Prevalence and Determinants of Sexual Dysfunction in Male Diabetic Patients in Saudi Arabia: A Cross-Sectional Study
Sherif M Zaki, Mohammed A Zahra, Saleem Alshobaki, Yousef Salamah, Nawaf Al-Nazzawi, Hussain Al-Taffi, Abdulaziz Yassin, Obai Yamani

TL;DR
This study found that most male diabetic patients in Saudi Arabia experience sexual dysfunction, with age, smoking, and diabetes duration being key risk factors.
Contribution
The study provides new insights into the prevalence and determinants of sexual dysfunction among diabetic men in Saudi Arabia.
Findings
85% of participants had erectile dysfunction and 47% had premature ejaculation.
Age, smoking, and diabetes duration were significant risk factors for both conditions.
High triglycerides and abnormal cholesterol levels increased the risk of sexual dysfunction.
Abstract
Introduction In Saudi Arabia, sexual health among diabetic men is one aspect that is less explored, unlike other complications related to diabetes. This study aimed to look at the prevalence of erectile dysfunction (ED) and premature ejaculation (PE) in male Saudi patients with diabetes and their risk factors. Methods A cross-sectional study targeting 100 male diabetic patients was carried out at Dr. Soliman Fakeeh Hospital in Jeddah, Kingdom of Saudi Arabia. Participants provided demographic and medical history information and underwent laboratory investigations, including glycated hemoglobin (HbA1c), lipid profiles, and markers of renal function. We evaluated sexual dysfunction using the International Index of Erectile Function and the Premature Ejaculation Diagnostic Tool. Results Eighty-five percent of participants had ED and 47% had PE. Erectile dysfunction (ED) was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
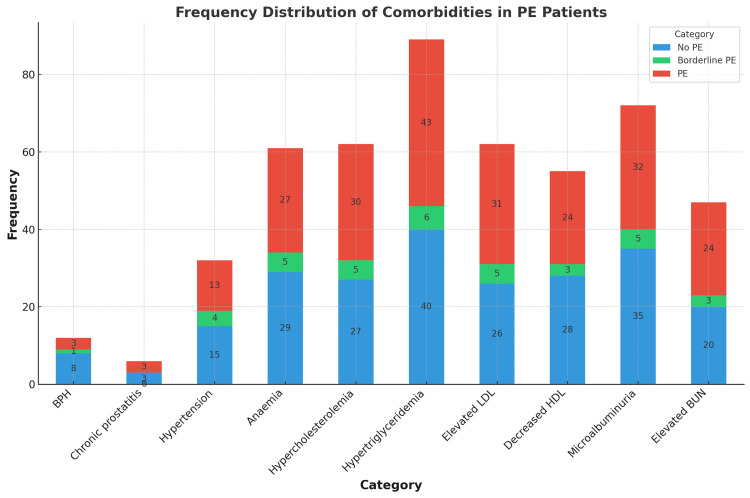 Figure 1
Figure 1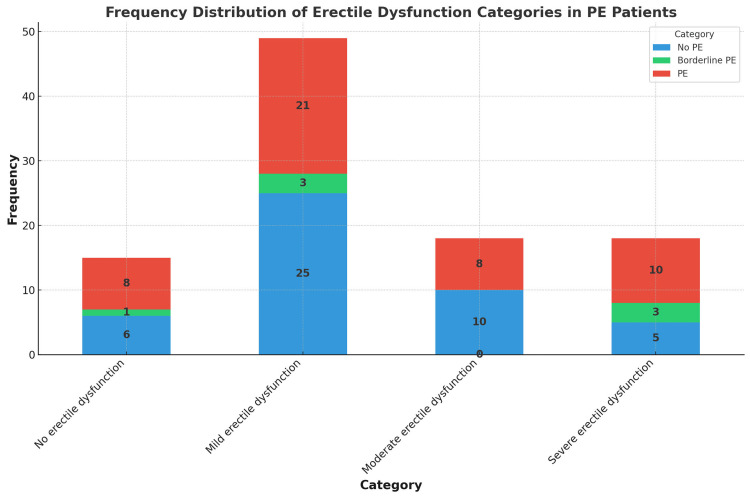 Figure 2
Figure 2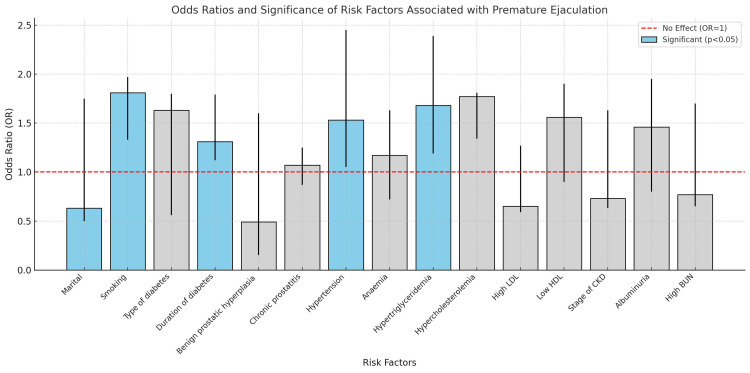 Figure 3
Figure 3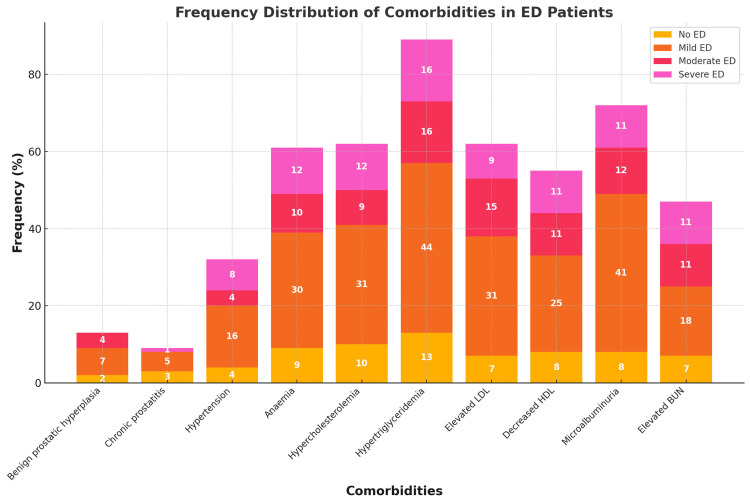 Figure 4
Figure 4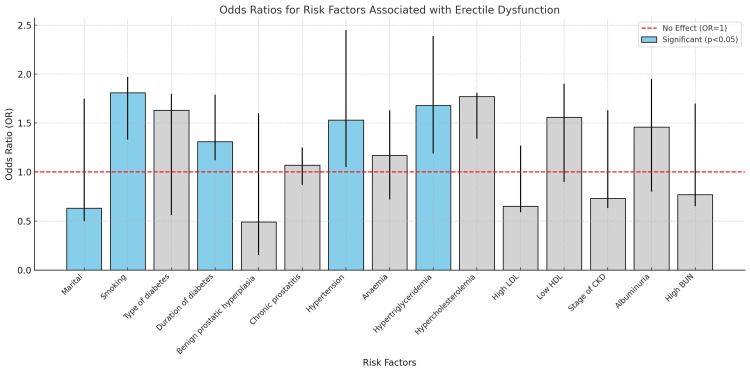 Figure 5
Figure 5| Premature ejaculation (PE) | p-value | ||||
| No PE | Borderline PE | PE | Total | ||
| Age (years) | 44±10 | 39±11 | 43±10 | 43±11 | 0.438 |
| Height (cm) | 158±13 | 156±8 | 161±10 | 159±11 | 0.357 |
| Weight (Kg) | 77±17 | 81±10 | 77±19 | 77±18 | 0.845 |
| BMI (kg/m2) | 31±8 | 33±6 | 30±8 | 31±8 | 0.500 |
| Systolic blood pressure (mmHg) | 125±9 | 123±9 | 124±11 | 124±10 | 0.900 |
| Diastolic blood pressure (mmHg) | 81±14 | 89±9 | 78±12 | 80±13 | 0.01* |
| HBA1c | 6±1 | 6±1 | 6±1 | 6±1 | 0.562 |
| Fasting plasma glucose (mg/dL) | 96±15 | 106±15 | 98±16 | 98±15 | 0.235 |
| Hb level (g/dL) | 12±2 | 11±3 | 12±2 | 12±2 | 0.447 |
| Total cholesterol (mmol/L) | 5.7±2.1 | 6.2±2.3 | 5.8±2 | 5.8±2.1 | 0.852 |
| TG (mmol/L) | 4.3±2 | 5.1±1.8 | 4.4±1.9 | 4.4±1.9 | 0.615 |
| LDL (mmol/L) | 3.3±2 | 3.6±1.7 | 3.4±2.2 | 3.4±2.1 | 0.922 |
| HDL (mmol/L) | 1.33±.8 | 1.46±1.01 | 1.45±.86 | 1.39±.84 | 0.767 |
| Serum creatinine (μmol/L) | 80±25 | 77±29 | 82±22 | 81±23 | 0.873 |
| eGFR (mL/min/1.73 m2) | 92±19 | 91±16 | 92±18 | 92±18 | 0.974 |
|
| 63±36 | 65±38 | 61±36 | 62±36 | 0.921 |
| BUN (mmol/L) | 6±2 | 6±3 | 7±3 | 6±3 | 0.510 |
| Blood uric acid (μmol/L) | 264±67 | 285±58 | 272±71 | 269±68 | 0.687 |
| Premature ejaculation (PE) | Total | p-value | ||||
| No PE | Borderline PE | PE | ||||
| Age group | 20-44 years | 21 (21%) | 4 (4%) | 25 (25%) | 50 (50%) | 0.432 |
| 45-64 years | 25 (25%) | 3 (3%) | 22 (22%) | 50 (50%) | ||
| Marital status | Married | 36 (36%) | 6 (6%) | 40 (40%) | 82 (82%) | 0.668 |
| Smoking status | Non-smoker | 33 (33%) | 5 (5%) | 36 (36%) | 74 (74%) | 0.652 |
| Smoker | 13 (13%) | 2 (2%) | 11 (11%) | 26 (26%) | ||
| BMI category | Underweight | 1 (1%) | 0 (0%) | 1 (1%) | 2 (2%) | 0.472 |
| Normal weight | 9 (9%) | 0 (0%) | 15 (15%) | 24 (24%) | ||
| Overweight | 10 (10%) | 3 (3%) | 11 (11%) | 24 (24%) | ||
| Obese | 26 (26%) | 4 (4%) | 20 (20%) | 50 (50%) | ||
| Type of diabetes | Type 1 diabetes | 9 (9%) | 1 (1%) | 6 (6%) | 16 (16%) | 0.665 |
| Type 2 diabetes | 37 (37%) | 6 (6%) | 41 (41%) | 84 (84%) | ||
| Duration of diabetic illness | Less than 10 years | 18 (18%) | 0 (0%) | 9 (9%) | 27 (27%) | 0.024* |
| More than 10 years | 28 (28%) | 7 (7%) | 38 | 73 (73%) | ||
| Comorbidity | BPH | 8 (8%) | 1 (1%) | 4 (4%) | 13 (13%) | 0.256 |
| Chronic prostatitis | 4 (4%) | 0 (0%) | 5 (5%) | 9 (9%) | 0.786 | |
| Hypertension (DBP≥ 90 mmHg) | 15 (15%) | 4 (4%) | 13 (13%) | 32 (32%) | 0.294 | |
| Anaemia (Hb < 13 g/dL) | 29 (29%) | 5 (5%) | 27 (27%) | 61 (61%) | 0.772 | |
| Hypercholesterolemia (˃ 5.2 mmol/L) | 27 (27%) | 5 (5%) | 30 (30%) | 62 (62%) | 0.762 | |
| Hypertriglyceridemia (TG˃ 1.7 mmol/L) | 40 (40%) | 6 (6%) | 43 (43%) | 89 (89%) | 0.752 | |
| Elevated LDL (≥2.6 mmol/L) | 26 (26%) | 5 (5%) | 31 (31%) | 62 (62%) | 0.559 | |
| Decreased HDL (<1.6 mmol/L) | 28 (28%) | 3 (3%) | 24 (24%) | 55 (55% | 0.509 | |
| Microalbuminuria | 35 (35%) | 5 (5%) | 32 (32%) | 72 (72%) | 0.691 | |
| Elevated BUN | 20 (20%) | 3 (3%) | 24 (24%) | 47 (47%) | 0.745 | |
| Creatinine (65-115 µmol/L) | Normal | 26 (26%) | 3 (3%) | 29 | 58 | 0.909 |
| Elevated | 5 (5%) | 1 (1%) | 5 (5%) | 11 (11%) | ||
| Decreased | 15 (15%) | 3 (3%) | 13 (13%) | 31 (31%) | ||
| Erectile dysfunction | No erectile dysfunction | 6 (6%) | 1 (1%) | 8 (8%) | 15 (15%) | 0.383 |
| Mild erectile dysfunction | 25 (25%) | 3 (3%) | 21 (21%) | 49 (49%) | ||
| Moderate erectile dysfunction | 10 (10%) | 0 (0% | 8 (8%) | 18 (18%) | ||
| Severe erectile dysfunction | 5 (5%) | 3 (3%) | 10 (10%) | 18 (18%) | ||
| eGFR | G1 (normal, no CKD) | 22 (22%) | 4 (4%) | 26 (26%) | 52 (52%) | 0.740 |
| G2 (No CKD) | 24 (24%) | 3 (3%) | 21 (21%) | 48 (48%) | ||
| Total | 46 (46%) | 7 (7%) | 47 (47%) | 100 (100%) | ||
| Risk Factor | RR | OR | 95% CI Lower | 95% CI Upper | p-value |
| Marital status | 0.79 | 0.63 | 0.5 | 1.75 | 0.04* |
| Smoking | 1.89 | 1.81 | 1.33 | 1.97 | 0.04* |
| Type of diabetes | 1.28 | 1.63 | 0.56 | 1.8 | 0.42 |
| Duration of diabetes | 1.58 | 1.31 | 1.12 | 1.79 | 0.01 |
| Benign prostatic hyperplasia | 0.71 | 0.49 | 0.15 | 1.6 | 0.25 |
| Chronic prostatitis | 1.04 | 1.07 | 0.87 | 1.25 | 1 |
| Hypertension | 1.28 | 1.53 | 1.05 | 2.45 | 0.01* |
| Anaemia | 1.09 | 1.17 | 0.72 | 1.63 | 0.84 |
| Hypertriglyceridemia | 1.82 | 1.68 | 1.19 | 2.39 | 0.03* |
| Hypercholesterolemia | 1.87 | 1.77 | 1.34 | 1.73 | 0.54 |
| High LDL | 0.8 | 0.65 | 0.59 | 1.27 | 0.31 |
| Low HDL | 1.27 | 1.56 | 0.9 | 1.9 | 0.32 |
| Stage of CKD | 0.85 | 0.73 | 0.63 | 1.63 | 0.54 |
| Albuminuria | 1.24 | 1.46 | 0.8 | 1.95 | 0.5 |
| High BUN | 0.87 | 0.77 | 0.65 | 1.7 | 0.55 |
| Erectile dysfunction | p-value | ||||
| No erectile dysfunction | Mild erectile dysfunction | Moderate erectile dysfunction | Severe erectile dysfunction | ||
| Age (years) | 45±11 | 43±10 | 42±11 | 42±12 | 0.706 |
| Height (cm) | 160±10 | 159±11 | 159±16 | 160±7 | 0.821 |
| Weight (Kg) | 77±15 | 76±17 | 80±20 | 77±18 | 0.639 |
| BMI (kg/m2) | 30±7 | 31±7 | 32±10 | 30±7 | 0.865 |
| Systolic blood pressure (mmHg) | 126±10 | 125±10 | 120±10 | 125±9 | 0.461 |
| Diastolic blood pressure (mmHg) | 76±13 | 79±14 | 81±13 | 84±10 | 0.305 |
| HBA1c | 6±1 | 6±1 | 6±1 | 6±1 | 0.693 |
| Fasting plasma glucose (mg/dL) | 96±15 | 98±17 | 96±15 | 100±13 | 0.898 |
| Hb level (g/dL) | 12±2 | 12±2 | 13±2 | 11±2 | 0.483 |
| Total cholesterol (mmol/L) | 6±2 | 6±2 | 5±2 | 6±2 | 0.307 |
| TG (mmol/L) | 4.1±1.7 | 4.3±1.9 | 4.4±2.2 | 5.0±2.2 | 0.672 |
| LDL (mmol/L) | 3.0±2.2 | 3.7±2.1 | 4.1±2.1 | 2.7±1.6 | 0.257 |
| HDL (mmol/L) | 1.4±0.9 | 1.3±0.7 | 1.4±0.7 | 1.2±1.0 | 0.633 |
| Serum creatinine (μmol/L) | 76±18 | 77±24 | 89±23 | 85±25 | 0.306 |
| eGFR (mL/min/1.73 m2) | 95±21 | 92±17 | 95±16 | 87±21 | 0.686 |
|
| 50±36 | 66±35 | 68±38 | 55±34 | 0.245 |
| BUN (mmol/L) | 7±2 | 6±3 | 7±3 | 7±2 | 0.265 |
| Blood uric acid (μmol/L) | 272±72 | 273±66 | 257±69 | 266±74 | 0.097 |
| Erectile dysfunction | p-value | |||||
| No erectile dysfunction | Mild erectile dysfunction | Moderate erectile dysfunction | Severe erectile dysfunction | |||
| Age group | 20-44 years | 7 (7%) | 24 (245) | 10 (10%) | 9 (9%) | 0.958 |
| 45-64 years | 8 (8%) | 25 (25%) | 8 (8%) | 9 (9%) | ||
| Marital status | Married | 13 (13%) | 42 (42%) | 13 (13%) | 14 (14%) | 0.560 |
| Smoking status | Non-smoker | 12 (12%) | 37 (37%) | 11 (11%) | 14 (14%) | 0.334 |
| Smoker | 3 (3%) | 12 (12%) | 7 (7%) | 4 (4%) | ||
| BMI category | Underweight | 0 (0%) | 1 (1%) | 1 (1%) | 0 (0%) | 0.930 |
| Normal weight | 4 (4%) | 13 (13%) | 2 (2%) | 5 (5%) | ||
| Overweight | 4 (4%) | 11 (11%) | 5 (5%) | 4 (4%) | ||
| Obese | 7 (7%) | 24 (24%) | 10 (10%) | 9 (9%) | ||
| Type of diabetes | Type 1 diabetes | 3 (3%) | 9 (9%) | 3 (3%) | 1 (1%) | 0.604 |
| Type 2 diabetes | 12 (12%) | 40 (40%) | 15 (15%) | 17 (17%) | ||
| Duration of diabetic illness | Less than 10 years | 6 (6%) | 12 (12%) | 5 (5%) | 4 (4%) | 0.03* |
| More than 10 years | 9 (9%) | 37 (37%) | 13 (13%) | 14 (14%) | ||
| Comorbidity | BPH | 2 (2%) | 7 (7%) | 4 (4%) | 0 (0%) | 0.181 |
| Chronic prostatitis | 3 (3%) | 5 (5%) | 0 (0%) | 1 (1%) | 0.083 | |
| Hypertension (DBP≥ 90 mmHg) | 4 (4%) | 16 (16%) | 4 (4%) | 8 (8%) | 0.517 | |
| Anaemia (Hb < 13 g/dL) | 9 (9%) | 30 (30%) | 10 (10%) | 12 (12%) | 0.924 | |
| Hypercholesterolemia (˃ 5.2 mmol/L) | 10 (10%) | 31 (31%) | 9 (9%) | 12 (12%) | 0.697 | |
| Hypertriglyceridemia (TG˃ 1.7 mmol/L) | 13 (13%) | 44 (44%) | 16 (16%) | 16 (16%) | 0.990 | |
| Elevated LDL (≥2.6 mmol/L) | 7 (7%) | 31 (31%) | 15 (15%) | 9 (9%) | 0.106 | |
| Decreased HDL (<1.6 mmol/L) | 8 (8%) | 25 (25%) | 11 (11%) | 11 (11%) | 0.832 | |
| Microalbuminuria | 8 (8%) | 41 (41%) | 12 (12%) | 11 (11%) | 0.065 | |
| Elevated BUN | 7 (7%) | 18 (18%) | 11 (11%) | 11 (11%) | 0.175 | |
| Creatinine (65-115 µmol/L) | Normal | 10 (10%) | 26 (26%) | 12 (12%) | 10 (10%) | 0.524 |
| Elevated | 0 (0%) | 5 (5%) | 3 (3%) | 3 (3%) | ||
| Decreased | 5 (5%) | 18(18%) | 3 (3%) | 5 (5%) | ||
| eGFR | G1 (normal, no CKD) | 9 (9%) | 25 (25%) | 11 (11%) | 7 (7%) | 0.513 |
| G2 (No CKD) | 6 (6%) | 24 (24%) | 7 (7%) | 11 (11%) | ||
| Total | 15 (15%) | 49 (49%) | 18 (18%) | 18 (18%) | ||
| Risk Factor | RR | OR | 95% CI Lower | 95% CI Upper | p-value |
| Marital | 1.66 | 1.51 | 1.20 | 2.05 | 0.04* |
| Smoking | 1.49 | 1.48 | 1.10 | 1.90 | 0.04* |
| Type of diabetes | 1.50 | 1.39 | 0.64 | 1.89 | 0.70 |
| Duration of diabetes | 3.00 | 2.90 | 1.50 | 3.50 | 0.02* |
| Benign prostatic hyperplasia | 0.97 | 0.97 | 0.49 | 1.87 | 1.00 |
| Chronic prostatitis | 0.40 | 0.30 | 0.17 | 0.84 | 0.13 |
| Hypertension | 2.70 | 2.60 | 1.50 | 2.60 | 0.77 |
| Premature Ejaculation | 2.20 | 2.09 | 1.45 | 2.60 | 0.04* |
| Anaemia | 0.96 | 0.95 | 0.43 | 1.92 | 1.00 |
| Hypertriglyceridemia | 2.55 | 2.50 | 2.15 | 2.97 | 0.03* |
| Hypercholesterolemia | 2.30 | 2.27 | 1.90 | 2.64 | 0.04* |
| High LDL | 1.87 | 1.80 | 1.30 | 2.90 | 0.02* |
| Low HDL | 1.78 | 1.70 | 1.40 | 2.80 | 0.01* |
| Stage of CKD | 1.44 | 1.40 | 0.86 | 1.87 | 0.54 |
| Albuminuria | 0.44 | 0.38 | 0.12 | 1.16 | 0.12 |
| High BUN | 0.99 | 0.98 | 0.33 | 1.36 | 1.00 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSexual function and dysfunction studies · Hormonal and reproductive studies · Urinary Bladder and Prostate Research
Introduction
Diabetes mellitus is a chronic condition with profound systemic implications. Among the complications that affect diabetic patients is sexual dysfunction. Male sexual dysfunction (SD) includes erectile dysfunction (ED), ejaculatory dysfunction, orgasmic dysfunction, and hypoactive sexual desire disorder (HSDD) [1]. ED has the highest morbidity, followed by premature ejaculation (PE) [2]. Disorders such as these are a major cause of deterioration in quality of life and personal relationships and can further exacerbate the psychological and physical load faced by sufferer groups [3]. These conditions are often unrecognised and untreated, though they severely impact both quality of life and psychological well-being [4].
Endothelial dysfunction, which includes lower bioavailability of nitric oxide and poor vasodilation, is a major cause of ED in diabetics. These processes are essential for achieving an erection. Additionally, diabetic neuropathy contributes to sensory deficits and autonomic dysfunction, compounding the difficulty in achieving or maintaining sexual performance [5].
Premature ejaculation (PE) is indeed associated with diabetes, although the relationship is complex and multifaceted. PE is common among many diabetic patients due to autonomic neuropathy, which leads to an overactive sympathetic nervous system [6]. Furthermore, stress and anxiety associated with diabetes elevate the threshold for ejaculation further through more stimulation of the sympathetic system [7]. Diabetes is also known to alter the hormones and thus the normal function during sexual activity. In the end, there is a much higher incidence of PE in diabetic patients who already suffer from erectile dysfunction [8].
The presence of diabetes increases the risk of sexual dysfunction threefold when compared to non-diabetic populations [9]. The prevalence of ED alone in diabetic men ranges from 35% to 75% [10]. Large population-based studies have recognised diabetes as the most important chronic disease associated with ED [11]. According to a meta-analysis of worldwide data from 145 studies representing 88,577 men, the overall estimated prevalence of ED was 52.5% [12]. This was much higher in men with diabetes than in healthy men, with an odds ratio of 3.62 (95% CI, 2.53 to 5.16). Studies using the International Index of Erectile Function-5 (IIEF-5) scale reported a higher prevalence of 82.2% [13].
Male sexual dysfunction also has far-reaching psychosocial implications, negatively impacting marital relationships, self-esteem, and overall quality of life [14]. Despite these severe consequences, many diabetic men do not seek help due to cultural shames or a lack of awareness, particularly in Middle Eastern societies, where discussing sexual health remains a sensitive topic [15]. With a high prevalence of diabetes, Saudi Arabia is giving us an opportunity to study this issue in a unique context. Saudi Arabia has extensively studied the complications of diabetes, such as nephropathy, neuropathy, and retinopathy, but the sexual health of diabetic men remains largely unexplored. The current study aims to fill this gap by assessing the prevalence of ED and PE among diabetic patients in Saudi society and the associated risk factors. Focusing on a Saudi cohort, this research will reveal the specific epidemiological features of sexual dysfunctions in this population and contribute to the design of culturally appropriate and clinically effective management strategies.
Materials and methods
A total of 100 male diabetic patients who visited Dr. Soliman Fakeeh Hospital, Jeddah, Saudi Arabia, between August and December 2024 were recruited for this cross-sectional, non-interventional, observational study. All participants gave informed consent prior to participation. We collected and stored the data in an encrypted file to safeguard the volunteers' identity and privacy. This study received ethical approval in accordance with the principles stated in the Declaration of Helsinki from the Institutional Review Board of Fakeeh College for Medical Sciences (approval number: 506/IRB/2023).
The study included participants who met the following criteria: a confirmed diagnosis of diabetes, an age range between 18 and 60 years, and the provision of written informed consent. We excluded individuals who were not sexually active, had severe conditions such as mental illnesses or physical disabilities that hindered their ability to participate in sexual health assessments, or lacked complete survey data.
Socio-demographic information, including age (years), height (cm), weight (kg), body mass index (BMI) (kg/m2), smoking history, and marital status, was collected through direct interviews. Additionally, medical records provided data on blood pressure, diabetes as the primary diagnosis, and associated comorbidities.
We got glycated hemoglobin (HbA1c), fasting plasma glucose (mg/dL), haemoglobin level (g/dL), total cholesterol (mmol/L), triglyceride (mmol/L), low-density lipoprotein cholesterol (LDL) (mmol/L), high-density lipoprotein cholesterol (HDL) (mmol/L), serum creatinine (µmol/L), estimated glomerular filtration rate (eGFR) (mL/min/1.73 m²), urea nitrogen (BuN) (mmol/L), urinary albumin-to-creatinine ratios (U.ACR) (mg/L), and blood uric acid (BUA) (µmol/L).
We evaluated the subjects' sexual dysfunction using a five-item version of the International Index of Erectile Function (IIEF-5) and the Premature Ejaculation Diagnostic Tool (PEDT). IIEF-5 includes five items that address erectile function and satisfaction with sexual intercourse. Additional analysis of the questionnaire helps to distinguish the presence and severity levels of ED: normal ED (22-25 points), mild ED (12-21 points), moderate ED (8-11 points), and severe ED (1-7 points) [16]. We used PEDT to assess PE. PEDT scores ≥11 indicate PE diagnosis; 9 or 10 refer to probable PE, while ≤ 8 indicates the nonexistence of PE [17]. Simultaneously, we considered PE if a patient's IELT (intravaginal ejaculatory latency time) was less than 3 minutes and they experienced poor sexual satisfaction.
The data were statistically analysed using IBM SPSS Statistics version 26 (IBM Corp., Armonk, NY, USA). We checked the normality of the data at the first stage using the Shapiro-Wilk test. We calculated descriptive statistics to characterise the participants, which included means (M) and standard deviations (SD) for continuous variables and frequencies with percentages for categorical variables. We used relative risks (RR) and odds ratios (OR) with 95% confidence intervals to analyse the association of risk factors for the development of ED and PE. For all tests, a p-value <0.05 was considered statistically significant.
Results
Analysis of findings on premature ejaculation
The prevalence pattern of PE varies among different subgroups within patients with diabetes. PE patients (43±10 years) were comparable in age to patients without PE (44±10 years) and borderline PE (39±11 years). No significant difference in height, weight, and BMI was observed between groups, unlike blood pressure parameters, which were all significantly different between groups, with borderline PE (BP 89±9 mmHg) being higher than the other groups in diastolic BP. There were no significant group differences in HbA1c, fasting plasma glucose, or lipid profiles (cholesterol, triglycerides (TG), or low-density lipoprotein (LDL)). Renal function markers (serum creatinine, eGFR, and urinary albumin to creatinine ratio) were stable between the groups. On the other hand, borderline PE patients showed slightly lower haemoglobin levels (11.3 ± 3 g/dL) (Table 1).
The two age groups, 20-44 years and 45-64 years, had equal distributions of PE. Married status at 40% accounted for most PE cases. Obesity was the most frequent response to BMI categories in PE patients, at 20%; overweight was second at 11%. A minority of PE sufferers were current smokers (9%), while 7% were ex-smokers. Major comorbid conditions are erectile dysfunction (39%); hypertriglyceridemia (43%); hypercholesterolaemia (30%); elevated LDL (31%); and microalbuminuria (32%) (Table 2, Figure 1).
Frequency distributions of comorbidities in PE patientsPE (premature ejaculation), LDL (low-density lipoprotein), HDL (high-density lipoprotein), and BUN (blood urea nitrogen).
Seven percent of the cases were classified as borderline PE, and 47% had PE. Erectile dysfunction was noted in 85% of patients, of whom 49% had mild ED, 18% moderate ED, and 18% severe ED. ED and PE were not present in 15% and 46% of the cases, respectively. ED and PE occurred simultaneously in 39% of the cases. Figure 2 illustrates the frequency of coexistence between ED and PE, showcasing the distribution of PE statuses across different levels of ED severity.
Frequency distribution of erectile dysfunction categories in PE patients PE (premature ejaculation)
Looking at odds ratios (ORs) and relative risks (RRs) for things that are linked to PE gives us important information about how these things are connected to the condition. There were statistically significant links (p < 0.05) between smoking (OR: 1.81, 95% CI: 1.33-1.97), high blood pressure (OR: 1.53, 95% CI: 1.05-2.45), and high triglycerides (OR: 1.68, 95% CI: 1.19-2.39), which suggests that these conditions may make getting PE more likely. The risk of PE was significantly associated with duration of diabetes (OR: 1.31, 95% CI: 1.12-1.79). But benign prostatic hyperplasia (BPH), low HDL, and chronic prostatitis did not have significant associations (p ≥ 0.05), which means they were not linked to PE in the people who were studied (Table 3, Figure 3).
Odds ratio for risk factors associated with premature ejaculation OD (odds ratio), RR (relative risk), CI (confidence interval), LDL (low-density lipoprotein), HDL (high-density lipoprotein), CKD (chronic kidney disease), and BUN (blood urea nitrogen).
Analysis of findings on erectile dysfunction
Severe ED was most frequent among individuals aged 42±12 years. While BMI and systolic blood pressure were similar across groups, diastolic pressure was greatest in severe ED (84±10 mmHg). Metabolic markers such as HbA1c and lipid profiles were identical, but severe ED cases showed mild TG increase (5.0±2.2 mmol/L). There was no significant difference in renal function markers except eGFR levels, which were mildly lower in severe ED (87±21 mL/min/1.73 m2). Severe ED patients had lower haemoglobin levels (11.2±2 g/dL) (Table 4).
The most common form of ED was mild (49%), then moderate and severe ED (18% each). Married individuals made up most patients (42% with mild ED and 149% with severe ED). Obesity was among the most common factors, notably in mild (24%) and severe ED (9%). Hypertriglyceridemia (44%), hypercholesterolaemia (31%), and decreased HDL levels (25%) were prevalent for all ED severity. Microalbuminuria and anaemia were also prevalent in mild (41%) and severe ED (12%); however, moderate ED showed less involvement. Smoking showed a weaker link, as most ED patients were non-smokers (37%) (Table 5, Figure 4).
Frequency distribution of comorbidities in ED patients ED (erectile dysfunction), LDL (low-density lipoprotein), HDL (high-density lipoprotein), and BUN (blood urea nitrogen).
ED was significantly associated with multiple risk factors. Marriage, smoking, hypertension, and long-term diabetes exhibited significant associations with ORs of 1.51, 1.48, 2.60, and 2.90, respectively. Furthermore, erectile dysfunction was significantly associated with elevated cholesterol (OR = 2.50), increased LDL (OR = 1.80), and decreased HDL (OR = 1.70). ED was not significantly predicted by BPH (OR = 0.97), chronic prostatitis (OR = 0.80), or albuminuria (OR = 0.38) (Table 6, Figure 5).
Odds ratio for risk factors associated with erectile dysfunction OD (odds ratio), RR (relative risk), CI (confidence interval), LDL (low-density lipoprotein), HDL (high-density lipoprotein), CKD (chronic kidney disease), and BUN (blood urea nitrogen).
Discussion
The prevalence of ED among male diabetic patients in Saudi Arabia is notably high. 85% of our patients had ED (49% had mild ED, 18% moderate ED, and 18% severe ED). Data from King Khalid University Hospital in Riyadh, which reported 75.2% of diabetic men with ED - 64% partial and 11.2% severe - aligns with these findings [18]. Another Saudi Arabian study found that diabetic men with low testosterone levels had an even higher ED prevalence of 86.7% [19]. A multicenter study in Jeddah revealed that 30% of patients with ED had diabetes [18]. Mild to moderate cases of ED in our study had borderline increases in diastolic blood pressure (84±10 mmHg) and low eGFR values (87±21 mL/min/1.73 m2), which may suggest some vascular and renal changes. Moreover, TG levels had higher values in severe cases of ED (5.0±2.2 mmol/L), suggesting that ED may have a continuum with an apparent role of lipid metabolism in propagation. The level of haemoglobin was the lowest in the severe cases of ED (11±2 g/d/L), indicating that there is a possibility that anaemia is a cause.
Forty-seven percent of our patients had PE, and 7% had borderline PE. The mean ejaculatory latency time was shorter in diabetic patients (3.6±2.7 minutes) compared to non-diabetic individuals (4.3±2.8 minutes) [8]. PE is found to be significantly more prevalent in diabetic patients compared to non-diabetics [8]. Although the search results don't offer precise information about the prevalence of PE in Saudi patients with diabetes, one study reported that PE was present in 75.8% of male Saudi diabetic patients, and another study reported the prevalence to be 83% [8, 20].
We noted the co-occurrence of ED and PE in 39% of our cases (OD = 2.09, CI = 1.45-2.60, p<0.05). A study of diabetic patients in Saudi Arabia found that those with ED showed a significantly higher incidence of PE and shorter ejaculatory latency times [8].
Sixteen percent of our studied patients had type 1 diabetes, while 84% had type 2 diabetes. Both type 1 and type 2 diabetes are associated with an increased risk of sexual dysfunction in men, particularly ED. We observed ED in 49% of patients with type 1 diabetes and 86% of patients with type 2 diabetes. Research indicates that 45.8% of men with both types of diabetes experience ED, which is nearly double the rate in men without diabetes (24.1%) [21]. Some studies have shown that 61.8% of men with type 1 diabetes report poor erectile function [21]. Additionally, other studies suggest that men with type 1 diabetes may have a higher risk of developing ED compared to those with type 2 diabetes [9].
We found that 37% of patients with type 1 diabetes and 81% of patients with type 2 diabetes had PE. Despite not being specific to Saudi Arabia, a study of type 2 male diabetic patients found the prevalence of PE to be 27.5% [22], while another study reported it to be 40.2% [23].
In this study, the results confirm the presence of a strong relationship between some risk factors and the prevalence of ED and PE in the population under review. More specifically, the presence of one or more of these three risk factors was found to predispose ED: marital status, smoking, and duration of diabetes, with ORs of 1.51, 1.48, and 2.90, respectively, all statistically significant at p < 0.05. This indicates that these factors are important contributors to the risk of developing ED. Similarly, smoking, marital contact, and long-standing diabetes were also associated with the occurrence of PE with ORs of 0.63 (p = 0.04), 1.81 (p = 0.04), and 1.31 (p = 0.01), respectively. The higher incidence of such sexual dysfunction among married patients reflects potential psychosocial stressors. While marriage itself is not explicitly identified as a risk factor for sexual dysfunction in diabetic men, the quality of the marital relationship and associated psychosocial factors can significantly influence sexual health outcomes [24]. Sexual function is significantly affected by diabetes duration, particularly when it exceeds 10 years. After more than 10 years of diabetes, 38% of our patients had PE and 64% had ED. After 10 years of having type 2 diabetes, the risk of ED becomes significantly greater compared to men without diabetes [21]. Men with diabetes lasting more than 10 years were 2.7 times more likely to report PE compared to those with diabetes for less than 5 years [23].
Also, other conditions such as hypertension (OR = 2.60, p< 0.05) were reported to have a strong relationship with ED, which underscores the need to control cardiovascular comorbidities in order to reduce sexual dysfunction.
According to our study, the proportion of patients with elevated triglycerides was 76% among those with ED and 43% among those with PE, with odds ratios of 2.5 and 1.68, respectively, indicating a significant relationship (p < 0.05). Furthermore, our studies revealed that there were also important relationships between ED and hypercholesterolaemia (OR = 2.50, p < 0.05), elevated LDL cholesterol levels (OR = 1.80, p < 0.05), and low HDL cholesterol levels (OR = 1.70, p < 0.05). Diabetic patients frequently have a specific lipid abnormality known as diabetic dyslipidaemia, which is characterised by elevated levels of TG, decreased levels of HDL, and elevated levels of LDL [25]. This dyslipidaemia is associated with an increased risk of future cardiovascular disease and an increase in the severity of one’s sexual dysfunction [25]. Studies have shown that hyperlipidaemia affects the smooth muscle and endothelium cells within the penis, resulting in impaired erectile function [26]. Besides, increased levels of LDL have been associated with arteriogenic ED. Research has shown that 2.41 mmol/L of LDL levels is a determinant in over 55.2% and up to 76.7% of cases of arteriogenic ED [27]. Lastly, the presence of HDL at low levels among diabetic patients may precipitate ED. Higher HDL levels may help protect against arteriogenic ED because there is a positive relationship between HDL levels and peak systolic velocity in penile arteries [27].
On the contrary, in our study, BPH (OR = 0.97, p = 1.00), chronic prostatitis (OR = 0.80, p > 0.05), and albuminuria (OR = 0.38, p > 0.05) were found to have weak associations with ED. In addition, these variables - BPH (OR = 0.49, p = 0.25), chronic prostatitis (OR = 1.07, p = 1.00), and albuminuria (OR = 1.46, p = 0.50) - were also shown to be statistically insignificant in predicting PE. Based on these findings, it can be inferred that these variables are not important in predicting either ED or PE attacks.
Adding to this, renal markers such as serum creatinine, eGFR, and urinary albumin-to-creatinine ratios were consistent throughout the groups, excluding the role of significant renal dysfunction in the prevalence of PE or ED. However, borderline PE patients showed slightly lower haemoglobin levels (11±3 g/dL), suggesting anaemia could be a mildly influential factor.
Limitations
The cross-sectional design limits causal inference. Additionally, the sample size of 100 participants restricts the generalisability of the findings. Future studies with larger, longitudinal designs are needed to confirm these associations and explore underlying mechanisms.
Conclusions
The increased incidences of ED and PE emphasise the importance of a proper diagnostic approach. An important step would be the approaches to quitting smoking, controlling blood sugar levels, managing lifestyle habits, and regulating lipids. Screening for sexual dysfunctions and assessment of lipid profiles should be part of the diabetes management in order to enhance the life of the patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Definitions of sexual dysfunctions in women and men: a consensus statement from the Fourth International Consultation on Sexual Medicine 2015 J Sex Med Mc Cabe MP Sharlip ID Atalla E 1351431320162695382810.1016/j.jsxm.2015.12.019 · doi ↗ · pubmed ↗
- 2Erectile dysfunction and premature ejaculation are the most frequently self-reported sexual concerns: profiles of 9,536 men calling a helpline Eur Urol Papaharitou S Athanasiadis L Nakopoulou E 5575634920061638741310.1016/j.eururo.2005.09.023 · doi ↗ · pubmed ↗
- 3Evaluation of sexual dysfunction in males with diabetes Sexuality and Disability Yıldız H BölüktaşRP 187205332015 https://acikerisim.uludag.edu.tr/entities/publication/274887 a 6-0c 14-4125-b 801-307291 cb 8273
- 4The relationship of childhood trauma, anxiety, and sexual satisfaction in Turkish men with erectile dysfunction Dusunen Adam Kutlubay S Safak Y Burhan HŞ 155163372024
- 5Endocrine-related sexual dysfunction in young people Paediatric Endocrinology: Management of Endocrine Disorders in Children and Adolescents Talaulikar V Sangster P Cham Springer 2024 https://link.springer.com/referenceworkentry/10.1007/978-3-030-23709-7_15
- 6Ejaculatory dysfunction in men with diabetes mellitus World J Diabetes Mostafa T Abdel-Hamid IA 9549741220213432694810.4239/wjd.v 12.i 7.954PMC 8311479 · doi ↗ · pubmed ↗
- 7The pathophysiology of acquired premature ejaculation Transl Androl Urol Mc Mahon CG Jannini EA Serefoglu EC Hellstrom WJ 434449520162765221610.21037/tau.2016.07.06PMC 5001985 · doi ↗ · pubmed ↗
- 8Premature ejaculation in type II diabetes mellitus patients: association with glycemic control Transl Androl Urol Majzoub A Arafa M Al-Said S Dabbous Z Aboulsoud S Khalafalla K Elbardisi H 248254520162714145410.21037/tau.2016.03.11PMC 4837318 · doi ↗ · pubmed ↗