An App-Based WHO Mental Health Guide for Depression Detection: A Cluster Randomized Clinical Trial
Brandon A. Kohrt, Akin Ojagbemi, Nagendra P. Luitel, Ioannis Bakolis, Toyin Bello, Paul McCrone, Tatiana Taylor Salisbury, Mark J. D. Jordans, Nicole Votruba, Kenneth Carswell, Eric Green, Evdoxia Gkaintatzi, Bishnu Lamichhane, Olufisayo Elugbadebo, Lola Kola, Heidi Lempp

TL;DR
A study tested a WHO mental health app in Nepal and Nigeria to detect depression, finding it worked well in Nigeria but not in Nepal.
Contribution
The study highlights the importance of testing digital health tools in multiple settings to ensure effectiveness and adoption.
Findings
In Nigeria, the app detected 88% of depression cases compared to 33% with the standard guide.
The app was rarely used in Nepal, leading to poor depression detection rates.
Cost per detected case was significantly lower in Nigeria using the app.
Abstract
What is the feasibility of using the World Health Organization’s mobile app version of the Mental Health Gap Action Programme–Intervention Guide (e-mhGAP-IG) to improve detection of depression? This cluster randomized clinical trial of 35 primary care facilities in Nepal and Nigeria found that in Nepal, the app was used rarely, and depression detection was poor for the standard mhGAP-IG and the e-mhGAP-IG. In Nigeria, the app was commonly used, with 88% of depression cases detected in the group using the e-mhGAP-IG compared with 33% of cases using the standard mhGAP-IG. This study demonstrated the need for feasibility testing of new technologies in multiple settings because adoption may vary and uptake cannot be generalized from a single context. Depression detection in primary care remains limited in low- and middle-income countries despite increasing use of the World Health…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
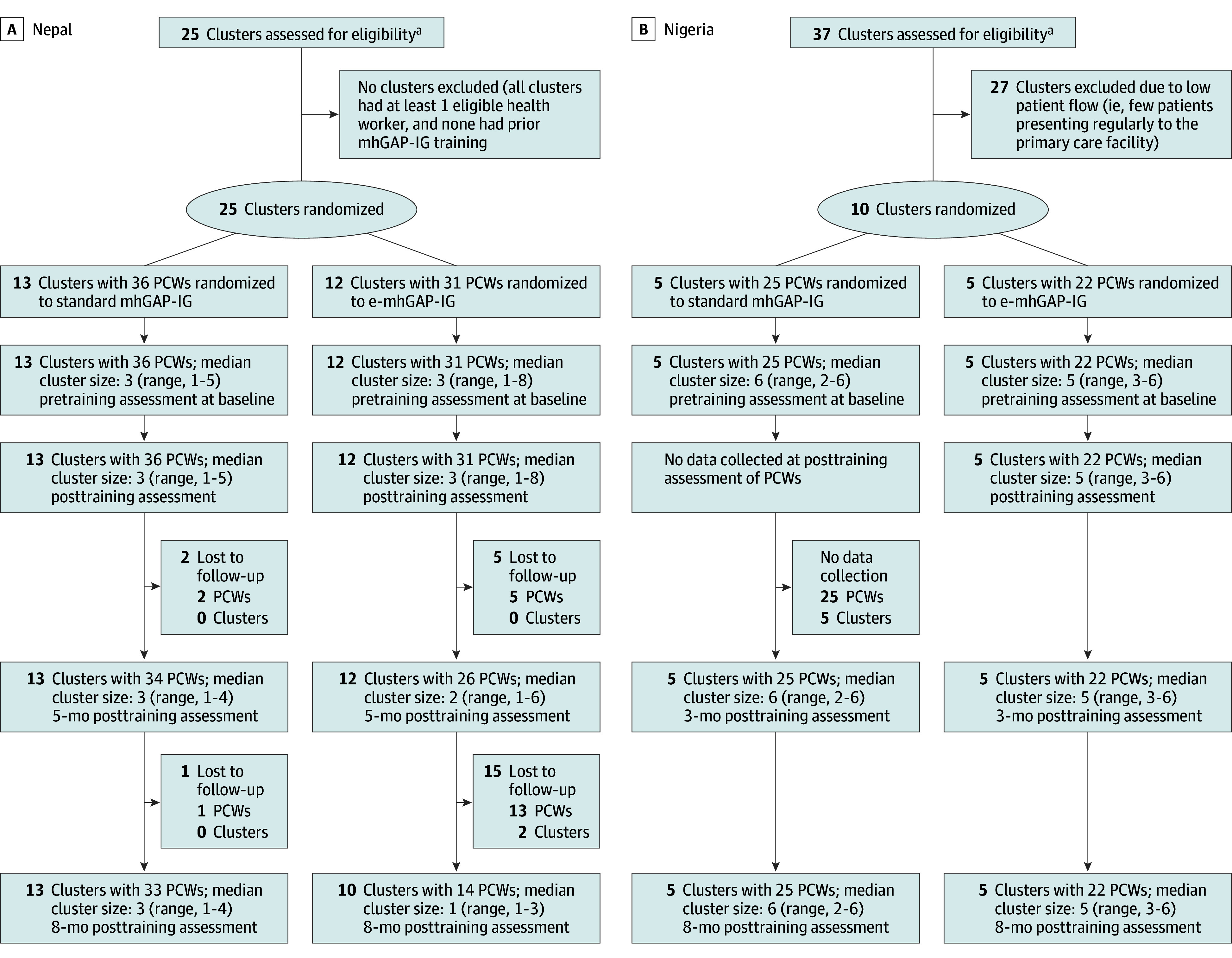 Figure 1
Figure 1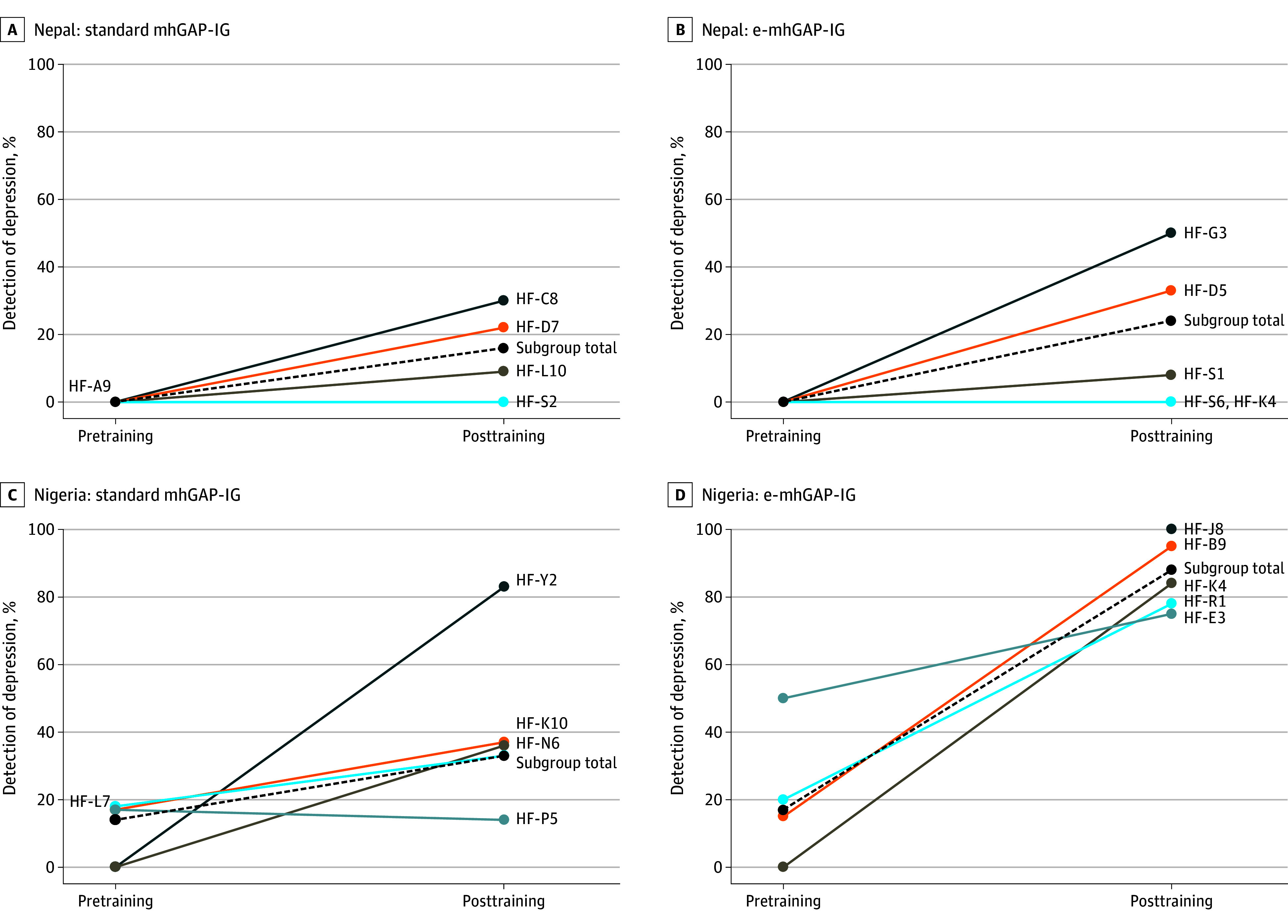 Figure 2
Figure 2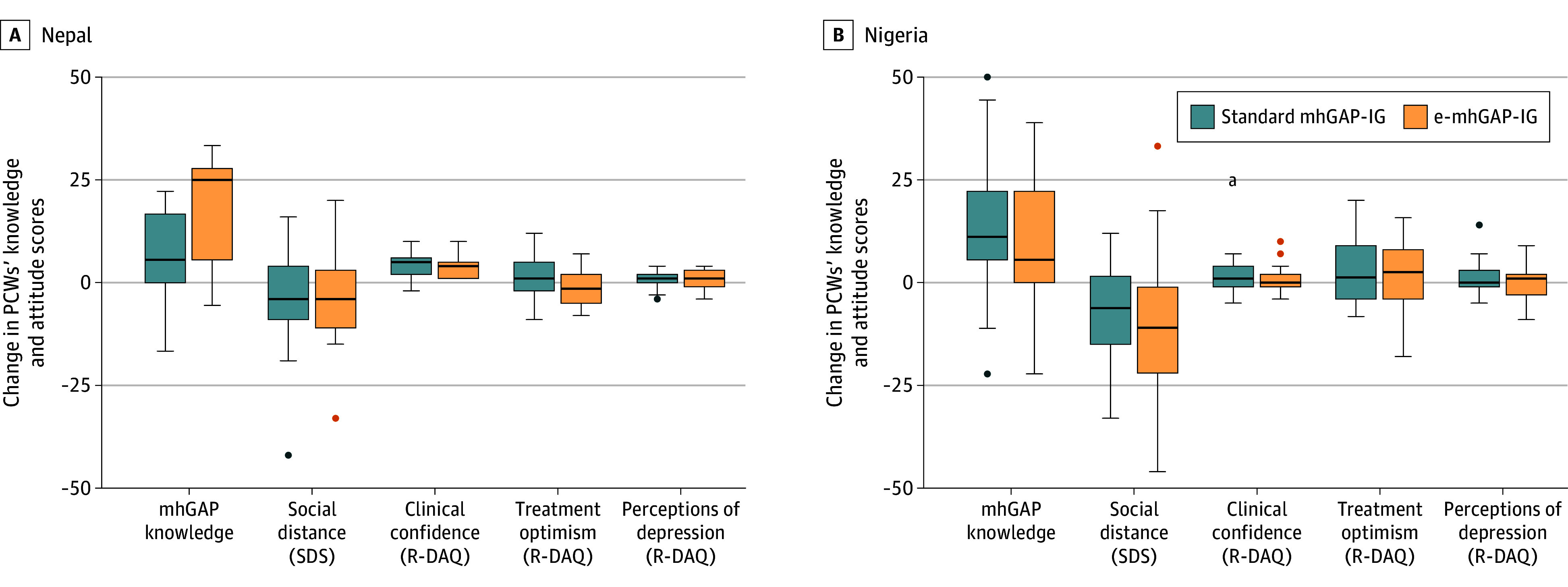 Figure 3
Figure 3| Characteristic | No. (%) | |||
|---|---|---|---|---|
| Nepal (n = 67) | Nigeria (n = 47) | |||
| Standard mhGAP-IG (n = 36) | e-mhGAP-IG (n = 31) | Standard mhGAP-IG (n = 25) | e-mhGAP-IG (n = 22) | |
| Gender | ||||
| Female | 8 (22.2) | 7 (22.6) | 24 (96.0) | 20 (90.9) |
| Male | 28 (77.8) | 24 (77.4) | 1 (4.0) | 2 (9.1) |
| Age, y | ||||
| 21-35 | 25 (69.4) | 16 (51.6) | 0 | 1 (4.5) |
| 36-50 | 8 (22.2) | 13 (41.9) | 13 (52.0) | 14 (63.6) |
| ≥51 | 3 (8.3) | 2 (6.5) | 12 (48.0) | 7 (31.8) |
| Academic qualification | ||||
| Diploma (2 y after secondary school) | 14 (38.9) | 13 (41.9) | 15 (60.0) | 9 (40.9) |
| Bachelor’s degree | 14 (38.9) | 8 (25.8) | 9 (36.0) | 10 (45.5) |
| Master’s degree | 3 (8.3) | 5 (16.1) | 1 (4.0) | 0 |
| Other (eg, medical degree) | 5 (13.9) | 5 (16.1) | 0 | 3 (13.6) |
| Years working in health care | ||||
| <1 | 3 (8.3) | 0 | 0 | 0 |
| 1-5 | 11 (30.6) | 8 (25.8) | 0 | 0 |
| 6-10 | 11 (30.6) | 8 (25.8) | 1 (4.0) | 1 (4.5) |
| >10 | 11 (30.6) | 15 (48.4) | 24 (96.0) | 21(95.5) |
| Prior mental health training | ||||
| No | 35 (97.2) | 29 (93.5) | 0 | 0 |
| Yes | 1 (2.8) | 2 (6.5) | 25 (100.0) | 22 (100.0) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDigital Mental Health Interventions · Mental Health Treatment and Access · COVID-19 and Mental Health
Introduction
The World Health Organization (WHO) Comprehensive Mental Health Action Plan’s goals for 2030 include delivery of mental health services in primary care in 80% of countries and a 50% increase in service coverage for depression.^1^ One tool to achieve this is the Mental Health Gap Action Programme–Intervention Guide (mhGAP-IG), a training and implementation resource for diagnosis and management of mental health conditions in primary care.^2,3^ The mhGAP-IG is used in more than 90 countries.^4^ However, most primary care workers (PCWs) fail to diagnose depression among their patients; a systematic review found that fewer than 1 in 10 patients with depression are detected in primary care facilities in low- and middle-income countries.^5^
Given the increasing availability of mobile technology to enhance health care,^6,7^ a strategy to improve use of the mhGAP-IG is WHO’s development of an app for use during patient encounters as a decision aid for diagnosing and managing depression and other conditions. This Android-based interactive digital version of mhGAP-IG (e-mhGAP-IG)^8^ has functionality for PCWs to enter patient symptoms and other health information to guide diagnosis and treatment.
The e-mhGAP-IG has potential to improve detection of depression. However, the added investment to implement the app (eg, digital technology infrastructure, training, and supervision) would need to be justified by a clinically relevant level of increased detection. Therefore, a feasibility cluster randomized clinical trial (cRCT) was conducted in Nepal and Nigeria with the goal of determining the potential benefit, app use, and associated costs for improving detection of depression, as well as the feasibility of a future fully powered trial evaluating the e-mhGAP-IG. The study outcomes will provide policymakers, clinicians, and health care managers with crucial information to make informed decisions about implementing the e-mhGAP-IG in their settings.
Methods
Design
The full study protocol for this feasibility cRCT has been published^9^ (study protocol in Supplement 1). The current analysis focuses on (1) patient detection outcomes, including e-mhGAP-IG use and cost; (2) PCWs’ depression knowledge, attitudes, and competency for diagnosing and treating depression; and (3) benchmarks for progression to a fully powered trial. Our trial documentation follows the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline, including extensions for pilot and feasibility trials^10^ and cluster trials.^11^ Approval was provided by the Nepal Health Research Council, University of Ibadan/University College Hospital Joint Ethics Committee in Nigeria, King’s College London Research Ethics Committee, and WHO Ethics Review Committee. All PCWs and patients provided written informed consent.
Setting
The feasibility cRCT was undertaken in 4 phases in Jhapa, Nepal, and Ibadan, Nigeria (eFigure 1 in Supplement 2). Nepal and Nigeria were selected because they were sites of prior studies that evaluated the introduction of mental health services into primary care.^12,13^ Primary care facilities in Jhapa were eligible to participate if they did not have mhGAP-IG training in the prior 24 months. Transcultural Psychosocial Organization Nepal implemented the study. In Nigeria, all regional health facilities in Ibadan were eligible to participate. The study was implemented by the University of Ibadan’s department of psychiatry. In both countries, the primary care services were delivered in government facilities. The trial was conducted in Nepal from February 14, 2021, to March 25, 2022, and in Nigeria from September 1, 2021, to January 31, 2022.
Participants
Primary Care Workers
Within primary care facilities, all PCWs who had prescribing privileges, including PCWs who had prior mental health training, were eligible for mhGAP-IG training. Educational level, years of clinical service, and prior experience delivering mental health care were documented for all participating PCWs.
Patients
Patients were recruited in 2 phases: the pretraining phase (for 30 days prior to the PCW mhGAP training) and the patient detection phase (conducted for 90 days during months 5-8 after training). Any patient older than 18 years presenting to the primary care facility who did not have an emergency medical need was eligible.
Interventions
Training duration in the standard mhGAP-IG arm vs the e-mhGAP-IG arm was time matched, with curricula in both arms lasting 6 days in Nepal and 5 days in Nigeria following existing training practices in the countries. The mhGAP-IG modules for depression, psychosis, alcohol use disorder, and suicide prevention were included in the training. For the e-mhGAP-IG, trainees were given smartphones and introduced to the mobile app on the first day of training in Nepal and on the second day of training in Nigeria. In Nepal, a refresher training on the app was held at 5 months, immediately before the patient detection phase.
Prior to this feasibility study, human-centered design was used in Nepal and Nigeria to refine the e-mhGAP-IG app.^8^ This process resulted in an app with the mhGAP-IG master chart for different conditions, interactive symptom assessment, prompted probing for suicide risk and special populations, and treatment guidance (eFigure 2 in Supplement 2). The app was used on Android phones or tablets. A dashboard that contained information submitted by PCWs through e-mhGAP-IG was available for supervisors.
Outcomes
Patient Outcome
The main patient outcome was accuracy of depression diagnosis, operationalized as the percentage of patients with a 9-item Patient Health Questionnaire (PHQ-9)^14^ score of 10 or more who received a depression diagnosis by a PCW. The PHQ-9 had previously been culturally adapted in Nepali language and clinically validated with primary care patients in southern Nepal; this Nepali PHQ-9 yielded a sensitivity of 94% and specificity of 80% for scores of 10 or more when compared with a structured clinical interview using the Composite International Diagnostic Interview.^15^ In Nigeria, a prior validation study with university students yielded a PHQ-9 score of 10 or more with a sensitivity of 85% and specificity of 99% when compared with the Mini International Neuropsychiatric Interview.^16^
PCW Outcomes
Primary care workers’ knowledge was assessed with the mhGAP-IG knowledge assessment tool.^17,18,19^ Attitudes were assessed with the Social Distance Scale (SDS)^20^ and the Revised–Depression Attitudes Questionnaire (R-DAQ).^21^ Competency was evaluated with the WHO-UNICEF (United Nations Children’s Fund) Ensuring Quality in Psychosocial and Mental Health Care competency platform using standardized role plays with the Enhancing Assessment of Common Therapeutic Factors (ENACT) tool^22,23^ (see the eMethods in Supplement 2 for additional information).
Randomization and Sample Size
Randomization was conducted at the level of the primary care facility. Following best practices for feasibility studies,^24^ there was no between-arm inference testing (ie, no comparison between the standard mhGAP-IG and e-mhGAP-IG arms). Instead, before vs after changes were compared separately within each arm by country. Intraclass correlation coefficients (ICCs) were calculated for baseline measures to estimate variance attributable to clustering. Primary care worker outcomes were visualized using box and whisker plots because of the small sample sizes.
Health Economic Analyses
In this feasibility exercise, we did not conduct a full economic evaluation. We limited our analyses to estimating the extra cost of the e-mhGAP-IG compared with the mhGAP-IG. We excluded costs of developing the e-mhGAP-IG app. We estimated the cost per patient with depression detected using the standard mhGAP-IG and the extra cost incurred per patient with depression detected when using the e-mhGAP-IG app (the eMethods in Supplement 2 provides additional information on economic analyses).
Progression to Full Trial
Consistent with best practices in feasibility trials,^25,26^ we established a priori benchmarks for progression to a full trial, as outlined in the study protocol.^9^ The cutoff for PCW retention was completion of all data collection points by at least 67% of PCWs per country. The cutoff for data missingness was no more than 15% per country. The criterion for adverse events was fewer than 10% of patients per country.
Statistical Analysis
Statistical analysis was conducted using SPSS, version 28 (IBM Corp)^27^ from July 20, 2022, through September 27, 2024. Analysis was performed on an intention-to-treat basis. Following best practices in pilot and feasibility studies, no between-arm hypothesis testing was conducted. For within-arm tests for sensitivity to change, 2-sided tests with P < .05 considered significant were used. Generalized estimating equations were used to evaluate within-arm changes in PCW outcomes (knowledge, attitudes, and competency). For depression detection, the outcome was dichotomous (depression detected vs not detected) for each patient with a PHQ-9 score of 10 or more (eMethods in Supplement 2 provides additional information on randomization and sample size calculation for within-arm testing).
Results
Cluster and Participant Characteristics
There were 25 eligible clusters (primary care facilities) in Nepal (Figure 1A). All 25 facilities (67 PCWs; mean [SD] age, 35.3 [9.2] years; 52 men [78%] and 15 women [22%]) were included in the PCW study; 13 primary care facilities were randomized to the standard mhGAP-IG training arm (36 PCWs: 28 men and 8 women), and 12 were randomized to the e-mhGAP-IG arm (31 PCWs: 24 men and 7 women) (Table). Ten of the 25 facilities were included in the patient detection component: 5 facilities from the standard mhGAP-IG arm and 5 facilities from the e-mhGAP-IG arm. In Nigeria, 37 clusters were eligible (Figure 1B), of which 10 facilities (47 PCWs; mean [SD] age, 46.9 [7.5] years; 44 women [94%] and 3 men [6%]) were selected for use in both the PCW and patient detection components: 5 facilities randomized to each arm (standard mhGAP-IG arm, 25 PCWs [24 women and 1 man]; e-mhGAP-IG arm, 22 PCWs [20 women and 2 men]). The Table provides the demographic characteristics of PCWs in the study (see also the eResults in Supplement 2).
CONSORT FlowchartCONSORT flow diagram for participants in (A) Nepal and (B) Nigeria. e-mhGAP-IG indicates mobile app version of the Mental Health Gap Action Programme–Intervention Guide; mhGAP-IG, Mental Health Gap Action Programme–Intervention Guide; and PCW, primary care worker.aClusters defined as primary health care facilities.
In the standard mhGAP-IG arm in Nepal, 246 patients (mean [SD] age, 51 [17.7] years; 131 women [53%] and 115 men [47%]) presented to the primary care facilities during the 1-month pretraining depression detection phase, and 743 patients (mean [SD] age, 48 [16.6] years; 469 women [63%] and 274 men [37%]) presented during the detection phase at 5 to 8 months after training. In the e-mhGAP-IG arm in Nepal, 292 patients (mean [SD] age, 47 [16.5] years; 184 women [63%] and 108 men [37%]) presented during the pretraining detection phase, and 616 patients (mean [SD] age, 49 [17.4] years; 413 women [67%] and 203 men [33%]) presented during the posttraining detection phase. In the standard mhGAP-IG arm in Nigeria, 419 patients (mean [SD] age, 33 [12.4] years; 381 women [91%] and 38 men [9%]) presented during the pretraining detection phase, and 917 patients (864 women, 50 men, and 3 did not report gender; mean [SD] age, 32 [10.5] years; 864 women [94%] and 50 men [6%]) presented during the posttraining detection phase. In the Nigerian e-mhGAP-IG arm, 446 patients (mean [SD] age, 31 [10.9] years; 414 women [93%] and 32 men [7%]) presented during the pretraining detection phase, and 1077 patients (mean [SD] age, 33 [12.8] years; 978 women [91%] and 97 men [9%]) presented during the posttraining detection phase.
Detection of Depression in Primary Care
During the 1-month pretraining phase in Nepal, none of the patients with PHQ-9 scores of 10 or more received a diagnosis of depression by PCWs in either study arm (ie, 0% detection) (Figure 2; eFigure 3 and eTable 1 in Supplement 2). During the pretraining phase in Nigeria, 5 of 36 patients with PHQ-9 scores of 10 or more received a diagnosis of depression by PCWs in mhGAP-IG arm facilities, and 6 of 35 patients in the e-mhGAP-IG arm received a diagnosis of depression.
Changes in Detection of Depression Between Pretraining and Posttraining by Country, Study Arm, and Health Facility Percentage detection is based on the number of patients with a 9-item Patient Health Questionnaire (PHQ-9) score of 10 or more who received a diagnosis of depression by the primary care worker. The pretraining detection period was for 1 month prior to training. The posttraining percentage detection period was from 5 to 8 months after the Mental Health Gap Action Programme–Intervention Guide (mhGAP-IG) training. See eFigure 3 in Supplement 2 for additional details on the number of patients presenting per facility, the number of patients with PHQ-9 scores of 10 or more, and rate of app use per facility. e-mhGAP-IG indicates app version of the Mental Health Gap Action Programme–Intervention Guide; HF, health facility code.
During the posttraining patient detection phase in Nepal, PCWs’ diagnoses of patients with depression in the standard mhGAP-IG arm increased from 0 of 43 patients before training to 15 of 92 patients after training (adjusted mean change [AMC], 16% [95% CI, 5%-28%]), and in the e-mhGAP-IG arm, detection increased from 0 of 49 patients before training to 22 of 91 patients after training (AMC, 24% [95% CI, 12%-36%]) (Figure 2; eFigure 3 and eTable 1 in Supplement 2). There was substantial variability across primary care facilities in the e-mhGAP-IG arm in Nepal (ICC, 0.24) compared with an ICC of 0.07 for standard mhGAP-IG facilities.
In Nigeria, detection of depression in the standard mhGAP-IG arm increased from 5 of 36 patients before training to 25 of 75 patients after training (AMC, 19% [95% CI, 2%-37%]) and in the e-mhGAP-IG arm, detection increased from 6 of 35 patients before training to 67 of 76 patients after training (AMC, 71% [95% CI, 57%-85%]) (Figure 2; eFigure 3 and eTable 1 in Supplement 2). With the standard mhGAP-IG, there were not statistically significantly greater odds (odds ratio, 1.13 [95% CI, 0.21-2.05]) of identifying depression after the training compared with detection prior to training. With the e-mhGAP-IG, there were greater odds (odds ratio, 3.58 [95% CI, 2.58-4.59]) of identifying depression after the training compared with before the training. The ICC was 0.14 among standard mhGAP-IG facilities and 0.02 among e-mhGAP-IG facilities.
In Nepal, 14% of depression diagnoses (6 of 43) by PCWs were individuals whose PHQ-9 score was below the cutoff of 10 or more. However, in Nigeria, of 2637 patients scoring below the PHQ-9 score cutoff of 10 or more, none were identified as having depression.
Use of the e-mhGAP-IG App
In Nepal, the e-mhGAP-IG app was used for 59 of the 616 patients (10%) presenting to the facilities during the patient detection phase (eFigure 4 in Supplement 2). In Nigeria, the app was used for 883 of the 1077 patients (82%). In Nepal, 10 of 15 PCWs never used the app for a patient assessment. The PCWs at the e-mhGAP-IG health facility with the highest detection rate in Nepal never used the app for patient assessments (Health Facility-G3, with depression detected among 18 of 36 patients) (eFigure 3 in Supplement 2). In Nigeria, only 2 of 24 PCWs never used the app for assessments.
PCWs’ Knowledge, Attitudes, and Competence
Knowledge of depression increased within arms in all groups (Figure 3; eFigure 5 and eTable 2 in Supplement 2). The change in the SDS score was not significant in either Nepal group but was significant for a reduced SDS score (lower stigma) within both arms in Nigeria. For the R-DAQ, clinical confidence in treating depression improved in both Nepal groups but not in either Nigeria group. Therapeutic optimism (eg, depression improves with treatment) and general perspectives about depression did not show improvement in either country. For clinical competency, both groups in Nepal showed within-arm improvement on the ENACT tool (improved helping skills and reduced harmful behaviors). Clinical competency was not assessed at baseline in Nigeria; therefore, changes could not be evaluated.
Changes Within Study Arm of Primary Care Worker (PCW) Knowledge and AttitudesMedian change and IQR (error bars) for change from before training to 8-month posttraining follow-up assessment. The PCW sample size with data available before training and at 8-month follow-up assessment: Nepal standard mhGAP-IG, 33 PCWs; Nepal e-mhGAP-IG, 14 PCWs; Nigeria standard mhGAP-IG, 25 PCWs; Nigeria e-mhGAP-IG, 22 PCWs. e-mhGAP-IG indicates mobile app version of the Mental Health Gap Action Programme–Intervention Guide; mhGAP-IG, Mental Health Gap Action Programme–Intervention Guide; R-DAQ, Revised–Depression Attitudes Questionnaire; and SDS, Social Distance Scale.aExtreme outlier.
Economic Evaluation
In Nepal, total training costs for both the e-mhGAP-IG and the mhGAP-IG was Nepali Rupiya (NPR) 534 000 (USD 14.79) for the e-mhGAP-IG and NPR 2798 ($20.90) for the mhGAP-IG.
In Nigeria, total training costs were naira (₦) 2 480 396 (750) for standard mhGAP-IG. The mean administration time was 10 minutes for the e-mhGAP-IG and 3 minutes for the mhGAP-IG. The cost per patient detected with depression was ₦1462 (0.71) for the standard mhGAP-IG (see the eResults in Supplement 2 for additional details on economic outcomes).
Progression to Full Trial
With the predetermined cutoff for progression of 67% retention, Nepal met the threshold with 46 of 67 PCWs (69%) completing all 4 assessments. Only 22 of 47 PCWs (47%) in Nigeria completed all 4 assessments. For data missingness, the cutoff was less than 15%. Nepal met the threshold with 10% data missingness (16 092 of 17 956 responses). Nigeria did not, with data missingness at 27% (9171 of 12 596 responses). Both countries were below the cutoff of 10% adverse events among patients. In Nepal, 5 of 1897 patients (0.3%) in the study had suicidality, and in Nigeria, 7 of 2859 patients (0.2%) had suicidality.
Discussion
This feasibility cRCT sheds light on the potential benefits and challenges of implementing a mobile app version of the mhGAP-IG for use by PCWs to integrate mental health services in primary care. In Nepal, the e-mhGAP-IG was used with only 1 of 10 primary care patients, and both the standard mhGAP-IG and e-mhGAP-IG demonstrated an improvement of only 2 of 10 additional patients with depression detected after training. In Nepal, the PCWs at the facility with the highest depression detection rates did not use the e-mhGAP-IG. In contrast, PCWs in Nigeria used the e-mhGAP-IG with 8 of 10 primary care patients. The PCWs using the e-mhGAP-IG in Nigeria showed improvement, reaching a detection rate of 9 of 10 patients with depression, whereas PCWs using the standard mhGAP-IG detected 3 of 10 primary care patients with depression.
Qualitative research was conducted in both sites as part of the pilot.^28,29^ The qualitative data revealed that in Nigeria, the PCWs were accustomed to using apps on mobile devices for a range of health care services. Apps have been used to provide clinical support information and for documentation (eg, vaccination records). Based on prior experiences with mobile technologies, they reported the e-mhGAP-IG was easy to use. Moreover, the health system enforced the use of health care apps; for example, PCWs were required to keep their mobile phones on at all times and ensure device batteries were charged. Nigerian PCWs also said that using apps in front of patients looked professional, whereas flipping through paper resources looked unprofessional. In Nepal, PCWs reported unfamiliarity with health care apps, and electricity was not available consistently to charge their mobile phones. Familiarity with technology and facility electrical infrastructure likely played a role in country differences in app use. Primary care workers in Nigeria also used the app faster (10 minutes for an e-mhGAP-IG consultation in Nigeria compared with 30 minutes in Nepal). Another difference between countries was prior experience with mental health care; all of the PCWs in Nigeria had prior mental health care experience compared with only 3 of 67 PCWs in Nepal.
Strengths and Limitations
This study has some strengths; a major strength is the multisite implementation strategy.^30,31^ This study also has some limitations. One methodological limitation was the use of the PHQ-9 to judge the accuracy of diagnosis. The PHQ-9 has high rates of false positives.^32^ Therefore, some individuals with elevated PHQ-9 scores in Nepal and Nigeria may not have met the clinical criteria for depression. For example, a cross-sectional study found that among 1897 primary care patients in Nepal, the prevalence of depression was 15% using a PHQ-9 score cutoff of 10 or more compared with only 6% using the PHQ-9 algorithm for a major depressive episode^33^; this finding suggests that many patients with a PHQ-9 score of 10 or more do not have actual clinical cases of depression. The PHQ-9 also has sensitivity limitations; sensitivity was 94% in Nepal and 85% in Nigeria,^15,16^ suggesting that the PHQ-9 misses some patients with major depressive episodes (ie, false negatives). Although there were some patients who received a diagnosis of depression who scored below the PHQ-9 cutoff, in Nigeria there were no diagnoses of depression made among the 2637 patients who scored below the PHQ-9 cutoff. This highlights a risk of reductionism; the e-mhGAP-IG may oversimplify the depression diagnosis to the administration of the PHQ-9. If a full trial were to be conducted evaluating e-mhGAP-IG, a structured clinical interview (eg, Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders) could be more accurate than using PHQ-9 as the clinical reference.^34^
Regarding progression to a full trial, Nepal met targets, but in Nigeria, 1 of the 4 assessments in the standard mhGAP-IG arm was not completed, and competency evaluations were not completed at baseline. This was partly due to research procedures being disrupted during the COVID-19 pandemic. If proceeding to a full trial, it would help to develop mechanisms to ensure completion at all study time points of all measures.
Conclusions
This feasibility cRCT of the e-mhGAP-IG app in Nepal and Nigeria provides valuable insights into the potential of digital tools to enhance depression detection in primary care in low- and middle-income countries. Evaluating new interventions and implementation strategies in multiple sites is recommended for global mental health studies given differences in culture, health systems, technological literacy, and help-seeking for mental health conditions.^30,31^ If this study had been conducted only at 1 site, the feasibility and potential benefit of the e-mhGAP would have been overestimated or underestimated, and the major influence of context on implementation would not have been evident.^30^ As primary care services strive to meet 2030 WHO mental health targets, thoughtful evaluation of digital tools, such as the e-mhGAP-IG, combined with robust training and supervision and a supportive technological infrastructure can play a crucial role in expanding access to quality mental health services worldwide.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Comprehensive Mental Health Action Plan 2013-2030. Document No. 9240031022. World Health Organization; 2021.
- 2World Health Organization. mh GAP Intervention Guide for Mental, Neurological and Substance Use Disorders in Non-Specialized Health Settings. Version 2.0. World Health Organization; 2016.27786430 · pubmed ↗
- 3Brohan E, Chowdhary N, Dua T, Barbui C, Thornicroft G, Kestel D; WHO mh GAP guideline team. The WHO Mental Health Gap Action Programme for mental, neurological, and substance use conditions: the new and updated guideline recommendations. Lancet Psychiatry. 2024;11(2):155-158. doi:10.1016/S 2215-0366(23)00370-X 37980915 · doi ↗ · pubmed ↗
- 4Keynejad R, Spagnolo J, Thornicroft G. WHO Mental Health Gap Action Programme (mh GAP) intervention guide: updated systematic review on evidence and impact. Evid Based Ment Health. 2021;24(3):124-130. doi:10.1136/ebmental-2021-300254 33903119 PMC 8311089 · doi ↗ · pubmed ↗
- 5Fekadu A, Demissie M, Birhane R, . Under detection of depression in primary care settings in low and middle-income countries: a systematic review and meta-analysis. Syst Rev. 2022;11(1):21. doi:10.1186/s 13643-022-01893-9 35123556 PMC 8818168 · doi ↗ · pubmed ↗
- 6Carter H, Araya R, Anjur K, Deng D, Naslund JA. The emergence of digital mental health in low-income and middle-income countries: a review of recent advances and implications for the treatment and prevention of mental disorders. J Psychiatr Res. 2021;133:223-246. doi:10.1016/j.jpsychires.2020.12.016 33360867 PMC 8801979 · doi ↗ · pubmed ↗
- 7Osei E, Mashamba-Thompson TP. Mobile health applications for disease screening and treatment support in low- and middle-income countries: a narrative review. Heliyon. 2021;7(3):e 06639. doi:10.1016/j.heliyon.2021.e 06639 33869857 PMC 8035664 · doi ↗ · pubmed ↗
- 8Luitel NP, Pudasaini K, Pokhrel P, . Development and functioning of the mobile app–based mh-GAP Intervention Guide in detection and treatment of people with mental health conditions in primary healthcare settings in Nepal. Glob Ment Health (Camb). 2023:10:e 90. doi:10.1017/gmh.2023.6938161752 PMC 10755379 · doi ↗ · pubmed ↗