Engraftment outcome of patients with anti-HLA antibodies in HLA-mismatched peripheral blood stem cell transplantation
Takeshi Hagino, Kazuhiro Ikegame, Hidenori Tanaka, Yoshinobu Kanda, Katsuji Kaida, Takahiro Fukuda, Yukio Kondo, Maho Sato, Noriko Doki, Hirohisa Nakamae, Ken-ichi Matsuoka, Yasuo Mori, Hideki Sano, Tetsuya Eto, Toshiro Kawakita, Yoshiko Hashii, Tatsuo Ichinohe, Yoshiko Atsuta

TL;DR
This study examines how anti-HLA antibodies affect engraftment outcomes in stem cell transplants using nationwide registry data.
Contribution
The study provides large-scale registry insights into the impact of anti-HLA antibodies on engraftment outcomes.
Findings
Anti-HLA antibody-positive patients had better neutrophil engraftment than antibody-negative patients.
High DSA levels did not necessarily lead to graft failure, as most patients achieved engraftment.
DSA-depleting interventions showed limited data due to the small number of high DSA patients.
Abstract
Anti-human leukocyte antigen (HLA) antibodies, particularly donor-specific HLA antibodies (DSA), negatively impact engraftment in hematopoietic cell transplantation. Past studies have proposed various interventions to reduce DSA, but these were primarily from single centers and not from large-scale registry data. Therefore, we conducted a retrospective analysis of nationwide registry data to examine the effects of anti-HLA antibodies on engraftment. Evaluable patients were classified into an anti-HLA antibody-negative group (n = 3657), an anti-HLA antibody-positive group (without high DSA) (n = 137), and a high-DSA (MFI > 5000) group (n = 8). Patient characteristics differed significantly between the anti-HLA antibody-negative and anti-HLA antibody-positive groups, and the number of patients with DSA was lower than expected. Statistical analyses revealed that the anti-HLA…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
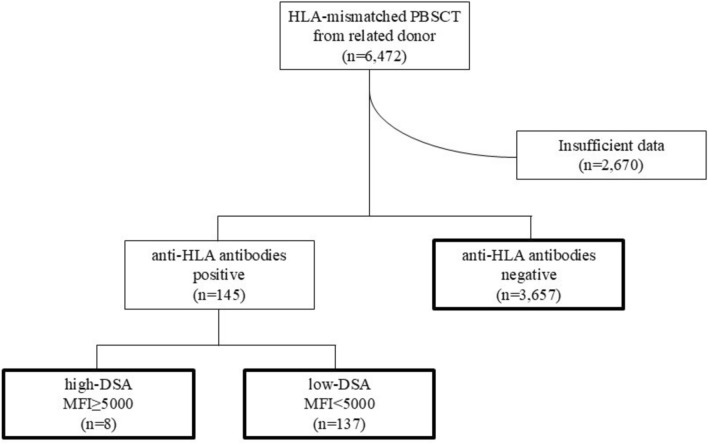 Figure 1
Figure 1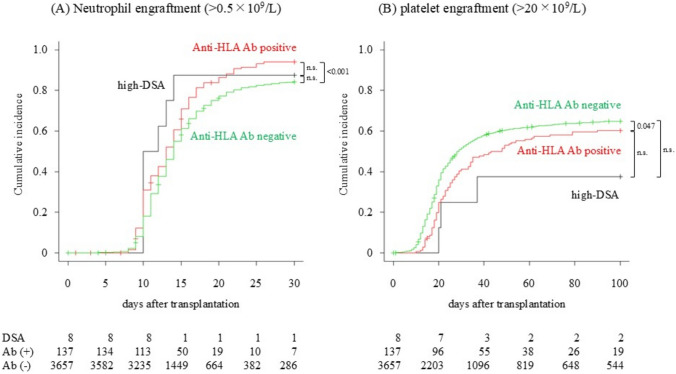 Figure 2
Figure 2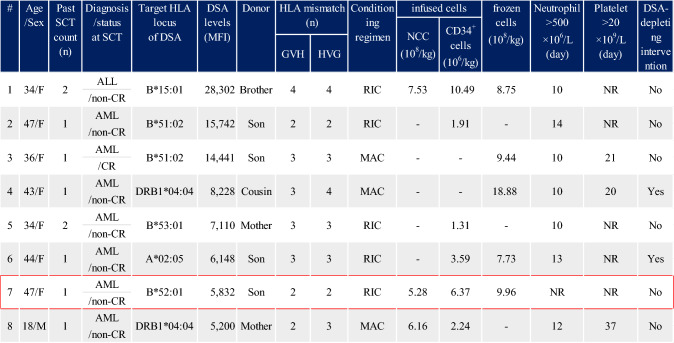 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHematopoietic Stem Cell Transplantation · Renal Transplantation Outcomes and Treatments · Transplantation: Methods and Outcomes
Introduction
As human leukocyte antigens (HLA)-mismatched hematopoietic stem cell transplantation has become more widespread, anti-HLA antibodies in pre-transplant recipients have come into focus. We and others have reported that anti-HLA antibodies, especially donor-specific anti-HLA antibodies (DSA), are a risk factor for graft failure not only in cord blood transplantation [1] but also in HLA-mismatched (haploidentical) stem cell transplantation [2, 3, 4, 5]. Various protocols have been proposed to reduce DSA levels, such as suppression of antibody production using rituximab [6], depletion of DSA through transfusion of targeted HLA-expressing platelets [7], and immunomodulation using high-dose intravenous immunoglobulin therapy [8]. The consensus guidelines from the European Society for Blood and Marrow Transplantation (EBMT) propose that a mean fluorescence intensity (MFI) of 5,000 or higher is the cut-off for high DSA [9]. However, the proposition that anti-HLA antibodies are a risk factor for graft failure has been reported primarily in single centers and has not yet been reported in large registry data. Additionally, none of the DSA-depleting interventions have sufficient evidence and are not covered by medical insurance in Japan. Therefore, we identified patients with anti-HLA antibodies, particularly those with high levels of DSA, in nationwide registry data to elucidate the effect of anti-HLA antibodies on engraftment in practical settings. To exclude the influence of the stem cell source, we focused on peripheral blood stem cell transplantation (PBSCT) in this study.
The effect of anti-HLA antibodies on engraftment is inconclusive based on the current data. However, it might be beneficial to know the existence of some patients who achieved neutrophil engraftment even with high levels of DSA. We also discussed why the MFI value of DSA is sometimes consistent with expectations and sometimes not, based on recent literature.
Materials and methods
Patients
A total of 6,472 patients who had undergone HLA-mismatched PBSCT from a related donor were enrolled in the Japanese Society for Transplantation and Cellular Therapy/The Japanese Data Center for Hematopoietic Cell Transplantation (JSTCT/JDCHCT) Transplant Registry Unified Management Program (TRUMP) during the 5 years from 2010 to 2014. Registration in the TRUMP requires checking one of three boxes: anti-HLA antibody-positive, anti-HLA antibody-negative, and not tested; if positive, checking whether it is DSA. We conducted a secondary survey for each DSA-positive case to determine the MFI of the DSA. According to the EBMT consensus, [9] we defined the cut-off for high DSA as MFI > 5,000. After excluding cases with insufficient data, 145 patients were found to have anti-HLA antibodies before transplantation, and the remaining 3,657 patients were classified into the anti-HLA antibody-negative group. Among the 145 patients with anti-HLA antibodies, only eight patients had high DSA (MFI > 5,000; high-DSA group). We designated the remaining 137 patients as anti-HLA antibody-positive (low DSA of less than MFI 5,000; not a high DSA of MFI > 5,000). No cases with DSA for multiple HLA loci were found. A consort diagram is shown in Fig. 1. We then compared the three groups: the high-DSA group (n = 8), the anti-HLA antibody-positive group (n = 137), and the anti-HLA antibody-negative group (n = 3,657). In this analysis, we evaluated antibodies targeting the HLA-A, B, C, and DRB1 loci based on the available data. Anti-HLA antibodies against HLA-DP, HLA-DQ, and HLA-DRB3/4/5 were not considered anti-HLA antibodies, because the donor data for these HLA loci were unavailable. MFI for each HLA allele was determined using a flow bead-based Luminex assay by the HLA Foundation Laboratory (n = 77), the Japanese Red Cross Society (n = 12), Repro CELL Incorporated (n = 5), cord blood bank (n = 1), the treating institution (n = 48), and unknown (n = 2).Fig. 1. Consort diagram. Consort diagram for grouping of “anti-HLA antibodies negative,” “high DSA,” and “anti-HLA antibody-positive (low DSA)” is shown. HLA, human leukocyte antigen; DSA, donor-specific antibody
Statistics
Neutrophil and platelet engraftments were defined as an absolute neutrophil count of > 0.5 × 10^9^/L on the first of 3 consecutive days and a platelet count of > 20 × 10^9^/L without transfusion. The cumulative incidences of neutrophil and platelet engraftment were estimated by treating death before engraftment as a competing risk and were compared using the Gray test. Yates’ Chi-square test and Student’s t test were used to compare categorical and numerical variables (age and infused CD34^+^ cells), respectively, between the two groups. Given that comparing among all three groups was deemed to lack logical significance, the comparisons were restricted to pairs of groups with a predetermined statistical significance level of p < 0.05, owing to the exploratory nature of the study. Statistical analyses were performed using EZR (Saitama Medical Centre, Jichi Medical University; http://www.jichi.ac.jp/saitama-sct/SaitamaHP.files/statmedEN.html), a graphical user interface for R (version 3.0.2; R Foundation for Statistical Computing, Vienna, Austria) [10]. This study was approved by the Institutional Review Boards of the JSTCT and Tama-Hokubu Medical Center, Tokyo Metropolitan Health and Medical Treatment Corporation.
Results
Patients’ characteristics
The characteristics of the patients in the anti-HLA antibody-negative, anti-HLA antibody-positive, and high-DSA groups are shown in Table 1. Compared with the anti-HLA antibody-negative group, the anti-HLA antibody-positive group was predominantly female, older in age, and had different diseases. Additionally, the anti-HLA antibody-positive group had a predominance of remission state, high Hematopoietic Cell Transplantation-specific Comorbidity Index (HCT-CI) scores, second or further transplantation, ABO mismatch, and HLA mismatches in the Graft versus Host (GVH) and Host versus Graft (HVG) directions, but fewer infused CD34^+^ cells. Furthermore, reduced-intensity conditioning without total body irradiation followed by GVH disease (GVHD) prophylaxis not consisting of mycophenolate mofetil (MMF), methotrexate (MTX), or post-transplant cyclophosphamide (PTCy) but consisting of tacrolimus (TAC) plus corticosteroid was more used in the anti-HLA antibody-positive group than in the anti-HLA antibody-negative group. Anti-thymocyte globulin was used as GVHD prophylaxis 0, 2, and 80 in the high-DSA, 2 anti-HLA antibody-positive (low-DSA), and 80 anti-HLA antibody-negative groups, respectively. We discuss the differences in the background and their effects on the following results.Table 1. Patients’ characteristicsCovariatesAnti-HLA Abnegative(n = 3,657)Anti-HLA Abpositive(n = 137)High-DSA(MFI > 5,000)(n = 8)p value(neg. vs pos.)p value(neg. vs DSA)p value(pos. vs DSA)SexMale2,143581 < 0.0010.0220.193Female1,514797Age (years)Average37.146.937.9 < 0.0010.9120.092(range)(0 – 76)(3 – 68)(18 – 47)PS0–12,4529870.5310.6880.6532–4848391DiseaseMDS/AML1687987 < 0.0010.3260.923ALL722191Other leukemia18950CML/MPD14530Lymphoma60290Miscellaneous28520Disease statusRemission4401027 < 0.0010.0020.783Non-remission942311HCT-CI0–23,166867 < 0.0011.0000.1863–10422641History of previous stem cell transplantation02,2217960.3840.6920.63811,14747222361103–65200Conditioning regimenMAC1,113323 < 0.0011.0000.628RIC16221055TBI (-)1,784927 < 0.0010.0710.417TBI ( +)1,831451Sex combination(Pt ← Donor)match1,8307810.0920.0020.011M ← F971261F ← M748336ABO type combinationMatch1,686785 < 0.0011.0000.677Major-mismatch621332Minor-mismatch57200Major + minor mismatch20181GVHD prophylaxisCyclosporin-based1,142150 < 0.0010.1150.695Tacrolimus-based2,3941228Additional GVHD prophylaxisCorticosteroid (-)2,493750 < 0.001 < 0.0010.008Corticosteroid ( +)1,057628MMF (-)2,9801097 < 0.0011.0000.927MMF ( +)338281MTX (-)1,5001008 < 0.0010.0030.198MTX ( +)2,066370post-CY (-)3,50612580.0051.0000.83post-CY ( +)136120HLA mismatch in GVH vector047590 < 0.0010.1070.7411–22,0205833–1,078705HLA mismatch in HVG vector037230 < 0.0010.0760.4051–22,0036223–1,197726Infused CD34^+^ cells (× 10^6^/kg)Average5.333.974.31 < 0.0010.5150.739(range)(0.01–52.30)(0.74–15.10)(1.31–10.49)HLA, human leukocyte antigen; DSA, donor-specific anti-HLA antibody; MFI, median fluorescence intensity; HCT-CI, Hematopoietic Cell Transplantation-specific Comorbidity Index; PS, performance status; Pt, patient; GVH, in graft-versus-host direction; HVG, in host-versus-graft direction; GVHD, graft-versus-host disease; MDS, Myelodysplastic syndrome; AML, Acute myelogenous leukemia; ALL, Acute lymphoblastic leukemia; CML, Chronic myeloid leukemia; MPD, Myeloproliferative Disease; RIC, Reduced-intensity conditioning; MAC, myeloablative conditioning; TBI, Total body irradiation; M, male; F, female; MMF, mycophenolate mofetil; MTX, methotrexate; Post-CY, post-transplant cyclophosphamideCharacteristics of patients in the anti-HLA antibody-negative, anti-HLA antibody-positive, and high-DSA groups are shown in the three left columns. Background covariates between the anti-HLA antibody-negative and anti-HLA antibody-positive groups, anti-HLA antibody-negative and high-DSA groups, and the anti-HLA antibody-positive and high-DSA groups were compared. The p values of Yates’ Chi-squared test for categorical variables or Student’s t test for age and infused CD34 + cells are shown in the three right columns. Significant differences (p < 0.05) are highlighted in red
Neutrophil and platelet engraftments
The cumulative incidence of neutrophil and platelet engraftment is shown in Fig. 2. The estimates of neutrophil and platelet engraftment rates for the anti-HLA antibody-negative, anti-HLA antibody-positive, and high-DSA groups and the statistical differences are summarized in Table 2. Contrary to previous reports, our data revealed the following: the cumulative incidence of neutrophils on day 30 was higher in the anti-HLA antibody-positive group than in the anti-HLA antibody-negative group (94.0% vs. 84.2%, p < 0.001); the cumulative incidence of platelets on day 100 was higher in the anti-HLA antibody-negative group than in the anti-HLA antibody-positive group (64.9% vs. 60.3%, p = 0.047); and high levels of DSA (MFI > 5,000) did not significantly affect the neutrophil and platelet engraftment outcome compared with the other two groups according to monovariate analyses. The first two results are conflicting and are difficult to interpret or explain; they will be discussed later. The last result is probably because the number of patients in the high-DSA group was too small to provide sufficient statistical power. Therefore, we focused on clarifying the actual outcomes in the DSA-high group.Fig. 2. Neutrophil and platelet engraftments. Cumulative incidences of neutrophil (A) and platelet (B) engraftment are described in three groups: anti-HLA antibody-negative group (n = 3,657, green), anti-HLA antibody-positive group (n = 137, red), and high-DSA group (n = 8, black). Death before engraftment was defined as the competing risk. The at-risk numbers are shown in the figure. HLA: human leukocyte antigen; DSA, donor specific anti-HLA antibody; DSA, high-DSA group; Ab ( +), anti-HLA antibody-positive group; Ab (-), anti-HLA antibody-negative groupTable 2Estimation of neutrophil and platelet engraftmentsEngraftment rateestimatesAnti-HLA Abnegative(n = 3,657)Anti-HLA Abpositive(n = 137)High-DSA(MFI > 5,000)(n = 8)p value(neg. vs pos.)p value(neg. vs DSA)p value(pos. vs DSA)NeutrophilPoint estimate0.8420.9400.875 < 0.001^a^0.1110.65695%CI0.830–0.8530.877–0.9120.174–0.990PlateletPoint estimate0.6490.6030.3750.047^b^0.1320.26795%CI0.633–0.6640.515–0.6800.070–0.697HLA, human leukocyte antigen; DSA, donor specific anti-HLA antibody; SCT, stem cell transplantation; MFI, median fluorescence intensity; GVH, in graft-versus-host direction; HVG, in host-versus-graft direction; NC, Nucleated cells; Plt, platelets; AML, Acute myelogenous leukemia; ALL, Acute lymphoblastic leukemia; non-CR, non-complete remission; F, female; M, malePoint estimates with 95% confidence intervals of neutrophil and platelet engraftment rates in the anti-HLA antibody-negative, anti-HLA antibody-positive, and high-DSA groups are shown in the three left-hand columns. Statistical differences in the Gray test between the anti-HLA antibody-negative and anti-HLA antibody-positive groups, anti-HLA antibody-negative and high-DSA groups, and anti-HLA antibody-positive and high-DSA groups are shown in the three right columns. Significant differences (p < 0.05) are highlighted in red^a^The engraftment rate of neutrophils was higher in the anti-HLA antibody-positive group than in the anti-HLA antibody-negative group^b^The engraftment rate of platelets was higher in the anti-HLA antibody-negative group than in the anti-HLA antibody-positive group
Profile of patients with high-DSA
The profiles of the eight patients in the DSA-high group are presented in Table 3. They were mainly females (7/8), suggesting alloantibody production due to pregnancy. Although only two patients (#4 and #6) received a DSA-depleting intervention, neutrophil engraftment was observed in seven cases. One patient (#7) who had DSA against HLA-B52:01 (MFI 5.832) and was transplanted with a sufficient number of CD34^+^ cells (6.3710^6^/kg) without DSA-depleting intervention developed graft failure. The patient died of sepsis on day 30 without engraftment. All three patients with MFI > 10,000 (#1: MFI, 28,302, #2: 15,742 and #3: 14,441) achieved neutrophil engraftment on days 10, 14, and 10, respectively, without DSA-depleting intervention. Patient 1 died of early recurrence within 28 days. The remaining two patients (2 and 3) developed recurrence at 90 and 132 days, respectively. Although detailed clarification concerning the process of donor selection and the indications for DSA-depleting interventions was desired, further information was unavailable due to data availability restrictions.Table 3. Profile and engraftment outcome of eight patients with high DSASCT, stem cell transplantation; HLA, human leukocyte antigen; DSA, donor-specific anti-HLA antibody; MFI, median fluorescence intensity; GVH, in graft-versus-host direction; HVG, in host-versus-graft direction; NCC, nuclear cell count; ALL, acute lymphoblastic leukemia; AML, acute myeloge1nous leukemia; CR, complete remission; MAC, myeloablative conditioning; RIC, reduced-intensity conditioning; NR, not reachedDuring the 5 years of TRUMP registry data, eight patients (0.20%) with MFI > 5,000 in the 3,882 patients received HLA-mismatched peripheral blood stem cell transplantation. Two patients (#4 and #6) underwent DSA-depleting depletion interventions. Only one patient (#7, red square) with DSA of MFI = 5,832 against B52:01 and transplanted with a sufficient number of CD34 + cells (6.37106/kg) without DSA-depleting intervention developed graft failure“-” denotes no available data
Discussion
One remarkable finding discovered after opening the data was that the background of the anti-HLA antibody-positive group differed from that of the negative group. The predominance of females, multiple transplantations, and HLA mismatches in the anti-HLA antibody-positive group could reasonably explain alloantibody production through the intervening variables of pregnancy and multiple transfusions. However, these differences could not explain the high cumulative incidence of neutrophil engraftment in the anti-HLA antibody-positive group compared with that in the anti-HLA antibody-negative group. Multivariate analyses revealed that CD34, HLA, mismatching in HVG direction, MMF-/ + , and MTX-/ + were significant for neutrophil engraftment, while anti-HLA antibody positivity was not among the covariates, which comprised anti-HLA antibody, age, sex, HLA-mis in GVH, HLA-mis-HVG, HCT-CI, disease status (CR or non-CR at SCT), CD34^+^, MAC/RIC, CsA/TAC, MMF-/ + , and MTX-/ + . This result was also true for the preliminary analyses with thresholds of MFI 3,000 and 1,000 (Supplemental data). This led us to assume that the better neutrophil engraftment in the anti-HLA antibody-positive group was due to confounding factors. Indeed, the presence or absence of HLA antibodies correlated with MTX use, and the difference between the effect of HLA antibodies disappeared in the MTX-adjusted cumulative incidence function (CIF). Since GVHD prophylaxis using TAC plus steroids in haploidentical transplantation has been widespread in Japan [11], prior information about the presence of HLA antibodies may have prevented a myelosuppressive MTX regimen. Regarding platelet engraftment, the presence of DSA has a slight negative effect on platelet engraftment. In multivariate analysis, this effect was observed only for DSA with MFI more than 5,000 and was not a significant factor for MFI 3,000 and 1,000 (Supplemental data). In contrast, HCT-CI and CD34^+^ were extracted as significant factors regardless of the MFI threshold. This suggests that the EBMT proposal of MFI 5,000 is reasonable as a “clinically significant” cut-off.
The impact of antibodies against loci other than HLA-A, B, C, and DRB1, specifically anti-HLA-DP, DQ, and DR3/4/5, should also be noted. In cord blood transplantation, the Toranomon Hospital group reported that HLA antibodies against HLA-DP, DQ, and DR3/4/5 adversely affect engraftment and nonrelapse mortality in their institute [12, 13]. The negative effect of HLA antibodies against HLA-DP and DQ was also documented in the cord blood transplantation provided by the Japanese Red Cross Kinki Cord Blood Bank [14]. In this study, donor HLA profiles were unavailable and were omitted from the analysis; however, future analyses including these profiles are warranted.
We found that only eight patients with high-DSA levels were registered in HLA-mismatched-related PBSCT in the TRUMP data. This Fig. (8/3,882 [0.2%]) is much smaller than expected (10–24%) based on the previously reported DSA prevalence [15]. This suggests that transplants with high DSA have been avoided, because the negative risk of DSA has become widely known. We found that seven of eight patients with high DSA (MFI > 5,000) achieved neutrophil engraftment. Conveying this fact is one of the objectives of this study. It remains unclear why some cases were engrafted even with high DSA levels. The biological hierarchy of anti-HLA antibodies in vivo is as follows: complement-binding IgG, viable cell-binding IgG, and flow bead-binding IgG. Ciurea et al. claimed that complement-dependent cytotoxicity, rather than antibody-dependent cell-mediated cytotoxicity, is a mainstay of graft rejection and that the presence of complement-binding IgG has the greatest impact on engraftment. However, methods for detecting complement-binding IgG (C1q assays) are not widely available [16, 9]. Viable cell-binding IgG, the second priority, is detected by physical cross-matching. Owing to the complexity of preparing viable donor cells, this method has recently been replaced with virtual cross-matching using flow beads. However, HLA coated on flow beads does not fully reproduce HLA expressed on viable cells, and the flow bead-based method also detects IgG that binds to cryptic epitopes not expressed on intact HLA in vivo [17]. This may explain why DSA-depleting therapy using transfusion of targeted HLA-expressing platelets may or may not decrease the flow-bead-based MFI [18]. A more fundamental problem is the MFI value. The flow bead method involves a mixture of several hundred colored single-HLA antigen-coated beads in one tube and the application of a serum sample; an anti-HLA antibody is an anti-HLA epitope (or eplet) antibody [19], for example, an antibody that binds to an HLA-A02:01-coated bead is a mixture of antibodies to multiple eplets of A02:01 (e.g., 9F, 44RM, 62GE, 65RA, 66 K) (http://www.epregistry.com.br). The MFI value of HLA-A02:01 reflected the sum of these antibodies. Since most eplets are shared by multiple HLAs, antibodies in the sample will also bind to beads of other HLAs sharing eplets with A02:01, resulting in an underestimation of the MFI value per bead (shared epitope phenomenon) [20]. Therefore, it should be recognized that the MFI value is only one indicator of the true amount of antibodies. In this series, except for B15:01 at #1 and B52:01 at #7 in the DSA-high group, the remaining HLA types are rare among Japanese individuals. Thus, it was considered that these antibodies might be natural antibodies. Natural antibodies, represented by flow bead-binding IgG among the aforementioned three, do not bind in vivo and therefore do not contribute to rejection.
In conclusion, contrary to previous reports, the effects of anti-HLA antibodies on engraftment were inconclusive. A limitation of the present study is that the sample population was already skewed owing to selection bias, and no valid statistical analysis was possible. However, it might be beneficial to determine the presence of patients with anecdotal cancer who achieved neutrophil engraftment despite high-DSA levels through a nationwide survey. Simultaneously, selecting patients who require DSA-depleting interventions is the next challenge.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementaryfile1 (DOCX 25 KB)