Trend, Epidemiology, and Clinical Characteristics of Vulvar Cancers in Lagos, Nigeria: A Facility-Based Study
Adeyemi A Okunowo, Oluwatoyin M Olayioye, Muhammad Y Habeebu, Chinedu C Anumni, Ephraim O Ohazurike, Kehinde S Okunade, Rose I Anorlu

TL;DR
This study examines the rising trend and characteristics of vulvar cancer in Lagos, Nigeria, highlighting its late-stage diagnosis and the need for increased awareness.
Contribution
The study provides new insights into the epidemiology and clinical features of vulvar cancer in a Nigerian setting.
Findings
Vulvar cancer accounted for 4.0% of all gynecological cancers in Lagos, with a rising trend in cases over the study period.
Most patients were postmenopausal, had multiple sexual partners, and presented with advanced-stage disease.
Abstract
Background Vulvar cancer (VC) is a rare gynecological cancer (GC) that is not commonly studied. Because of its location, vulvar symptoms are not frequently brought to the clinician’s attention. Many women are not aware of VC and frequently attribute its early symptoms to other benign causes. In addition, little is known about the disease epidemiology and clinical characteristics in Lagos, Nigeria. Objectives Our study aimed to describe the trend, epidemiology, and clinical characteristics of VC in Lagos, Nigeria. Materials and methods Records of women with VC who presented to Lagos University Teaching Hospital between January 2010 and December 2019 were retrieved, and information on their socio-demographic and clinical characteristics was obtained for analysis. Data analysis was done using IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
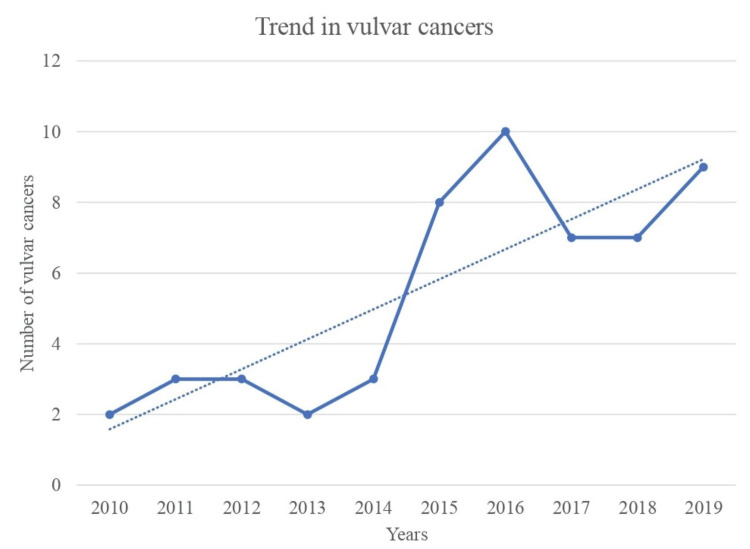 Figure 1
Figure 1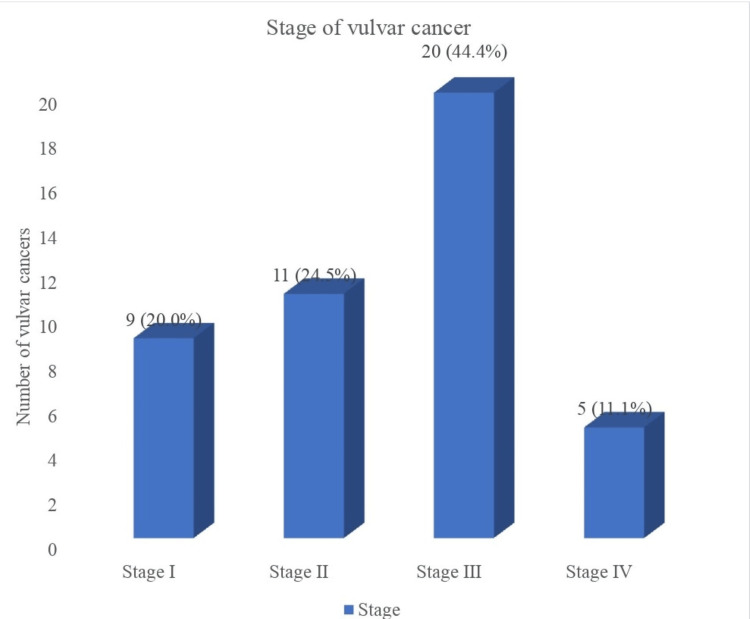 Figure 2
Figure 2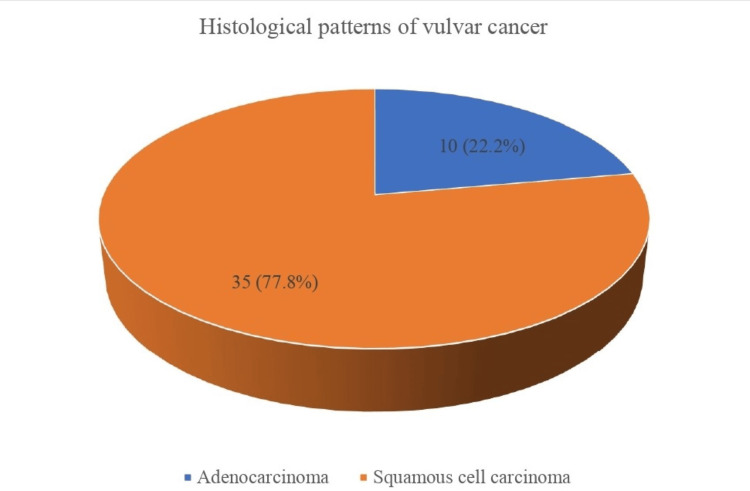 Figure 3
Figure 3| VARIABLE | FREQUENCY (n=45) | PERCENTAGE |
| Age at presentation (Years) | ||
| <40 | 9 | 20.0 |
| 40 to 49 | 9 | 20.0 |
| 50 to 59 | 15 | 33.3 |
| ≥60 | 12 | 26.7 |
| Mean ± SD | 52.2 ± 11.8 | |
| Marital status | ||
| Single | 4 | 8.9 |
| Married | 22 | 48.9 |
| Divorced | 1 | 2.2 |
| Separated | 2 | 4.4 |
| Widow | 16 | 35.6 |
| Educational status | ||
| Primary | 9 | 20.0 |
| Secondary | 26 | 57.8 |
| Tertiary | 10 | 22.2 |
| Ethnic | ||
| Yoruba | 19 | 42.2 |
| Igbo | 20 | 44.4 |
| *Others | 6 | 13.4 |
| Religion | ||
| Christianity | 36 | 80.0 |
| Islam | 9 | 20.0 |
| Occupation | ||
| Skilled | 1 | 2.2 |
| Semi-skilled | 18 | 40.0 |
| Unskilled | 17 | 37.8 |
| Unemployed | 9 | 20.0 |
| VARIABLE | FREQUENCY (n=45) | PERCENTAGE (%) |
| Children Alive | ||
| <2 | 14 | 31.1 |
| 2-4 | 18 | 40.0 |
| ≥5 | 13 | 28.9 |
| Median (IQR) | 3 (1-5) | |
| Parity | ||
| 0 | 5 | 11.1 |
| 1 to 4 | 21 | 46.7 |
| ≥5 | 19 | 42.2 |
| Median (IQR) | 4 (1-6) | |
| Menarche (years) | ||
| <12 | 1 | 2.2 |
| 12 to 14 | 24 | 53.4 |
| >14 | 20 | 44.4 |
| Mean ± SD | 14.4 ± 1.3 | |
| Menopausal status | ||
| Menopausal | 26 | 57.8 |
| Pre-Menopausal | 19 | 42.2 |
| Multiple sexual partners | ||
| No | 16 | 35.6 |
| Yes | 29 | 64.4 |
| Age at coitarche | ||
| >18 | 7 | 15.6 |
| 18 to 21 | 26 | 57.8 |
| >21 | 12 | 26.6 |
| Mean ± SD | 19.9 ± 2.5 | |
| Number of sexual partners | ||
| 1 | 16 | 35.6 |
| 2 to 3 | 22 | 48.9 |
| >3 | 7 | 15.6 |
| Median (IQR) | 2 (1-3) |
| VARIABLE | FREQUENCY (n=45) | PERCENTAGE (%) |
| HIV infection | ||
| Yes | 5 | 11.1 |
| No | 40 | 88.9 |
| History of genital warts | ||
| Yes | 35 | 77.8 |
| No | 10 | 22.2 |
| History of cervical dysplasia or cancer | ||
| Yes | 2 | 4.4 |
| No | 43 | 95.6 |
| Vulva skin lesion | ||
| Yes | 40 | 88.9 |
| No | 5 | 11.1 |
| History of Smoking | ||
| Yes | 2 | 4.4 |
| No | 43 | 95.6 |
| Chronic use of steroids | ||
| Yes | 11 | 24.4 |
| No | 34 | 75.6 |
| VARIABLE | FREQUENCY (n=45) | PERCENTAGE (%) |
| Symptoms | ||
| Asymptomatic | 8 | 17.8 |
| Vulvar swelling | 32 | 71.1 |
| Pruritus vulvae | 14 | 31.1 |
| Abnormal vulvo-vaginal bleeding | 10 | 22.2 |
| Abnormal vaginal discharge | 15 | 33.3 |
| Vulva ulcer | 15 | 33.3 |
| Vulva pain | 2 | 4.4 |
| Examination findings | ||
| Vulvar mass | 39 | 86.7 |
| Vulvar bleeding | 3 | 6.7 |
| Vulva ulceration | 9 | 20.0 |
| Discharge | 8 | 17.8 |
| Abnormal skin lesion | 8 | 17.8 |
| VARIABLE | FREQUENCY (n=45) | PERCENTAGE |
| Treatment modalities | ||
| Surgery alone | 15 | 33.3 |
| Chemotherapy alone | 4 | 8.9 |
| Radiotherapy alone | 4 | 8.9 |
| Chemoradiation alone | 4 | 8.9 |
| Surgery and chemotherapy | 3 | 6.7 |
| Surgery and radiotherapy | 2 | 4.4 |
| Surgery and chemoradiation | 1 | 2.2 |
| No treatment received | 12 | 26.7 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Endometrial and Cervical Cancer Treatments · Global Cancer Incidence and Screening
Introduction
The vulva is an essential part of the female genitalia called the external genitalia, and it comprises the labia majora, labia minora, clitoris, bulb of the vaginal vestibule, the lesser vestibular glands also called the Skene glands, and the greater vestibular glands known as the Bartholin’s glands [1]. It is a private region of the female’s body reserved for sexual and reproductive activities, and cancer can arise from any of its components. Vulva cancer (VC) is a rare gynecological malignancy, accounting for barely 1% of all female cancers and 4% of all reproductive tract cancers [1,2]. According to the GLOBOCAN 2022 report, VC is the fourth most common genital tract cancer, after cervical, uterine, and ovarian cancers, with 47,342 new cases and 18,579 cancer deaths reported worldwide, accounting for 0.2% of the total new cases of cancers and cancer deaths, respectively, in 2022 [3]. The incidence and mortality burden of VC is highest in Europe and Asia, with Africa accounting for an incidence and mortality rate of 11.9% and 16.1%, respectively [4]. In Nigeria, 1056 new cases and 579 deaths were attributed to VC in 2022, accounting for less than 1% of all new cancer cases and cancer-related deaths, respectively [5].
Approximately 80-95% of VC are squamous cell carcinoma (SCC) in origin, followed by melanoma and other rare histologic types [1,6]. There are two major histological variants of SCC, and they arise from different etio-pathological pathways with distinct characteristics. Keratinizing SCCs are human papillomavirus (HPV)-independent, arising from chronic vulvar dystrophies like lichen sclerosus, squamous hyperplasia, and differentiated vulvar intraepithelial neoplasia (dVIN). This is the most common variant, accounting for about 60% of all SCC, and it typically occurs in older women above 60 years. Warty or basaloid SCC is an HPV-associated cancer, commonly caused by high-risk HPV (hr-HPV) similar to the ones causing cervical cancer, especially HPV 16, 18, 31, and 33. It is usually multifocal in origin, occurs in younger women, and accounts for approximately 30% of all SCC [1,6]. SCC may arise from preneoplastic lesions in the vulvar and anal regions generally referred to as lower anogenital squamous intraepithelial lesions. Low squamous intraepithelial lesions (LSIL), formerly referred to as vulvar intraepithelial neoplasia 1 (VIN 1), and high squamous intraepithelial lesions (HSIL), formerly referred to as VIN 2 & 3, are precursor lesions of HPV-associated SCC, while dVIN is associated with chronic vulvar dermatoses and keratinizing SCC with more aggressive malignant behavior compared with HSIL [1,6].
Due to its occurrence at a late age, VC is typically referred to as a disease of menopause. However, following the advent of HIV/AIDS and the high prevalence of HPV infection, its incidence has significantly increased, and the age at onset of the disease has decreased [1,6]. The risk factors for VC are multifaceted and include age, HR-HPV infections, HIV/AIDS, history of cervical cancer, presence of cervical or vulvar HSIL, chronic vulvar dystrophies such as lichen sclerosus, smoking, and immunosuppression [7]. Bucchi et al. [8], in a systematic review, reported on other risk factors associated with VC, such as the presence of other sexually transmitted diseases, autoimmune diseases such as systemic lupus erythematosus, familial clustering of HPV-associated cancers, metabolic syndrome, diabetes mellitus, and high body mass index. Similarly, sexual behavior and practices like early age at coitarche, high number of sexual partners, type of sexual intercourse, total number of marriages, and age at first marriage have been reported to be associated with the risk of VC, though with some conflicting results [8]. Women with VC can either present with symptoms or be asymptomatic. Common symptoms include pruritus vulvae, vulvar growth or nodule, ulcerative lesions, vulvar pain, discharge, bleeding, or dysuria [9,10].
VC has been poorly studied worldwide due to the rarity of the disease, leading to a lack of adequate statistical data to guide recommendations and management [11,12]. Studies on VC are very few in Nigeria, resulting in a poor understanding of the epidemiology, clinical characteristics, and management strategy of the disease among Nigerian women. Among the few studies conducted in Nigeria [13-16], none has been conducted in Lagos State, Nigeria, leaving a huge knowledge gap in the understanding of the epidemiology and characteristics of VC in a cosmopolitan and the most populous city in Nigeria and Africa. To bridge this gap, our study aimed to examine the trend of VC and describe the epidemiology and clinical characteristics of the disease in Lagos State, Nigeria.
Materials and methods
Study design and setting
This was a retrospective cross-sectional study conducted among women with histological diagnoses of VC who received care at the Lagos University Teaching Hospital (LUTH), Lagos State, Nigeria. LUTH is the main and largest referral center for cancer management in Lagos State, southwestern Nigeria. It has approximately 760 beds and caters to the huge population of about 25 million people living in the twenty local government areas of the state [17] and its neighborhood. It has facilities for complex cancer surgery, radiation therapy, chemotherapy, and palliative care.
Study population and eligibility criteria
This included all women with histological diagnoses of VC managed at LUTH over a 10-year period from January 1st, 2010, to December 31st, 2019. Women who had histologically confirmed VC during the study period with complete data were enrolled in the study, while women without histological confirmation of VC or with missing or incomplete data were excluded from the study.
Data collection
The medical record register of all patients who attended the LUTH gynecological oncology outpatient clinic, gynecological accident & emergency unit, and radiotherapy outpatient clinic or were admitted into the female in-lying wards during the 10-year study period was reviewed to identify women with a diagnosis of VC who received care in the hospital during the period. The medical records of these women were identified and retrieved from the medical records department, and appropriate information was obtained using a structured study proforma. Information on sociodemographic characteristics, reproductive characteristics, risk factors for VC, and symptoms at presentation was obtained. Information on the stage at presentation, histological types, and mode of treatment of VC were also retrieved from the case notes. The information on the number of women managed for gynecological malignancies in the institution during the study period was also obtained to determine the burden of VC relative to other gynecological malignancies.
Data analysis
The collected data was entered into a Microsoft Excel spreadsheet, de-identified, cleaned, and validated. Statistical analysis was done using IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp. Variables were grouped into continuous and categorical variables. Continuous variables were tested using the Shapiro-Wilk test for normal distribution, and normally distributed and skewed variables were expressed as mean ± standard deviation (SD) and median with interquartile range (IQR), respectively, while categorical variables were grouped into different categories. Descriptive statistics of variables were computed and presented in frequency tables or charts.
Ethical consideration
Ethical approval (ADM/DCST/HREC/APP/3572) was obtained from LUTH’s Human Research and Ethical Committee before conducting the study. The study was carried out in accordance with the Declaration of Helsinki (1964).
Results
A total of one thousand, three hundred and forty-nine (1,349) cases of gynecological malignancies were managed at LUTH during the study period. During this period, VC accounted for 54 (4.0%) of all gynecological malignancies and an approximate average annual frequency of five cases per year. Out of the 54 cases of VC identified, only 45 (83.3%) cases had complete data and were included in the study analysis.
Figure 1 shows the trend in the number of VCs seen over the 10-year study period. There was a rising trend in the number of VCs managed within the institution, from two cases in 2010 to nine cases in 2019, with a peak of 10 cases in 2016. More than three-quarters, 41 (75.9%), of VC cases were managed within the last five years (2015-2019), compared to just 13 (24.1%) managed within the first five years (2010-2014) of the study period.
Trend in vulvar cancers over 10 years.There was an increasing trend in the number of vulvar cancers seen during the study period.
Table 1 shows the sociodemographic characteristics of women with VC. The majority, 27 (60.0%) of the women were above the age of 50 years at presentation with a mean ± SD age of 52.2 ± 11.8 years (25 - 74 years). Most of the women were married, 22 (48.9%), Christians, 36 (80.0%), of Igbo ethnicity, 20 (44.4%) with semi-skilled and unskilled occupations, 35 (77.8%), and had at least secondary school education, 26 (57.8%).
Table 2 shows the reproductive and sexual characteristics and risk factors for VC among the study participants. A large proportion of women, 19 (42.2%), has had at least five deliveries with a median (IQR) parity of 4 (1-6), while 18 (40.0%) had between two and four children with a median (IQR) of 3 (1-5). Most of the women, 29 (64.4%), had a history of multiple sexual partners, with the majority, 22 (48.9%), having two to three sexual partners, and the median (IQR) number of sexual partners was 2 (1-3). The mean ± SD age at coitarche was 19.9 ± 2.5 years; many women, 26 (57.8%), initiated sexual activities between 18 and 21 years, and more than half, 26 (57.8%), were postmenopausal.
Most of the women with VC had a history of genital warts, 35 (77.8%), and vulva skin lesions, 40 (88.9%), before the diagnosis of VC. Only five (11.1%) were HIV positive, while two (4.4%) had a history of cervical dysplasia or cancer. Only a minority, 11 (24.4%) and two (4.4%) had a history of chronic use of steroids and smoking of tobacco, respectively (Table 3).
The most common presenting symptoms of VC were vulvar swelling (32 cases, 71.1%), vulvar ulcer (15 cases, 33.3%), vaginal discharge (15 cases, 33.3%), and pruritus vulvae (14 cases, 31.1%). Similarly, the common examination findings in women with VC were vulvar mass (39 cases, 86.7%) and vulvar ulceration (nine cases, 20.0%) as shown in Table 4.
Figure 2 illustrates the stages of VC. The majority, 20 (44.4%), of women with VC presented in stage III disease, while 11 (24.5%) and 9 (20.0%) presented in stages II and I, respectively. More than half of the women, 25 (55.5%), presented with late-stage disease.
The stages of vulvar cancer at presentation.Most women with vulvar cancer present with stage III disease, followed by stage II, I, and IV disease.
The most common histological type of VC among women in the study was squamous cell carcinoma, accounting for 35 (77.8%), while 10 (22.2%) women have adenocarcinoma (Figure 3).
Histological patterns of vulvar cancer over 10 years.The most common histological type of VC was squamous cell carcinoma, followed by adenocarcinoma.
Table 5 shows the various treatment modalities for VC during the study period. Surgery was the most common single modality of treatment for VC, 15 (33.3%), followed by chemotherapy, four (8.9%), and radiotherapy, four (8.9%). Chemoradiation, four (8.9%); surgery followed by chemotherapy, three (6.7%); and surgery and radiotherapy, two (4.4%), were the most common combination therapies received for the treatment of VC, while 12 (26.7%) did not receive any treatment, mainly due to financial inability to afford care.
Discussion
VC is a rare disease that has not received much attention worldwide due to the investment of resources and focus of research on “the big three” gynecological cancers, i.e., cervical, ovarian, and endometrial cancers, which are more prevalent and associated with more cancer-related morbidity and mortality. Africa and other LMICs have contributed very little to the available epidemiological knowledge on VC, with minimal research output on the subject matter, leaving a knowledge gap in the understanding of the disease in the region. To bridge this gap, our study examined the trend in VC cancer over a 10-year period and described the epidemiological and clinical characteristics of the disease in Lagos State, Southwestern Nigeria.
VC accounted for 54 (4.0%) of the total gynecological cancers seen during the 10-year survey. This is in keeping with the widely reported 4.0-5.0% prevalence of the disease among other gynecological cancers [1,2,9,11,12]. Though this prevalence was similar to the 3.6% reported at Port Harcourt, South-southern Nigeria [15], it was higher than what was reported at Nnewi, Southeastern Nigeria (1.27%) [13], Zaria, Northwestern Nigeria (2.6%) [16], and Ibadan, Southwestern Nigeria (1.6%) [18], but lower than what was reported at Benin, South-southern Nigeria (5.7%) [14]. In Africa, VC accounted for 2.0% of all gynecological cancers in Ghana [19], while in Burkina Faso it accounted for 5.3% [20]. The variation in the prevalence of VC may be attributed to the variation in the prevalence of its etiological and risk factors, such as chronic vulvar dystrophies, HPV-related infections, and HIV/AIDS, in different populations. We found a rising trend in the number of cases of VC presenting to the institution for care during the study period. This is similar to the increasing incidence reported in the United Kingdom [21] and the United States of America [22] but contrary to the stable trend observed in Croatia [6]. Globally, a rising trend has been observed among elderly women, while a mixed trend was observed among young women [23]. This is mainly due to the increase in the aging population and the high prevalence of HPV infections [21].
In our study, the majority, 17 (60.0%), of the women with VC were within the menopausal age of 50 years and beyond, with a mean age at presentation of 52.2 years, and were menopausal (57.8%), in keeping with the assertion that VC is a disease of menopause, and that age plays a critical role in its epidemiology [21]. Compared to other centers in Nigeria, a lower mean age at presentation was reported in Ibadan (49.7 years) [18], Zaria (45.4 years) [16], and Port Harcourt (49.0 years) [15], while a higher mean age at presentation was seen at Nnewi (61.2 years) [13]. In Africa, higher mean ages at diagnosis were observed in Ghana (56.3 years) [19], Tunisia (65.4 years) [24], and Burkina Faso (55 years) [20], while a much higher age at diagnosis, between 70 and 73 years, was reported in high-income countries [6,12,25].
Approximately 80.0% and almost all (97.8%) of the women with VC in our study had secondary or primary education levels and low-level occupations, respectively, which suggests a low socioeconomic status (SES). This is consistent with findings by Ouh et al. [26], where VC was more prevalent in women with low SES. Low SES has been shown to be associated with an increased risk of developing HPV-related cancers due to more frequent exposure to sexual activities, which increases the risk of acquisition and persistence of high-risk HPV infections, and the poor uptake of HPV preventive practices by this group of women [26,27]. HPV infection is responsible for 40% of VC [11], and the rising rate of the infection in many LMICs has been implicated to be responsible for the high incidence of the disease in the region [10]. It is therefore not surprising that the majority of women with VC in our study had a history of multiple sexual partners, with approximately two-thirds having two or more sexual partners. Similarly, there was a high rate of prior genital wart disease among these women but a low rate of cervical dysplasia or cancer. This may be due to a low cervical screening rate, which is frequent among low SES and women with VC [26]. Vulvar dystrophies and vulvar intraepithelial neoplasm are common risk factors for VC, and these usually present with abnormal vulvar skin lesions, which were reported by the majority of women with VC in our study. Unfortunately, the actual diagnoses of these vulvar skin lesions are not known, as many women believe that they are signs of vulvar infections. As a result, they do not present early with these symptoms for proper evaluation but usually rely on self-treatment and over-the-counter medications only to present late when the disease has progressed. The prevalence of other known risk factors such as HIV/AIDS, smoking, and chronic use of steroids was, however, low among women in our study.
Vulvar swelling or mass, vulvar ulcer, abnormal discharge, and pruritus vulvae were the frequent presenting symptoms of VC in our study, which are consistent with the common symptoms reported in several studies [11,13,15,19,28,29]. Vulvar swelling or mass was the most common presenting symptom of VC in Lagos, similar to what was reported in other studies [11,19,21,28,30], while pruritus vulvae [13,24,29], vulvar ulcer [20,21], vulvar pain [15,20], and discharge [15] were the most common symptoms reported by other authors.
The majority (55.5%) of women with VC in Lagos presented with advanced VC. This is in line with findings from other regions in the country, with Zaria, Northwestern Nigeria [16], Port Harcourt, South-southern Nigeria [15], and Nnewi, Southeastern Nigeria [14], having between 80.0% and 100.0% rates of advanced-stage disease. A similar finding of late-stage presentation was observed in other African countries [19,24] and Iran [28]. On the contrary, the incidence of late-stage presentation of VC is lower in high-income countries, with rates ranging between 19.0% and 39.0% [12,25,30]. The most common stage at presentation of VC in Lagos was stage III disease. This is consistent with the stage at presentation in other regions in Nigeria [13-16] and Africa [24]. On the other hand, stage I disease is the most common stage at presentation in many high-income countries [12,25,30].
Squamous cell carcinoma was the most common histological type of VC in Lagos, accounting for approximately 80.0% of all the VC, which is in keeping with the findings in the literature [1], while adenocarcinoma accounted for the remaining percentage. The most common single treatment modality for VC was surgery alone in one-third of VC cases, followed by chemotherapy and radiotherapy alone, while chemoradiation and surgery followed by either chemotherapy or radiotherapy were the most common combination therapies. The use of radiotherapy and chemotherapy is a common and important form of treatment modality for VC in our environment due to the frequent presentation of advanced-stage diseases that are non-resectable, incompletely resected with positive surgical margins, or with nodal involvement. Unfortunately, more than a quarter of women with VC did not receive any treatment due to their inability to afford care. The majority of these women had advanced VC and could not afford the cost of chemo-radiation due to the lack of health insurance and government support for cancer care.
Limitations
The study was a single institutional-based study with a limited study population, which may not represent the true population characteristics of VC in the general population. As a result, these findings cannot be generalized. Being a retrospective study, its findings are limited by the availability, completeness, and quality of the data in the medical record. Furthermore, the use of paper-based medical records may also affect the quality of data collected. The small sample size also limits the accuracy and reliability of the study findings. A large prospective multicenter study is recommended for a more comprehensive and reliable evaluation of the epidemiology of VC in Lagos and Nigeria at large.
A major strength of our study is that it is the first study, to the best of our knowledge, to describe the trend, epidemiology, and clinical characteristics of VC in Lagos, Nigeria. This will serve as a baseline study for future epidemiological research on VC in the state and region.
Conclusions
VC is a rare gynecological cancer in Lagos, Nigeria, accounting for 4.0% of gynecological cancers in LUTH. It is more prevalent among women with advanced age, multiple sexual partners, low levels of occupation, and postmenopausal women. The most common symptom at presentation is vulvar swelling or mass, and women with VC frequently present in advanced-stage disease, commonly stage III. The most common histological type is squamous cell carcinoma, and the majority of the women received either surgical treatment, chemotherapy, or radiotherapy, with a significant proportion of the women not receiving any care due to financial constraints. There is a need to increase public awareness about the disease among women to enhance early presentation, provide and subsidize preventive measures such as HPV vaccination, and treat women with VC to improve health outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer of the vulva: 2021 update Int J Gynaecol Obstet Olawaiye AB Cuello MA Rogers LJ 718155 Suppl 120213466920410.1002/ijgo.13881 PMC 9298362 · doi ↗ · pubmed ↗
- 2Prognostic factors for vulvar cancer Acta Clin Croat Miljanović-Špika I MadunićMD Topolovec Z 253260202110.20471/acc.2021.60.01.04PMC 830535334588718 · doi ↗ · pubmed ↗
- 3Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin Bray F Laversanne M Sung H 2292637420243857275110.3322/caac.21834 · doi ↗ · pubmed ↗
- 4International Agency for Research on Cancer: Global cancer observatory: cancer today: vulva 2 2024 2024 https://gco.iarc.who.int/media/globocan/factsheets/cancers/21-vulva-fact-sheet.pdf
- 5International Agency for Research on Cancer: Global cancer observatory: cancer today Nigeria Nigeria 2 2024 2024 https://gco.iarc.who.int/media/globocan/factsheets/populations/566-nigeria-fact-sheet.pdf
- 6Epidemiology of vulvar cancer in Croatia Croat Med J BarišićI Čukelj P Brkić BilošI Šekerija M 1031096420233713131210.3325/cmj.2023.64.103PMC 10183957 · doi ↗ · pubmed ↗
- 7European society of gynaecological oncology guidelines for the management of patients with vulvar cancer - update 2023 Int J Gynecol Cancer Oonk MH Planchamp F Baldwin P 102310433320233736937610.1136/ijgc-2023-004486 PMC 10359596 · doi ↗ · pubmed ↗
- 8New insights into the epidemiology of vulvar cancer: systematic literature review for an update of incidence and risk factors Cancers (Basel) Bucchi L Pizzato M Rosso S Ferretti S 14202210.3390/cancers 14020389 PMC 877387335053552 · doi ↗ · pubmed ↗