Male Occult Primary Breast Cancer Diagnosed with Small Bowel Metastases: A Case Report
Suguru Ogata, Uhi Toh, Kunihiro Ozaki, Yutaro Mihara, Nanae Ogata, Yuko Takao, Shuko Saku, Rie Sugihara, Fumihiko Fujita

TL;DR
A rare case of male occult breast cancer diagnosed through small bowel metastases is reported, highlighting the challenges in diagnosis and treatment.
Contribution
This case report adds to the limited literature on male occult breast cancer and its unusual metastatic patterns.
Findings
The patient was diagnosed with metastatic lobular breast cancer without an identifiable primary tumor.
The cancer responded to initial therapy but later developed brain metastases.
The case emphasizes the need for comprehensive diagnostic methods in male breast cancer.
Abstract
Male occult breast cancers are extremely rare and often difficult to diagnose. With only few cases reported, no established treatment is available. And metastatic spread to the small intestine from a tumor originating outside the peritoneal cavity is rare. However, there is a higher tendency for metastasis to the peritoneal cavity, including the small bowel, in the case of lobular carcinoma of the breast. A 72-year-old man who initially presented with complaints of abdominal distention. Computed tomography revealed small bowel stenosis. Post-endoscopic stenosis dilatation, an emergency small bowel resection was performed for small bowel perforation. Postoperative histopathology revealed small bowel metastasis due to mammary gland lobular carcinoma with human epidermal growth factor receptor 2 (3+), estrogen receptor-negative, and progesterone receptor-negative status; the patient was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
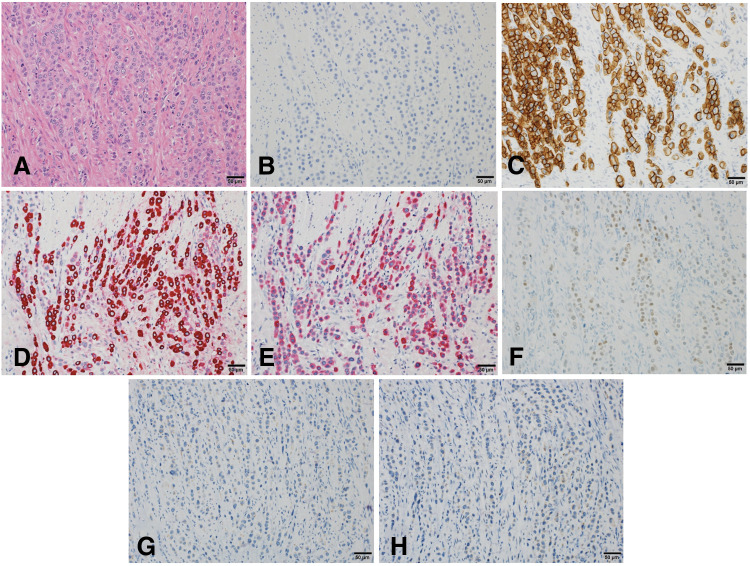 Fig. 1
Fig. 1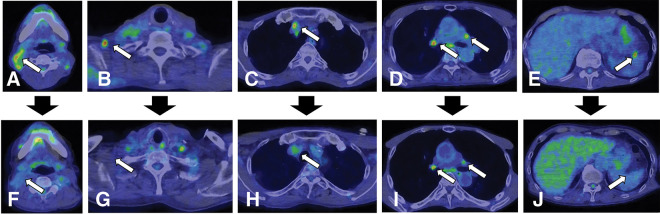 Fig. 2
Fig. 2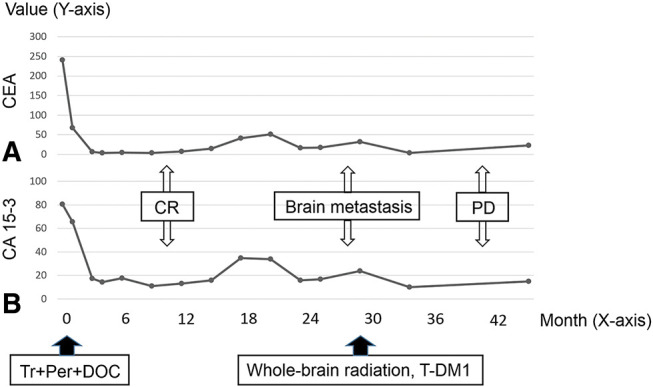 Fig. 3
Fig. 3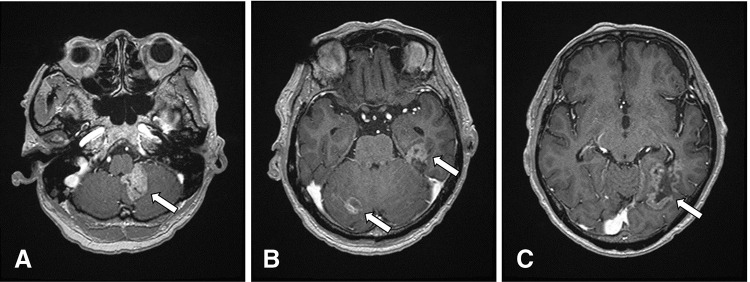 Fig. 4
Fig. 4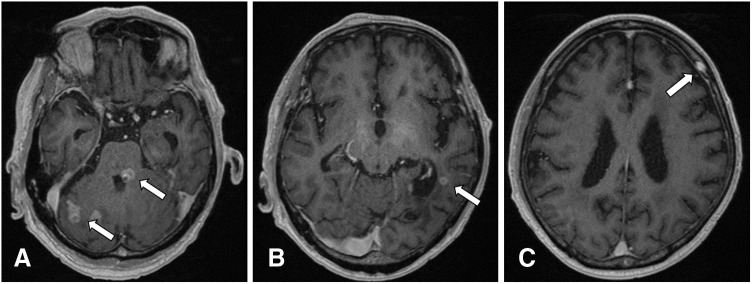 Fig. 5
Fig. 5| Study/reference | Age | TNM | Subtype | Local | Adjuvant | Recurrence | OS | Prognosis |
|---|---|---|---|---|---|---|---|---|
| Ogata et al., 2025 (present case) | 72 | T0N3M1 | ER(−), | Small bowel resection | Molecular targeted therapy, Chemotherapy, Radiotherapy | Brain | 52 | Death |
| Xu et al., 2017 | 29 | T0N3M0 | ER(+), | ALND and whole breast radiotherapy | Chemotherapy | None | 19 | Survival |
| Kuninaka et al., 2017 | 67 | T0N3M1 | ER(+), | Skin biopsy | Molecular targeted therapy | None | 33 | Survival |
| He et al., 2015 | 40 | T0N3M0 | ER(−), | Mastectomy with ALND | Endocrinotherapy, Chemotherapy | Lung and lymph nodes (Axillary and supraclavicular) | 27 | Survival |
| Gu et al., 2009 | 72 | T0N2M0 | ER(−), | Mastectomy with ALND | None | None | 24 | Survival |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMale Breast Health Studies · Cancer Diagnosis and Treatment · Cancer and Skin Lesions
Abbreviations
AKT1 AKT serine/threonine kinase 1 ALND axillary lymph node dissection BM brain metastases BRCA breast cancer susceptibility genes CA 15-3 carbohydrate antigen 15-3 CDH1 cadherin 1 CEA carcinoembryonic antigen CK cytokeratin DOC docetaxel ER estrogen receptor ERBB2 erb-b2 receptor tyrosine kinase 2 ESR1 estrogen receptor 1 FOXA1 forkhead box protein A1 GATA3 GATA-binding protein-3 GCDFP-15 gross cystic disease fluid protein-15 GM gastrointestinal metastases HBOC hereditary breast and ovarian cancer syndrome HER2 human epidermal growth factor receptor 2 IDC invasive ductal carcinoma IGFR1 insulin-like growth factor receptor 1 ILC invasive lobular carcinoma LFS Li-Fraumeni syndrome OBC occult breast cancers Per pertuzumab PR progesterone receptor SUVmax maximum standardized uptake value T-DM1 trastuzumab emtansine TP53 tumor protein p53 Tr trastuzumab WBRT whole-brain radiation therapy
INTRODUCTION
OBC, first reported by Halsted in 1907, is a rare entity characterized by axillary lymph nodes or distant organ metastases without identifiable primary breast lesions.^1)^ Most OBC involve axillary lymph node metastases, with distant metastases such as to the skin or brain rarely reported.^2,3)^ However, in some cases of OBC, metastases can appear in unexpected organs, including the small bowel. This occurrence is more commonly seen in metastatic breast cancer, particularly ILC of the breast.^4,5)^ Despite the developments in breast imaging, the incidence of OBC has not decreased; representing <1% of all breast cancers, and male patients account for only about 1% of OBC cases.^6)^ In this report, we demonstrate a case of male OBC with small bowel metastasis presenting obstruction.
CASE PRESENTATION
A 72-year-old man presented to his family doctor with complaints of abdominal distention lasting for about 2 months, accompanied by nausea, loss of appetite, and weight loss. CT revealed small bowel stenosis with proximal distension. Emergency small bowel resection was performed for a small perforation that developed after endoscopic stenosis dilatation. There was no family history of breast cancer or of other tumors; neither was there any sign of exposure to epidemiologic risk factors. Additionally, there was no notable past history suggesting a hereditary disease.
Postoperative pathological examination (Fig. 1A–1H) revealed invasion of cancer cells from the serosal surface of the small bowel. The tumor cells had pale eosinophilic cytoplasm and decreased cellular adhesion. Immunohistochemically, tumor cells were negative for ER, PR, and E-cadherin, but positive for HER2 (3+), mammaglobin, GCDFP-15, and GATA3. The patient was identified as ILC of the breast and was subsequently referred to our hospital for further evaluation and treatment.
Histopathological examination-immunohistochemistry (Scale bar = 50 μm). (A) Hematoxylin-Eosin: Pale eosinophilic cytoplasmic tumor cells with decreased cellular adhesion. (B) E-cadherin: negative. (C) Human epidermal growth factor receptor type 2: positive (3+). (D) Mammaglobin: positive. (E) Gross cystic disease fluid protein-15: positive. (F) GATA-binding protein-3: positive. (G) Estrogen receptor: negative, (H) Progesterone receptor: negative.
Blood serum levels of CEA and CA 15-3 were found to be elevated. Despite the unavailability of routine mammography for this extremely slender patient with smaller male breasts containing less glandular tissue, breast ultrasound, contrast-enhanced CT, and PET scan revealed no obvious neoplastic lesions or enlarged lymph nodes in the breast or axilla (Supplementary Fig. 1A–1H). PET scan (Fig. 2A–2E) showed multiple accumulation areas in the cervical lymph node, right supraclavicular lymph nodes, mediastinum, and pulmonary hilum (SUVmax = 2.8–7.1); abnormal accumulation was also observed in the splenic hilum (SUVmax = 3.9). Endoscopic examination revealed no esophago-gastrointestinal neoplastic lesion. Thus, we diagnosed the current case as OBC with multiple organ metastases.
Positron emission tomography scan (A–E: before chemotherapy; F–J: after chemotherapy). (A–D) Abnormal accumulation as indicated by maximum standardized uptake value (SUVmax) in cervical lymph node, right supraclavicular lymph nodes, mediastinum, and hilar region (SUVmax = 2.8–7.1) (arrows). (E) Abnormal accumulation as indicated by SUVmax = 3.9 at the splenic portal (arrow). (F–J) Loss of accumulation or reactive accumulation (arrows).
The patient’s progression is shown in Fig. 3. The patient was administered trastuzumab (Tr: Initial dose of 8 mg/kg followed by 6 mg/kg) plus pertuzumab (Per: Initial dose of 840 mg followed by 420 mg) plus docetaxel (DOC: 60 mg/m^2^) therapy in a 3-week cycle. PET scan obtained after 12 cycles showed that all areas of abnormal accumulation had disappeared or improved (Fig. 2F–2J), both serum levels of CEA and CA15-3 were normalized, and the patient achieved clinical complete response. At 18 months post-onset of chemotherapy, the serum levels of CEA and CA 15-3 increased once more (Fig. 3); however, no abnormal findings during the follow-up imaging were revealed. At 30 months after chemotherapy initiation, the patient experienced vertigo and lightheadedness, which worsened over time with the onset of neurological symptoms such as visual field disturbance and difficulty in walking. The head MRI (Fig. 4A–4C) showed multiple enhancing lesions in the left cerebellum, hippocampus, right cerebellum, and temporal-occipital lobe areas around the left temporal ventricle, near the left foramen of Luschka, which were diagnosed as multiple BM. For the treatment of multiple BM, the patient and his family opted not to pursue stereotactic radiosurgery; therefore, WBRT was chosen. After receiving second-line treatment with 30 Gy WBRT and 14 cycles of trastuzumab emtansine (T-DM1: 3.6 mg/kg, every 3 weeks), his neurological symptoms, activities of daily living, and the tumor markers showed improvement. However, head MRI (Fig. 5A–5C) revealed that although the originally noted metastases tended to shrink, new lesions had appeared in the left and right portions of the cerebellum, near the left lateral ventricle, and in the left frontal periosteum. The patient had a progressive disease, and palliative care with symptomatic treatment was provided based on the wishes of the patient and his family. He died 4 years and 4 months after treatment onset.
Treatment progress. (A) Carcinoembryonic antigen value transition. (B) Carbohydrate antigen 15-3 value transition.CA 15-3, carbohydrate antigen 15-3; CEA, carcinoembryonic antigen; CR, complete response; DOC, docetaxel; PD, progressive disease; Per, pertuzumab; T-DM1, trastuzumab emtansine; Tr, trastuzumab
Head magnetic resonance imaging after neurological symptoms. Multiple enhancing lesions within the brain (arrows). (A) Cerebellum near left foramen of Luschka. (B) Hippocampus, right cerebellum. (C) Temporal-occipital lobe around the left lateral ventricle.
Head magnetic resonance imaging after secondary treatment. Multiple new lesions within the brain (arrows). (A) Right and left-brain ventricles. (B) Near left lateral ventricle. (C) Left frontal periosteum.
DISCUSSION
Male OBC is extremely rare worldwide, making diagnosis challenging. Therefore, identifying metastatic sites using endoscopic and imaging methods, evaluating the primary site through histological examination with immunohistochemical analyses, and providing treatment based on the organ of origin are essential. Immunohistochemically, CK7 and CK20 are often used in the estimation of the primary organ, and addition of tissue-specific markers provide a higher estimation rate of the primary tumor. Generally, positive results for ER, PR, and HER2 staining support primary breast cancer diagnosis; however, this specificity is not sufficient. In addition to these markers, mammaglobin, GCDFP-15, GATA3, and lactalbumin are also useful in supporting the diagnosis of primary breast cancer. This case was diagnosed as OBC based on immunostaining results. Additionally, negative E-cadherin expression and HER2-positive findings suggested ILC.
The drug treatment strategies for ILC are generally recommended to follow the same protocols as those for typical invasive breast cancer.^7)^ While ILC is considered to have a relatively favorable prognosis compared with IDC, it is also reported to have a higher incidence of late recurrences.^8)^ Therefore, careful long-term follow-up is necessary for ILC patients. In terms of imaging diagnostics, MRI has been reported to have the highest sensitivity, ranging from 93% to 100%.^9)^ Additionally, several cohorts suggest that PET/CT modalities using 18F-fluciclovine or 18F-fluoroestradiol may be superior in detecting ILC metastases.^10,11)^
The mechanisms of metastasis in ILC remain unclear, though recent studies have identified potential correlations with its metastatic behavior. Immunophenotypic analyses have shown diverse interactions between hormone receptors and their cofactors as cancer progresses, particularly highlighting frequent downregulation of PR expression and variability in androgen receptor, GATA3, and FOXA1 across different metastatic sites within the same patient.^12)^ Additionally, several cohort studies have indicated an increased frequency of gene mutations, CDH1, AKT1, ESR1, IGFR1, and ERBB2, in metastatic ILC.^13,14)^ ILC metastasizes not only to common sites but also frequently to the peritoneum, ovaries, and the gastrointestinal tract.^5)^ Recognizing these patterns is crucial for the early diagnosis and effective disease management of ILC.
This case was diagnosed as male OBC based on histopathological findings, but the possibility of HBOC cannot be entirely ruled out. Although there is no notable family history or past history that would strongly suggest HBOC in this case, the association between HBOC and male breast cancer has been recognized, and it cannot be dismissed that this case may have had pathogenic BRCA 1/2 mutations.^15)^
In addition to HBOC, LFS is another hereditary condition associated with breast cancer. LFS is caused by germline TP53 mutations and is known to increase the risk of developing breast cancer.^16)^ Furthermore, it has been suggested that breast cancers arising in the context of pathogenic TP53 mutations are more likely to exhibit HER2 amplification.^17)^ Considering the rarity of HER2-positive subtype male breast cancer patients, it cannot be ruled out that this case may have harbored a pathogenic TP53 mutation.
Male breast cancer is generally known to have a very high ER and PR positivity rate (more than 80%) and a low HER2 positivity rate.^18)^ However, this case was a very rare immunophenotype with ER and PR-negative and HER2-positive. To our knowledge, this is the fifth case of a HER2-positive male OBC (Table 1).^19–22)^ Three of the 4 previously reported cases involved only axillary lymph node metastasis, and only 1 case involved distant skin metastasis. All M0 cases underwent at least mastectomy, ALND, or WBRT, resulting in disease control. However, unlike most of the previously reported cases, our case was not accompanied by axillary lymph node metastasis but involved the small bowel at diagnosis and was a stage IV disease.
HER2-positive breast cancer is known to have a higher incidence of BM compared with other subtypes.^23)^ For cases of BM, the efficacy of drugs such as tucatinib and trastuzumab deruxtecan has been suggested, and recent advancements in systemic therapy have significantly improved clinical outcomes.^7,24)^
GM from breast cancer occur in approximately 10% of all metastatic cases, with few reports on male breast cancer.^25)^ The reported case we identified involved hormone receptor-positive and HER2-positive IDC, whereas our case presented as hormone receptor-negative and HER2-positive ILC.^26)^ It is known that GM are more commonly derived from lobular carcinoma than from ductal carcinoma.^5)^ Furthermore, a significant difference between the reported case and the present case is that the present case involved male OBC.
Due to its rarity, male OBC is often advanced by the time symptoms appear. As in the present case, where metastases are observed at nonspecific sites at the time of diagnosis, distinguishing them as breast cancer becomes more challenging. Given this context, we cannot rule out the possibility that some cases of male OBC may be treated as cancers of unknown primary origin. To effectively screen for such cases, it is crucial for clinicians to understand the characteristics of male OBC, develop research designs and guidelines specific to this condition, and standardize the diagnostic and treatment processes.
CONCLUSIONS
We report a case of male OBC. For male OBC, it is important to understand the potential metastatic patterns and genetic factors, as well as to utilize comprehensive diagnostic methods for early diagnosis and disease management.
SUPPLEMENTARY MATERIALS
Supplementary Fig. 1. Imaging findings at diagnosis. No abnormal findings were observed in the breast or axillary lymph node area on ultrasound examination (a–d), contrast-enhanced computed tomography scan (e, f), or positron emission tomography scan (g, h).
ACKNOWLEDGMENTS
The authors thank Editage (www.editage.jp) for English language editing.
DECLARATIONS
Funding
Not applicable.
Authors’ contributions
SO: design concept, investigation, acquisition of data, drafting, and revision of the article.
UT: design concept, revision and editing, and supervision.
KO: acquisition of data and revision and editing.
YM: diagnosis of pathological histology and revision of the manuscript.
NO: acquisition of data and revision and editing.
YT: revision and editing.
SS: revision and editing.
RS: acquisition of data and revision and editing.
FF: revision and editing and supervision.
All authors have read and approved the final manuscript.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics approval and consent to participate
This work does not require ethical considerations or approval. Informed consent to participate in this study was obtained from the patient.
Consent for publication
Written informed consent for publication of the case details and images was obtained from the patient.
Competing interests
The authors declare that they have no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Halsted WSI. The results of radical operations for the cure of carcinoma of the breast. Ann Surg 1907; 46: 1–19.17861990 10.1097/00000658-190707000-00001 PMC 1414357 · doi ↗ · pubmed ↗
- 2Matsubara Y Yamashita T Suganuma N A case of male occult breast cancer diagnosed with skin metastasis. Nihon Rinsho Geka Gakkai Zasshi 2021; 82: 1648–52. (in Japanese)
- 3Hosomura M Toi M Hayashi K An occult breast cancer developed after craniotomy for metastatic brain tumor. J Jpn Pract Surg Soc 1996; 57: 850–3. (in Japanese)
- 4Hani MB Attuwaybi B Butler B. Breast cancer metastasis to the colon and rectum: review of current status on diagnosis and management. Int Surg 2019; 104: 508–13.
- 5Mc Cart Reed AE Kalinowski L Simpson PT Invasive lobular carcinoma of the breast: the increasing importance of this special subtype. Breast Cancer Res 2021; 23: 6.33413533 10.1186/s 13058-020-01384-6PMC 7792208 · doi ↗ · pubmed ↗
- 6Siegel RL Miller KD Jemal A. Cancer statistics, 2020. CA Cancer J Clin 2020; 70: 7–30.31912902 10.3322/caac.21590 · doi ↗ · pubmed ↗
- 7National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: breast cancer, version 4. 2024. https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (Accessed 25 September 2024).
- 8Van Baelen K Geukens T Maetens M Current and future diagnostic and treatment strategies for patients with invasive lobular breast cancer. Ann Oncol 2022; 33: 769–85.35605746 10.1016/j.annonc.2022.05.006 · doi ↗ · pubmed ↗