. The incidence of calcaneal pressure ulcers was the primary outcome of this meta-analysis.
Search Strategy
The databases extracted articles from PubMed, the Cochrane Central Register of Controlled Trials, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), and the Central Journal of Medicine, with a limited focus on Japanese and English papers published up to July 2024. Controlled vocabulary was created by converting terms into appropriate equivalents for each database, based on basic conditions (study location, study design, and intervention method). The following search terms were used: intensive care unit, pressure ulcer, prevention, randomized, and non-RCT. Further details are provided in Appendix Table 4.
Eligibility Criteria
In this study, differences and details related to the study area, environment, and variations in beds and mattresses were not included in the endpoints. We included literature that measured the incidence of new pressure ulcers by providing direct intervention to the heel in addition to routine care, compared with the provision of routine care alone. The eligibility criteria were as follows, in accordance with the PICO framework set as a basic condition: (1) the target population is adults hospitalized in the ICU and critically ill, regardless of condition, disease, or prognosis; (2) the intervention is direct preventive care for heel pressure ulcers; (3) the research setting is the ICU; (4) the study design may be an RCT, non-RCT, before-after comparative trial, or intervention study. The exclusion criteria were as follows: (1) studies written in languages other than Japanese or English; (2) literature without a control group.
Outcomes
Our primary outcome was the incidence of heel pressure ulcers in hospitals. As an intervention, we included literature from intervention studies that provided pressure ulcer prevention care directly to the heel in addition to usual care, which was considered an important outcome for critically ill patients in this study. In addition to the inclusion and exclusion criteria, we extracted data from the literature based on the criteria for pressure ulcers. In this study, the severity of pressure ulcers was not assessed, and outcomes were judged solely by whether pressure ulcers occurred.
Study Screening and Data Extraction
The article identified by the search was imported into Rayyan.ai software (Qatar Computing Research Institute, Ar-Rayyan, Qatar; http://rayyan.qcri.org/). As a primary screening, two reviewers screened the article individually to confirm that the basic conditions were met, based on the title and abstract of the article, and the evaluations of the two researchers were collated. In the event of a conflict between the two evaluations, a third reviewer decided whether to accept the proposal. In addition, if a clear judgment could not be made, the article was adopted. In the secondary screening, the full text of the article was obtained, and two reviewers screened the study individually to ensure that the study design, target audience, and intervention met the basic criteria. If the eligibility criteria were met, the study was accepted. In the event of a conflict between the two evaluations, a third reviewer decided whether or not to accept the proposal.
Articles accepted by secondary screening were independently extracted by two review authors based on the following: year of publication, country, ICU type, participant age, duration of ventilator use, ICU admission time, intervention method, and the presence or absence of heel pressure ulcer formation.
Assessment of the Risk of Bias
The studies included not only RCTs but also non-RCTs. Therefore, the evaluation was conducted using the Mixed Methods Appraisal Tool (MMAT), version 2018 [11,12]. There were two common items: (1) Do you have a clear research topic? and (2) Can the collected data address this research problem? RCTs and non-RCTs were evaluated on these two common items using three levels: “Yes,” “No,” and “Can’t tell.” If “No” or “Can’t tell” was selected for either of the two common items, the article was excluded as not being an empirical study. In addition, if both common items were evaluated as “Yes,” the five criteria of each study design were evaluated on the same three terms: “Yes,” “No,” and “Can’t tell.” The five items for RCTs were as follows: (2.1) whether the study participants were adequately randomized, (2.2) whether the intervention and control groups were comparable at the start of the study, (2.3) whether complete outcome data were available, (2.4) whether outcome assessors were blinded to the intervention, and (2.5) whether participants were able to comply with the assigned intervention. The five items for non-RCTs were as follows: (3.1) participants were representative of the target population, (3.2) measured variables were measured in a clear and credible manner, (3.3) complete outcome data were available, (3.4) confounders were taken into account in the design and analysis, and (3.5) whether the intervention was implemented as intended during the study period. The quality of the studies was then critically assessed based on the number of “No” and “Can’t tell” responses to the five items in each study design. We also examined publication bias using funnel plots. However, when the number of articles included in the study was small (fewer than 10), the shape of the plots tended to be unstable. It is also difficult to accurately determine the presence or absence of asymmetry or bias, making visual interpretation challenging. Furthermore, the results tend to depend on specific conditions and contexts, making it difficult to draw broad conclusions and limiting the generalizability of the results [13,14]. Therefore, we decided not to evaluate the risk of bias, as we believe that the potential error in assessing the risk of bias would be greater.
Data Synthesis and Assessment of Heterogeneity
The synthesis and analysis of the data extracted from the article use the method of meta-analysis, and the analysis software, which is the graphical user interface of R (The R Foundation for Statistical Computing, Vienna, Austria), is EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan). EZR is a graphical user interface for R, or more precisely, an improved version of the R Commander, designed to add statistical functions frequently used in biostatistics.
Two variables that are conceptually homogeneous are defined as odds ratios (ORs). Seven articles were adapted for this systematic review, but the details of the methodological differences between the articles were not included in the evaluation. Random Effects Meta-analysis was chosen to allow for differences in research methodology and approach across articles. The study also aimed to identify the effectiveness of interventions to prevent heel pressure ulcers by using statistical methods to investigate the effectiveness of such interventions, comprehensively identifying and quantitatively integrating studies on preventive care for heel pressure ulcers in critically ill patients. ORs were also evaluated to compare the likelihood of developing pressure ulcers between the intervention group, which received the pressure ulcer prevention intervention, and the control group, which did not. A 95% CI was calculated for the reliability of the statistics. The effect size was evaluated based on previous studies [15]. Data were analyzed in subgroups by intervention methods and study design and pooled by forest plots. Variation in conclusions across articles was determined using the heterogeneity I² statistic. According to the Cochrane Handbook [16], “heterogeneity may not be significant” in the case of I² < 40% of cases. Therefore, I² ≧ 40% was judged to be highly heterogeneous. We also conducted a sensitivity analysis of each type of intervention to assess the robustness of the data.
Results
An article search was conducted on July 28, 2024. A total of 514 studies from PubMed, 2,137 from the Cochrane Central Register of Controlled Trials, 415 from CINAHL, and 204 from the Central Journal of Medicine were identified, for a total of 3,270 studies. Of these, 2,800 articles, excluding duplicate studies, were screened.
In the first screening, 2,678 cases were excluded. In the second screening, 122 full-text studies were searched, and eligibility was assessed according to the inclusion and exclusion criteria. Seven of these studies met the eligibility criteria (Figure 1).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagramThe selection of studies on prophylactic interventions for heel pressure ulcers in critically ill patients, admitted to the intensive care unit, is presented.Abbreviation: Cochrane CENTRAL, Cochrane Central Register of Controlled Trials; CINAHL, Cumulative Index to Nursing and Allied Health Literature
Characteristics of the Study
The characteristics of the seven selected studies are summarized in Table 1. The included studies were published between 2013 and 2024 and were conducted in Turkey (two studies), Iran (one study), Germany (one study), the United States (two studies), and Australia (two studies). Six of the seven studies were RCTs, and one was a case-control study. A total of 1,412 patients (739 in the intervention group and 673 in the control group) were included in the study, with a mean age of 40.6-74.52 years. The subjects included three studies on trauma emergency patients and four studies in the general intensive care field, including surgery, internal medicine, and cardiology. Four of the seven studies involved patients on mechanical ventilation or sedation for at least 90%, and five of the seven studies had ICU stays of ≥3-5 days. As an inclusion criterion, four studies used the Braden scale at the time of entry, with one criterion being a Braden scale score of ≤18. There was also one study that looked at sedatives and immobility time as criteria. As exclusion criteria, some literature excluded patients with peripheral vascular disease, unstable peripheral circulatory dynamics, patients receiving vasoconstrictor drugs, and patients who were contraindicated for repositioning for medical reasons. In addition, two studies in trauma emergency patients excluded patients with spinal cord injuries or those with a history of pressure ulcers or trauma in the heel.
In all articles, the control group had regular positional changes, retention, rehabilitation, and choice of bed mats as part of their usual care. In the intervention group, in addition to usual care, two of seven studies [17,18] used oil application, three studies [19,20,21] used heel dressing, and two studies [9,22] used protector intervention.
Risk of Bias in the Included Studies
Both RCTs and non-RCTs were assessed using the MMAT (Table 2). For the two common screening questions, all included studies presented “Yes,” and there was a low risk of bias. All six RCTs were adequately randomized, had a comparable baseline for the intervention and control groups, and had complete outcome data. In all studies, the participants could comply with the interventions. One (16.7%) study had outcome assessors blinded to the details of the intervention, three (50.0%) were unblinded, and two (33.3%) did not clearly describe blinding. In one non-RCT study, the participants were well chosen, the variables were measured reliably, and the outcome data were analyzed appropriately. The intervention was implemented throughout the study period. Confounding factors were also considered in the design and analyses. All studies had a bias score of 0%-20%, which indicated a low risk. We also examined publication bias using funnel plots. However, due to the small number of papers included in this study (no more than 10), the shape of the plots was unstable.
Outcomes
The results of the meta-analysis are shown in Figure 2. In this study, additional pressure ulcer preventive interventions on the heel prevented pressure ulcers compared with usual care alone (OR = 0.16, 95% CI = 0.08-0.33, I² = 0%, large effect size). In addition, heterogeneity was low. Analyses were performed on subgroups for each intervention. There were two RCTs [19,20] and one non-RCT [21] that used dressings. The application of the dressing was effective in preventing pressure ulcers compared with normal care alone (OR = 0.15, 95% CI = 0.05-0.45, I² = 0%, large effect size). In addition, there were two studies in which protectors were worn (OR = 0.04, 95% CI = 0.00-0.31, I² = 0%, very large effect size) [9,22]. However, oil application did not show any effect on preventing pressure ulcers compared with usual care alone (OR = 0.34, 95% CI = 0.06-1.90, I² = 0%) [17,18]. All the intervention methods resulted in low heterogeneity.
Forest plot of the included studiesForest plot of subgroup analysis based on intervention for the prevention of heel ulcers.Abbreviations: OR, odds ratio; CI, confidence interval; χ2, chi-squared test; df, degree of freedom
A sensitivity analysis was performed by study design. Six of the seven studies were RCTs (OR = 0.18, 95% CI = 0.08-0.39, I² = 0%), and one was a non-RCT (OR = 0.03, 95% CI = 0.00-0.54). In the analysis based on design, the results showed that the intervention prevented pressure ulcers. The six RCTs demonstrated low heterogeneity (Appendix Figure 3).
Discussion
Summary of Findings
A systematic review and meta-analysis were conducted to determine the effectiveness of preventive interventions for heel ulcers, and the results were pooled from seven papers, with a total of 1,412 participants. Heel pressure ulcer prevention interventions included three studies using dressings, two using oil applications, and two using protector interventions, and the results showed that these interventions were effective in preventing heel pressure ulcers compared to usual care alone.
Heel pressure ulcers can be easily prevented by simple care, such as wearing a protector and applying a dressing to prevent heel ulcers in severely ill patients. A 2021 meta-analysis of previous studies in patients in acute care hospitals also showed a significant protective effect from wearing protectors, which was consistent (relative risk (RR) = 0.38, p < 0.001) [8]. A meta-analysis of an intervention in which a prophylactic dressing was applied to the heel of critically ill patients found similar results (RR = 0.31, 95% CI = 0.12-0.80, p = 0.02) [7]. On the other hand, in this study, the effect of applying oil to prevent pressure ulcers on the heel was compared for the first time, but the preventive effect of oil was not shown.
Existing Evidence and Gaps
In this study, a subgroup analysis was used to compare protectors and dressings with placebo or normal care alone and found a protective effect. On the other hand, there have been no comparative studies between the types of dressings and protectors, and no studies have been conducted on which types of prevention methods are most effective. Therefore, there is a lack of further comparative studies between interventions that have been found to have such protective effects on the heels of critically ill patients. In addition, pressure ulcer prevention, including for the heels, reduced the mortality of patients with and without pressure ulcers (9.1% vs. 1.8%, OR = 5.08, 95% CI = 5.03-5.1, p < 0.001) and length of hospital stay (median: seven days vs. three days), but also improved patient outcomes, such as reducing healthcare costs (median: 17,200) [23]. A comparative study in Brazil in critically ill patients [24] showed the same results for mortality (48.8% vs. 21.6%, p < 0.001) and length of hospital stay (20.7 ± 15.76 days vs. 9.7 ± 8.07 days, p < 0.001). In addition, compared to the care of pressure ulcer treatment, preventive care can be done with less time and effort and prevents the increase in medical burden and medical costs. However, cost-effectiveness was not included in the evaluation of this study. In a previous study, Lyman [25] found that protector wear is effective in preventing heel pressure ulcers and can significantly offset the cost of treatment, although initial costs are required. Also, according to a study by El Genedy et al. [26], the application of prophylactic dressings in critically ill patients is limited in the heel area due to cost-effectiveness, but dressings should be applied for patients at high risk for pressure ulcers. Both studies indicate that the more severe the pressure ulcer, the more cost-effective it is. Therefore, it is necessary to prevent heel pressure ulcers according to the economic situation and culture of the area. From the above, it follows that in the future, it will be necessary to conduct comparative studies between each intervention method from a broad perspective, including not only preventive effects but also patient outcomes and medical burdens.
There were also different types of interventions in the prevention of oils, protectors, and dressings. In the included studies, all three dressings were silicone dressings, with some having three layers and some having five layers. The oils applied in the intervention included extra virgin olive oil, almond oil, and paraffin oil. A comparative study conducted in Iran in 2019 [27] on the prevention of pressure ulcers by type of oil examined the effects of henna oil and olive oil as treatments for pressure ulcer grade I, but it was not clearly shown whether they were effective in preventing pressure ulcers. There are also other comparative studies in which olive oil and aloe vera gel were applied alone or in combination to critically ill patients, showing efficacy in preventing pressure ulcers (OR = 0.43 in the olive group, 0.86 in the aloe vera group, 0.34 in both groups) [28], but it was not an intervention for the heel. In this way, although there are various studies, which type of oil is better has not been compared, and such comparative studies will be necessary in the future.
Implications for Clinical Practice and Research
In this study, it was clarified that, in addition to usual care for the heel, the intervention of applying a protector or a dressing can help prevent pressure ulcers on the heel. This means that the intervention is suitable for patients with unstable circulatory dynamics or those who are immobile due to sedation or intubation management, and that it is possible to prevent heel ulcers by adding simple interventions to existing care. Research suggests that protective patches and dressings are effective in preventing heel pressure ulcers in critically ill patients, but it is not yet known which interventions are most effective. In addition, there are differences in the types of interventions and the materials used (e.g., the type of protector or dressing), and it remains unclear which option is the simplest and most effective. Therefore, such comparative studies need to be conducted through large-scale RCTs.
Strengths and limitations of research
To the best of our knowledge, this is the first report of any systematic review or meta-analysis of pressure ulcer prevention interventions limited to the heel of critically ill patients. Existing meta-analyses have focused on older adults or the acute phase in general, not specifically on higher-risk ICU patients. In this study, we conducted a meta-analysis that included not only RCTs but also non-RCTs. These are the strengths of this study. However, there are also limitations in some of the included studies. First, the inclusion of non-RCTs may lead to bias. In this study, the MMAT assessment showed low risk in all literature, so the risk of bias is judged to be small, and its effect may be minimal. Second, we analyzed the intervention methods as a subgroup analysis, classifying them into dressings, protectors, and oil applications. However, the number of studies was small - two on oil applications, two on protectors, and three on dressings. Due to the small number of studies, caution should be exercised when interpreting the results of the subgroup analyses, and the number of high-quality intervention studies will need to be increased in the future. Third, we were unable to assess publication bias using a funnel plot. This was due to the small number of included papers, which made it difficult to accurately determine the presence or absence of asymmetry or bias. In addition, the results are easily influenced by specific conditions and circumstances, making it difficult to draw broad conclusions. Therefore, the generalizability of the present results is considered limited.
Conclusions
This meta-analysis demonstrated that additional preventive interventions for heel pressure ulcers in critically ill patients were more effective in preventing the incidence of heel pressure ulcers compared to usual care. The use of dressings and protectors has a preventive effect on heel pressure ulcers. Oil application, however, does not have a preventive effect on pressure ulcers. Additionally, the number of studies is small and insufficient to draw firm conclusions from the subgroup analysis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wound Healing Society 2015 update on guidelines for pressure ulcers Wound Repair Regen Gould L Stuntz M Giovannelli M 1451622420162668352910.1111/wrr.12396 · doi ↗ · pubmed ↗
- 2Global prevalence and incidence of pressure injuries in hospitalised adult patients: a systematic review and meta-analysis Int J Nurs Stud Li Z Lin F Thalib L Chaboyer W 10354610520203211314210.1016/j.ijnurstu.2020.103546 · doi ↗ · pubmed ↗
- 3Risk factors for pressure injuries among critical care patients: a systematic review Int J Nurs Stud Alderden J Rondinelli J Pepper G Cummins M Whitney J 971147120172838453310.1016/j.ijnurstu.2017.03.012PMC 5485873 · doi ↗ · pubmed ↗
- 4Prevalence, associated factors and outcomes of pressure injuries in adult intensive care unit patients: the Decub IC Us study Intensive Care Med Labeau SO Afonso E Benbenishty J 1601694720213303468610.1007/s 00134-020-06234-9PMC 7880913 · doi ↗ · pubmed ↗
- 5Incidence and prevalence of pressure injuries in adult intensive care patients: a systematic review and meta-analysis Crit Care Med Chaboyer WP Thalib L Harbeck EL 08146201810.1097/CCM.000000000000336630095501 · doi ↗ · pubmed ↗
- 6Heel pressure injuries in the adult critical care population Crit Care Nurs Clin North Am Delmore B Ayello EA 5895993220203312941610.1016/j.cnc.2020.08.008 · doi ↗ · pubmed ↗
- 7Effectiveness of interventions to prevent pressure injury in adults admitted to intensive care settings: a systematic review and meta-analysis of randomised controlled trials Aust Crit Care Lovegrove J Fulbrook P Miles S Steele M 1862033520223414486510.1016/j.aucc.2021.04.007 · doi ↗ · pubmed ↗
- 8Effectiveness of interventions to prevent pressure injury in adults admitted to acute hospital settings: a systematic review and meta-analysis of randomised controlled trials Int J Nurs Stud Lovegrove J Fulbrook P Miles SJ Steele M 10402712220213433417510.1016/j.ijnurstu.2021.104027 · doi ↗ · pubmed ↗