A novel reshapable catheter facilitates selective biliary and pancreatic duct cannulation following endoscopic submucosal dissection including papilla
Haruo Miwa, Kingo Hirasawa, Kazuki Endo, Ritsuko Oishi, Yuichi Suzuki, Hiromi Tsuchiya, Shin Maeda

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
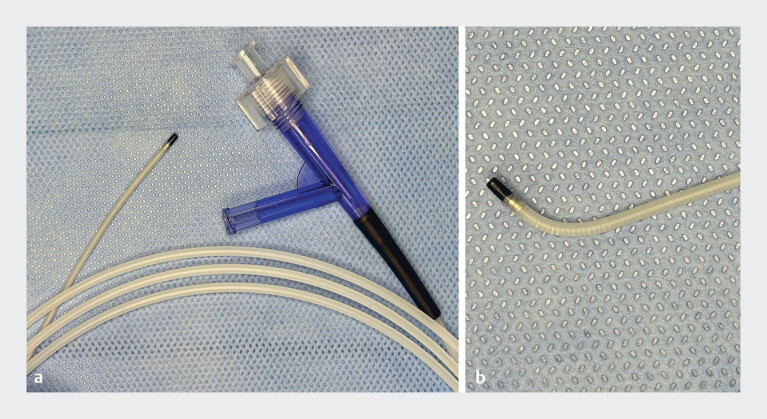 Fig. 1
Fig. 1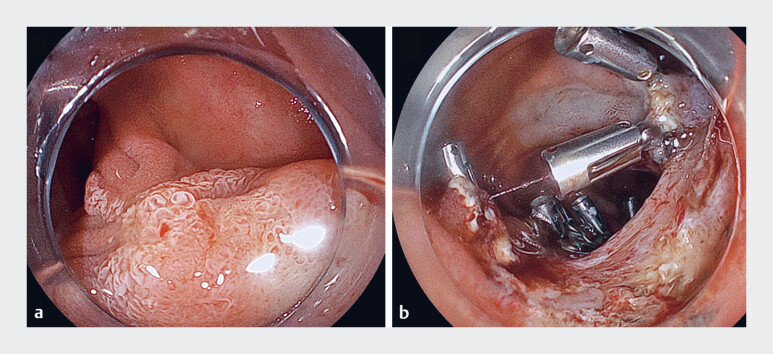 Fig. 2
Fig. 2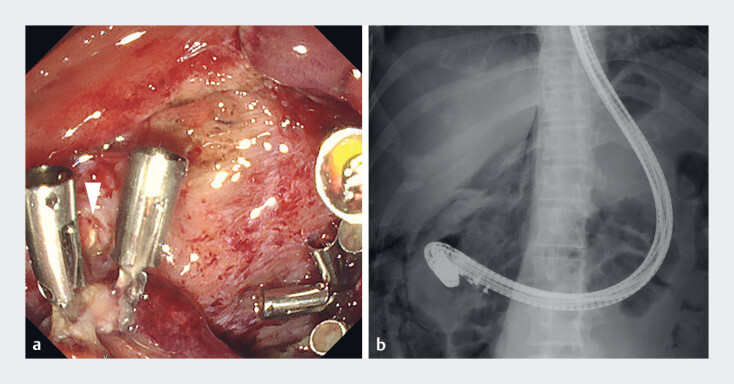 Fig. 3
Fig. 3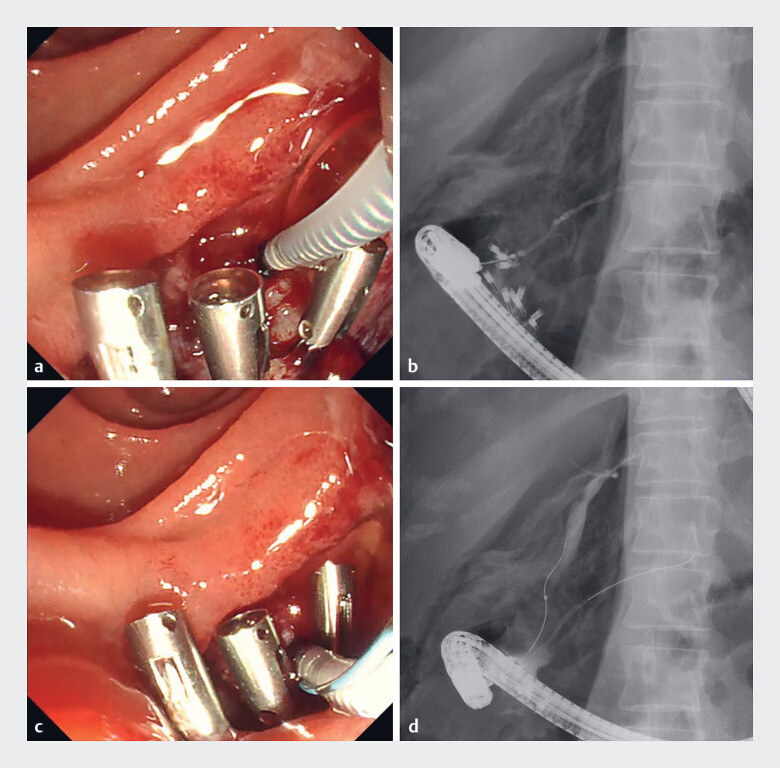 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Esophageal and GI Pathology · Gastric Cancer Management and Outcomes
Endoscopic submucosal dissection including the papilla (ESDIP) carries the risk of delayed bleeding and perforation 1 2 ; therefore, endoscopic nasobiliary and nasopancreatic duct drainage (ENBPD) is recommended to prevent adverse events 3 4 . However, after ESDIP, the maneuverability of the duodenoscope is restricted, making it difficult to align with the axes of the bile duct and pancreatic ducts for cannulation. A novel reshapable catheter (VEGA; Japan Lifeline Co., Ltd., Tokyo, Japan) features a coiling shaft that allows for easy manual adjustment to an appropriate angle ( Fig. 1 ).
The novel reshapable catheter (VEGA; Japan Lifeline Co., Ltd., Tokyo Japan). a The catheter features a coiling shaft. b The tip of the catheter allows for easy manual adjustment to an appropriate angle.
A 41-year-old woman was referred to our hospital because of a laterally spreading tumor involving the papilla. ENBPD was planned to prevent adverse events following ESDIP ( Fig. 2 , Video 1 ). A duodenoscope (TJF-290V; Olympus Medical Systems, Tokyo, Japan) was inserted into the second part of the duodenum ( Fig. 3 ). The duodenal lumen was narrowed due to clipping performed during ESDIP. The orifices of the bile and pancreatic ducts were identified beyond the clips. The axis of the pancreatic duct ran downward. First, the novel reshapable catheter was used in a straight shape. Pancreatography was successfully performed before guidewire insertion. The bile duct axis appeared to run upward. The catheter was manually reshaped to adjust to the direction of the bile duct. The tip of the catheter was gently positioned at the orifice of the bile duct and the guidewire was successfully inserted. Cholangiography confirmed successful bile duct cannulation ( Fig. 4 ). Subsequently, nasopancreatic duct and nasobiliary tubes were placed, and the duodenoscope was carefully withdrawn. The patient experienced no complications, and she was discharged on Day 8.
Endoscopic images. a A laterally spreading tumor involving the papilla. b After endoscopic submucosal dissection, the duodenal lumen was narrowed due to clipping.
After endoscopic submucosal dissection including the papilla. a The orifices of the bile and pancreatic ducts were identified beyond the clips (arrowhead). b The maneuverability of the duodenoscope was restricted.
Selective biliary and pancreatic duct cannulation. a The axis of the pancreatic duct ran downward. The catheter was used in a straight shape. b Pancreatic duct cannulation was successfully performed. c The bile duct axis appeared to run upward. The catheter was manually reshaped to adjust to the direction of the bile duct. d Cholangiography confirmed successful bile duct cannulation.
The novel reshapable catheter was useful for biliary and pancreatic duct cannulation after endoscopic submucosal dissection including the papilla.Video 1
To the best of our knowledge, this is the first report describing the use of a novel reshapable catheter for selective biliary and pancreatic duct cannulations. This catheter facilitates cannulation in challenging cases where duodenoscope maneuverability is restricted.
Endoscopy_UCTN_Code_TTT_1AR_2AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yahagi N Takatori Y Sasaki M Feasibility of endoscopic submucosal dissection including papilla (with video)Dig Endosc 20253740241039489706 10.1111/den.14942 · doi ↗ · pubmed ↗
- 2Dohi O Iwai N Yoshida N Endoscopic submucosal dissection for duodenal tumors including papilla: is it feasible?Dig Endosc 20253741141210.1111/den.1499139810694 · doi ↗ · pubmed ↗
- 3Fukuhara S Kato M Iwasaki E Management of perforation related to endoscopic submucosal dissection for superficial duodenal epithelial tumors Gastrointest Endosc 2020911129113710.1016/j.gie.2019.09.02431563595 · doi ↗ · pubmed ↗
- 4Fukuhara S Kato M Iwasaki E External drainage of bile and pancreatic juice after endoscopic submucosal dissection for duodenal neoplasm: feasibility study (with video)Dig Endosc 20213397798433258135 10.1111/den.13907 · doi ↗ · pubmed ↗