Inhalation of a gastric polyp upon removal
Ke Liu, Yuqing Chen, Xiaoli Ren, Lizhi Yi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
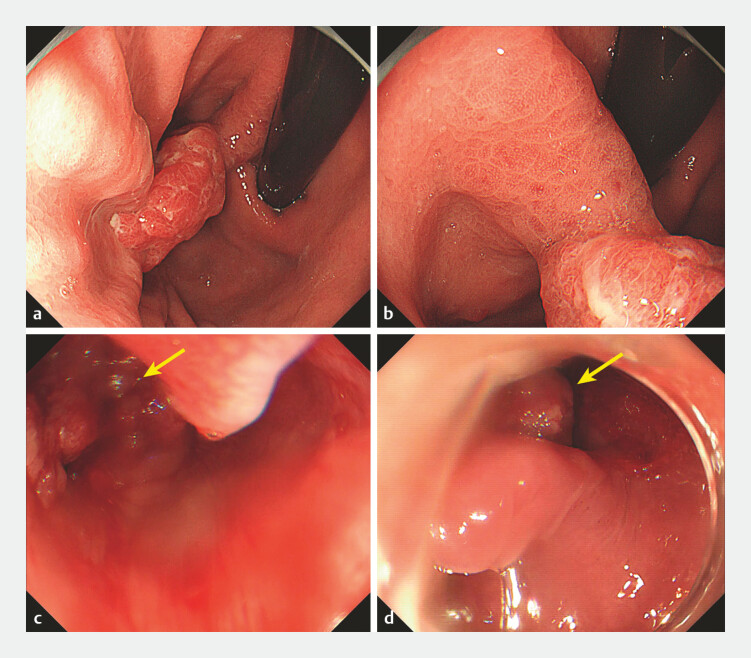 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Gastric Cancer Management and Outcomes
A 48-year-old man was admitted to our hospital for gastric polyp removal. His history and physical examination were unremarkable, and coagulation was normal.
After the patient had been anesthetized with propofol, esophagogastroduodenoscopy was performed and revealed a 2-cm type Isp polyp in the lesser curvature of the gastric fundus ( Fig. 1 a, b ). The polyp was removed by endoscopic mucosal resection. Thereafter, a snare was used to extract the sample. When passing through the esophageal entrance, the removed gastric polyp accidentally fell off the snare. When the gastroscope returned, the sample was inhaled into the trachea ( Fig. 1 c , Video 1 ). The patient was immediately placed in a semiprone position. Then, transnasal gastroscopy was performed with the intention of entering the trachea. Fortunately, before entering the trachea, the patient coughed out the specimen, which was eventually removed successfully ( Fig. 1 d ).
Endoscopy images. a, b Esophagogastroduodenoscopy revealed a 2-cm type Isp polyp in the lesser curvature of the gastric fundus. c The removed gastric polyp (arrow) fell into the hypopharynx. d The patient coughed out the specimen (arrow).
The specimen was inhaled into the trachea.Video 1
The patient experienced no discomfort postoperatively. Postoperative computed tomography of the lungs was normal. The histopathology of the specimen was gastric villous adenoma.
Common complications of gastric polyp resection include throat pain, abdominal distention, bleeding, and perforation 1 2 . Specimen aspiration has not been reported previously. It was inferred that the main cause of the aspiration was that the snare was pulled too loose. Our case shows that more attention should be given when the specimen passes through the entrance of the esophagus.
Endoscopy_UCTN_Code_CPL_1AH_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Perisetti A Goyal H Tharian B Endoscopic resection of multiple large gastric polyps Endoscopy 20215365966010.1055/a-1244-914732916726 · doi ↗ · pubmed ↗
- 2Landin MD Guerrón AD Endoscopic mucosal resection and endoscopic submucosal dissection Surg Clin North Am 20201001069107810.1016/j.suc.2020.07.00433128880 · doi ↗ · pubmed ↗