A Case of Spontaneously Resolving Valsalva Retinopathy in a 29-Year-Old Patient
Dawid Woszczek, Aleksandra Górska, Sebastian Sirek, Dorota Wyględowska-Promieńska

TL;DR
A 29-year-old patient with Valsalva retinopathy experienced spontaneous resolution of vision loss without surgery.
Contribution
This case report highlights the spontaneous resolution of Valsalva retinopathy in a young patient.
Findings
The patient's visual acuity improved from 0.4 to 1.0 over one month.
The hemorrhage under the inner limiting membrane decreased significantly in size.
Non-surgical management with observation led to recovery without intervention.
Abstract
Valsalva retinopathy (VR) occurs when a sudden rise in pressure within the thoracic or abdominal cavity results in a pre-retinal hemorrhage. The elevated venous pressure leads to increased blood flow through the retinal vessels, causing the rupture of peripapillary capillaries. This rupture leads to unilateral or bilateral pre-retinal hemorrhage, with blood pooling beneath the inner limiting membrane (ILM). A 29-year-old patient presented to the Emergency Eye Care Unit of the Professor Kornel Gibiński University Hospital Center of the Silesian Medical University in Katowice due to deterioration of vision in the right eye over the past five days. On physical examination, the visual acuity (VA) in the right eye was 0.4, and the ocular pressure was 24 mmHg. In the left eye, the VA was 1.0, and the ocular pressure was 22 mmHg. A fundus examination showed a tear-shaped hemorrhage in the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
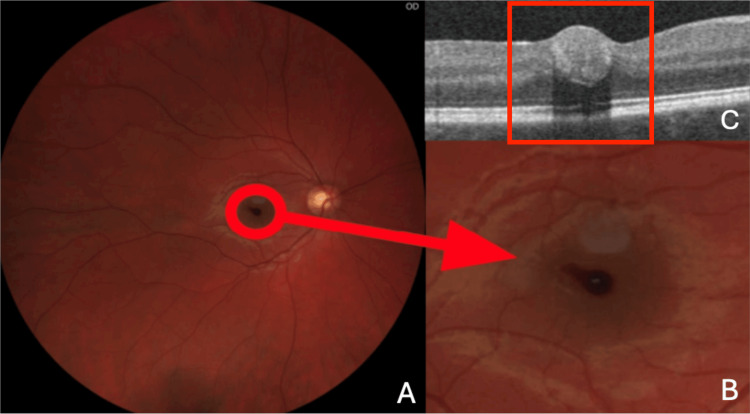 Figure 1
Figure 1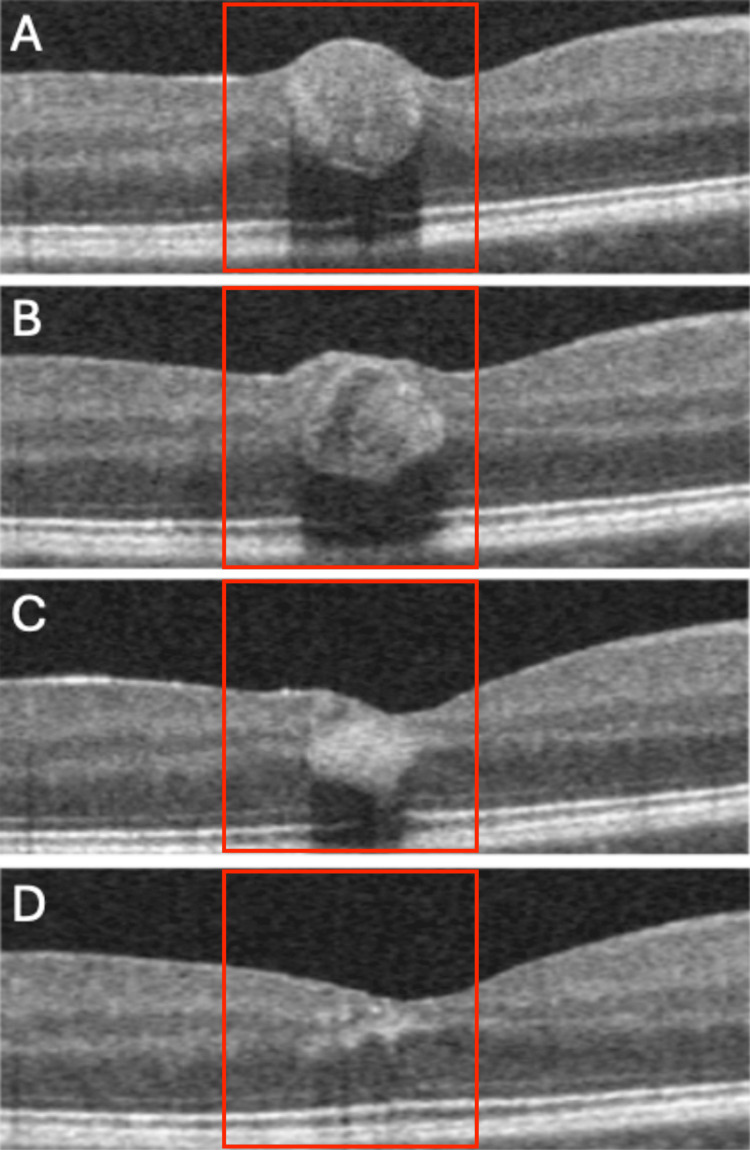 Figure 2
Figure 2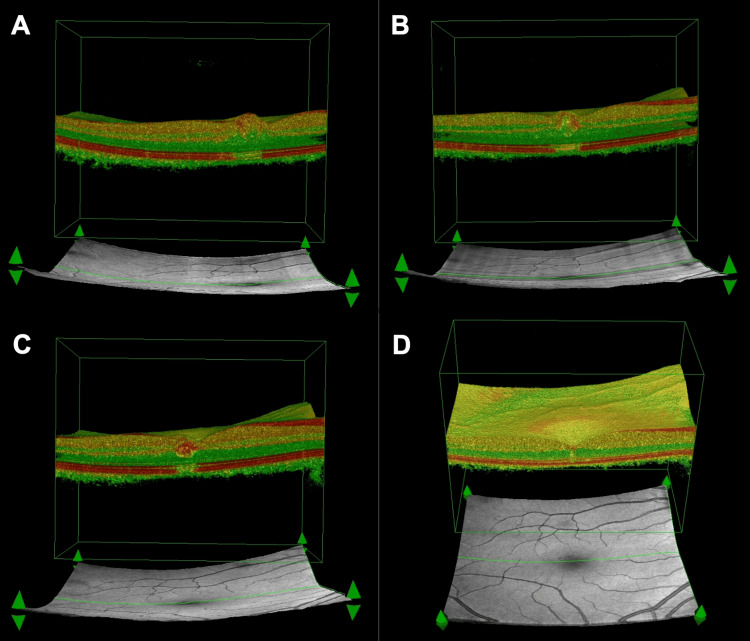 Figure 3
Figure 3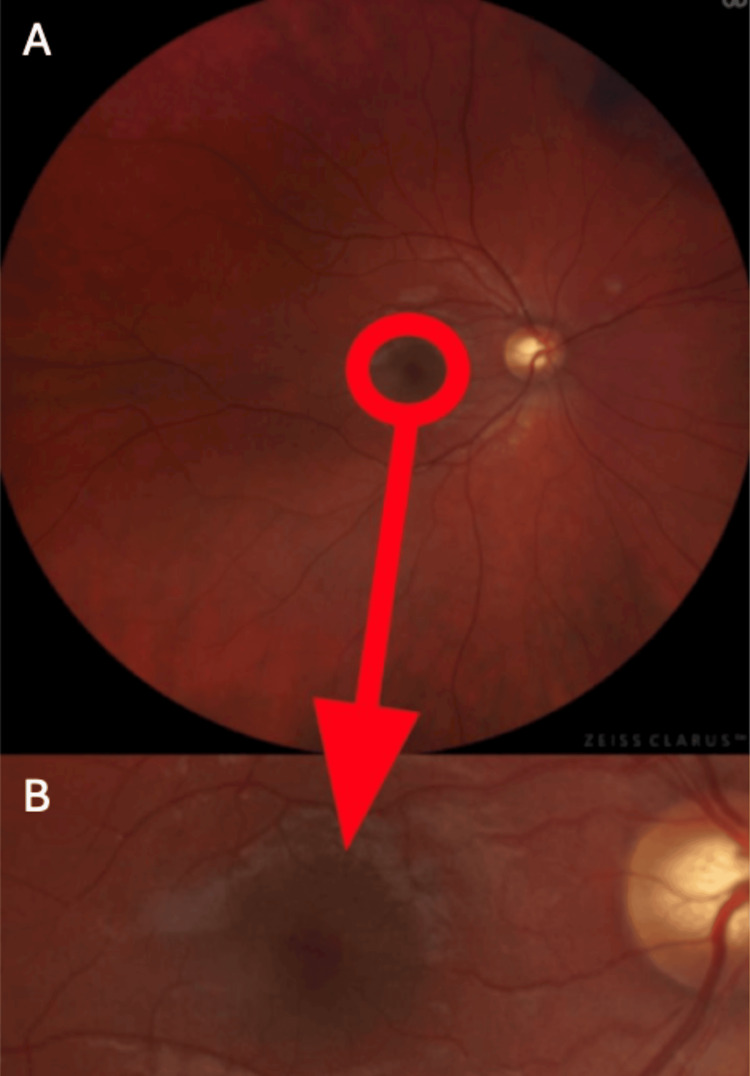 Figure 4
Figure 4| Dimensions (µm) | Test date | Visual acuity |
| 524 x 246 | September 18, 2024 | 0.4 |
| 516 x 211 | September 26, 2024 | 0.5 |
| 400 x 151 | October 3, 2024 | 0.6 |
| 152 x 62 | October 17, 2024 | 1.0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Brain Injury and Neurovascular Disturbances · Child Abuse and Related Trauma · Cerebrospinal fluid and hydrocephalus
Introduction
Valsalva retinopathy (VR) is a pre-retinal hemorrhage resulting from a sudden increase in pressure within the thoracic or abdominal cavity. First described by Duane in 1972 [1], this phenomenon is considered rare, with its exact epidemiology still not well-documented in the scientific literature. However, it is known to primarily affect individuals who engage in activities that provoke rapid and significant pressure changes, such as intense physical exertion, coughing, vomiting, labor, straining during defecation, or thorax-abdominal trauma [2-5].
The pathophysiology of VR is based on a sudden rise in venous pressure, which causes a corresponding increase in blood flow through the retinal vessels. This increased flow exerts pressure on the fragile peripapillary capillaries, leading to their rupture and the subsequent leakage of blood into the pre-retinal space. The hemorrhaged blood then accumulates beneath the inner limiting membrane (ILM) of the retina, which typically results in the characteristic appearance of a flame-shaped hemorrhage [6]. Such hemorrhages are often located near the optic disc, and their size and location vary depending on the severity of the event. The clinical presentation of VR usually includes a sudden, painless loss of vision in one or both eyes, often described as visual disturbances or the presence of floaters. Patients may also experience a temporary or permanent decrease in visual acuity (VA), particularly if the hemorrhage is large or involves the macular region [7-9].
While the condition is often self-limiting, with many patients experiencing spontaneous resolution of the hemorrhage, the severity and duration of visual symptoms can vary. Although the majority of VR cases resolve without intervention, treatment options - including laser photocoagulation, intravitreal anti-vascular endothelial growth factor (anti-VEGF) injections, or even vitrectomy - may be considered for more severe or persistent cases. These approaches aim to reduce the risk of further retinal damage and improve visual outcomes, especially in patients with significant symptoms or recurring hemorrhages [10].
Case presentation
A 29-year-old patient presented to the Emergency Eye Care of the Professor Kornel Gibiński University Hospital Center of the Silesian Medical University in Katowice due to deterioration of vision in the right eye for five days. In addition to the decreased VA, the patient reported in his history that he had been seeing a central spot, which had not moved with the eyeball’s movement, in the right eye for five days. The patient noticed the first signs of vision deterioration after bending down. In his history, the patient denied any comorbidities. On physical examination, VA in the right eye was 0.4, and intraocular pressure (IOP) was 24 mmHg; in the left eye, it was 1.0 mmHg and 22 mmHg, respectively. As shown in Figures 1A-1B, a fundus examination revealed a tear-shaped hemorrhage in the fovea, the size of which did not exceed that of one optic nerve disc.
Fundus of the right eye, on the day the patient reported to the emergency room, and the corresponding OCT image.(A) Photograph of the fundus of the right eye, with a tear-shaped hemorrhage (arrow) in the fovea visible; (B) Close-up image of a tear-shaped hemorrhage (arrow) in the fovea; (C) OCT scan, with a tear-shaped hemorrhage (box) in the fovea visible.OCT, optical coherence tomography
On admission, optical coherence tomography (OCT) (Optovue AngioVue; Optovue, Inc., Fremont, CA, USA) of the right eye was performed, which confirmed the presence of hemorrhage under the ILM, with dimensions of 524 μm × 246 μm. Observation and avoidance of physical activity were recommended. At the first follow-up, seven days after the patient's report, the VA of the right eye was 0.5 on examination. OCT of the right eye was performed again, and the size of the hemorrhage was measured, obtaining dimensions of 516 μm × 211 μm. The dimensions had decreased from the previous visit. In the subsequent follow-ups, which took place 14 days and one month after enrollment, respectively, the VA of the right eye was 0.6 and 1.0. On OCT, the dimensions of the hemorrhage decreased to 400 μm × 151 μm and 153 μm × 62 μm, respectively. All the above data have been presented in Figure 2 and Table 1.
Subsequent follow-up of self-limiting intraretinal hemorrhage captured on OCT scans.(A) OCT image of hemorrhage on admission day; (B) OCT image after 1 week; (C) OCT image after 2 weeks; (D) OCT image after 4 weeks.OCT, optical coherence tomography
The process of spontaneous reduction of preretinal hemorrhage was visualized in the 3D OCT projection, as shown in Figure 3.
Process of spontaneous restriction of intraretinal hemorrhage in 3D OCT projection.Subsequent follow-up of self-limiting intraretinal hemorrhage with 3D OCT images with dates.(A) Visible intraretinal hemorrhage (date of the scan: September 18, 2024); (B) Visibly reduced intraretinal hemorrhage (date of the scan: September 26, 2024); (C) Visibly more reduced intraretinal hemorrhage (date of the scan: October 3, 2024); (D) Invisible intraretinal hemorrhage (date of the scan: October 17, 2024).
During subsequent follow-ups, self-limitation of the hemorrhage was observed until it completely disappeared after 35 days, achieving full return of VA and stabilization of IOP at 20 mmHg. The effect of restriction of the hemorrhage was captured on a fundus image, presented in Figure 4.
A fundus image showing the complete absorption (arrow) of the intraretinal hemorrhage.(A) Photograph of the fundus of the right eye showing the complete absorption of the hemorrhage; (B) Close-up photograph of the fundus of the right eye showing the complete absorption of the hemorrhage.
Discussion
In the available literature, various treatment methods are considered, among the main options are observation, Nd-YAG (neodymium-doped yttrium aluminum garnet) laser hyaloidotomy, pneumatic displacement of hemorrhage by intravitreal injection of gas with or without recombinant tissue plasminogen activator (rTPA), and pars plana vitrectomy (PPV).
Mukherjee et al. highlight the fact that preretinal hemorrhage and sub-ILM hemorrhage resolve spontaneously in most cases, with a good visual outcome. Intervention with Nd:YAG laser or surgery is not necessary unless the patient wants a faster visual recovery, or there is a breakthrough hemorrhage into the vitreous. Gaseous injection of rTPA into the vitreous may be an effective treatment when the hemorrhage is in the deeper layers of the retina [11].
Studies by subsequent authors have shown that PPV is the most effective treatment for patients with severe intraretinal hemorrhage located under the ILM and insufficient spontaneous reabsorption. The most important intra- and post-operative complications of PPV use include secondary macular hole and accelerated cataract formation [12,13]. Hemorrhages with a diameter of less than one normal optic disc, as in the case described here, tend to resolve spontaneously in a short period of time, and a conservative approach is generally justified. In contrast, spontaneous resolution of large and dense hemorrhages is highly unlikely [13].
One common intervention is drainage with the Nd-YAG laser. The laser can be useful in treating preretinal hemorrhages that are not dense, have not coagulated, and when the blood is not localized under the ILM. Close proximity to the retinal surface risks the formation of a macular hole or a persistent pre-retinal defect. Further complications described include retinal detachment or epiretinal membrane formation [14,15].
Each time, the possibility of mislocalization of blood must be taken into account, even with advanced retinal imaging techniques, such as high-resolution OCT.
Conclusions
Successful management of VR depends on the timing and size of the hemorrhage. Despite severe visual impairment in the early stages of the disease, VA is usually restored to normal levels. For hemorrhages smaller than the size of one normal optic disc, management includes close observation and avoidance of strenuous physical activity. This is a minimally invasive and safe method, especially for a young, active patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Valsalva hemorrhagic retinopathy Trans Am Ophthalmol Soc Duane TD 298313701972 https://pubmed.ncbi.nlm.nih.gov/4663671/4663671 PMC 1310456 · pubmed ↗
- 2Valsalva retinopathy induced by vigorous nightclub dancing Med J Aust Sueke H 33319020091929681710.5694/j.1326-5377.2009.tb 02427.x · doi ↗ · pubmed ↗
- 3Valsalva retinopathy in pregnancy: SD-OCT features during and after Nd:YAG laser hyaloidotomy Ophthalmic Surg Lasers Imaging Jayaprakasam A Matthew R Toma M Soni M 0842201110.3928/15428877-20110210-0621366206 · doi ↗ · pubmed ↗
- 4Valsalva retinopathy induced by labour Eur J Ophthalmol Ladjimi A Zaouali S Messaoud R Ben Yahia S Attia S Jenzri S Khairallah M 3363381220021222000910.1177/112067210201200417 · doi ↗ · pubmed ↗
- 5Valsalva and Purtscher's retinopathy with optic neuropathy in compressive thoracic injury Eye (Lond) Chandra P Azad R Pal N Sharma Y Chhabra MS 914915192005 https://doi.org/10.1038/sj.eye.67016651535924010.1038/sj.eye.6701665 · doi ↗ · pubmed ↗
- 6Internal limiting membrane: the innermost retinal barrier Med Hypotheses Chawla R Tripathy K Temkar S Kumar V 60629820172801260810.1016/j.mehy.2016.11.017 · doi ↗ · pubmed ↗
- 7Valsalva retinopathy in twin-pregnancy: a case report and literature review Am J Case Rep Li N Zhu Z Yi G Li S Han X 591920182929236610.12659/AJCR.905738 PMC 5757405 · doi ↗ · pubmed ↗
- 8Postcoital visual loss due to valsalva retinopathy: a case report Ann Med Surg (Lond) Mahjoub A Ben Abdesslem N Ben Abderrazek A 1047218220223626828410.1016/j.amsu.2022.104721 PMC 9577858 · doi ↗ · pubmed ↗