Scoping review on the perceptions and attitude of women on methods for collecting cervicovaginal samples for Human Papillomavirus testing in Sub-Saharan Africa
Uduak Ima Andrew-Bassey, Deborah Olamiposi Oke, Michael A. Okunlola, Imran Morhason-Bello

TL;DR
This review explores how women in Sub-Saharan Africa perceive self-sampling for HPV testing, finding it preferred for privacy, comfort, and ease.
Contribution
The study provides new insights into women's attitudes toward self-sampling for HPV testing in Sub-Saharan Africa.
Findings
Women perceive self-sampling as more private, comfortable, and less painful than clinician sampling.
Self-sampling is viewed as easier and less embarrassing compared to clinician-collected samples.
Women prefer self-sampling in private hospital settings to reduce financial burden and seek reassurance.
Abstract
The burden of cervical cancer (CC) continues to rise in Sub-Saharan Africa (SSA) while some high-income countries are approaching elimination targets. Self-sampling for Human Papillomavirus (HPV) test for CC screening is increasingly used globally to accelerate wide coverage but some have reported barriers against its use. This scoping review explored published literature on the perception and attitude of women on the methods for collecting cervicovaginal samples for HPV testing for CC in SSA. This involves a review of electronic databases including Pubmed, Cochrane, Google Scholar, and African Journal Online. The review was limited to published English articles between 2013–2023 using the Arksey and O’Malley framework. Included studies were articles that used perception, attitude, perspective, or acceptability as primary or secondary outcome variables. Of the 137 articles, 131 articles…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
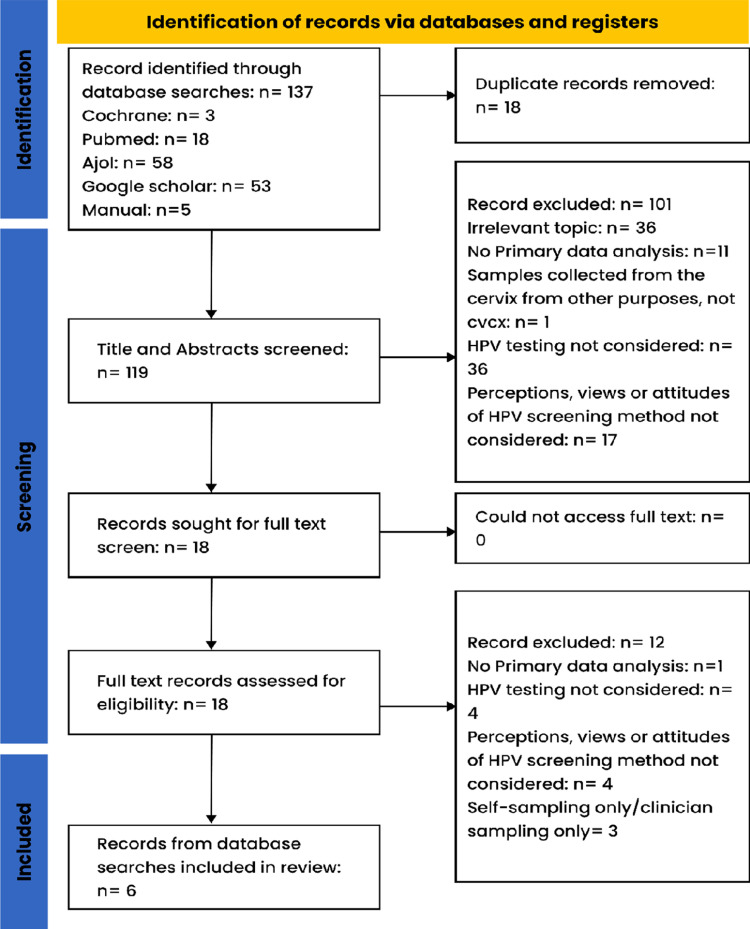 Fig 1
Fig 1- —http://dx.doi.org/10.13039/501100022496Institute for Life and Earth Sciences, Pan African University
- —http://dx.doi.org/10.13039/100000054National Cancer Institute
- —http://dx.doi.org/10.13039/100000054National Cancer Institute
- —http://dx.doi.org/10.13039/100000054National Cancer Institute
- —http://dx.doi.org/10.13039/100000054National Cancer Institute
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Global Cancer Incidence and Screening · Vaccine Coverage and Hesitancy
Introduction
The primary cause of almost all CCs is the persistence of high-risk human papillomavirus (HPV) infections in the transformation zone for nearly 2–7 years [1–3]. The latency period between the acquisition of high-risk HPV infections, its persistency, and the development of precancer and invasive cancer provides an opportunity for secondary prevention strategy including cytology and HPV-based testing [4]. Studies showed that the proportion of women who screen for CC is relatively low [5]. For example, a study reported that only 3.5% of women aged 25–65 years had ever screened for CC in the last three years [6]. Women in low-middle-income countries (LMICs) often face the challenges of poor access to screening services, lack of awareness and knowledge on cervical cancer (CC), screening, and sociocultural influences that prevent them from screening [7–9].
Some of the barriers associated with low CC screening using the clinician sample collection method include inadequately trained personnel, lack of functional referral and laboratory facilities, and lack of transport and follow-up systems [9,10]. Other barriers include embarrassment/shyness, pain, and/or dislike associated with pelvic examination, and spousal disapproval [11]. The World Health Organization (WHO) recommends HPV testing and treatment for women at risk of developing CC as part of efforts to eliminate the disease globally [12]. Self-sampling (SS) of cervicovaginal samples presents a unique opportunity to mitigate the challenges of barriers associated with healthcare provider’s collection of samples for HPV testing and cytological screening [13,14]. HPV testing presents women with the option of self-collection of cervicovaginal samples by removing the barriers associated with a third person’s engagement to collect cytology samples.
Studies have demonstrated that the quality of biological samples collected and DNA extracted from SS are similar to those collected by healthcare providers (HCP) [15–18]. Despite the opportunities that SS presents, it is important to assess the perception of women within the African context as a preliminary step and its implication in integrating this method of sample collection for CC screening programs. The perception of women who had experienced SS in SSA is yet to be reviewed across different settings to fully understand their preferences and concerns. This scoping review explored published literature on perceptions and attitudes of women on the collection of cervicovaginal samples for HPV testing in SSA, and it also identified potential gaps with this method as a proxy for assessing the effectiveness of CC screening in SSA.
Objective
The objective of this review is to explore published literature on the perception and attitude of women on the methods for collecting cervicovaginal samples for HPV testing for CC in SSA.
Methods
Protocol and registration
The protocol for this review has been published (https://doi.org/10.1136/bmjopen-2024-085408) [19].
Eligibility criteria
The eligibility requirements were created using the PICO format (population, intervention, comparator, and outcome) (Table 1). The studies were qualitative, quantitative, or mixed-method designs (a) published in peer-reviewed journals as either observational or experimental designs on the perception or attitude of women on methods of collecting cervicovaginal samples for CC screening and, (b) data collected in SSA among indigenous black women population. We excluded case reports, letters to editors, or expert opinions without primary data on methods of collecting samples for CC screening and original articles on this subject that were conducted outside SSA. Only English publications were included to avoid the cost and time required to translate foreign languages.
Table 1: Table showing eligibility criteria for the review using PICO format.
Information sources
A systematic search of electronic databases including PubMed (a medical/health-related journal), Cochrane (Cochrane evidence provides high-quality information to enhance your healthcare knowledge and decision-making), AJOL (African Journals Online is rich in African journals), and Google Scholar (indexes the full text or metadata of scholarly literature across an array of publishing formats and disciplines) was conducted. In addition, grey literatures were reviewed to complement the original search strategy. The search criteria were limited to published original research studies conducted in community or clinical settings in SSA in the last ten (10) years (2013–2023).
Search
The following keywords were used to search the databases: HPV/ Human papillomavirus/ papillomavirus, cervical cancer/ adenocarcinoma, sample collection, sample taking, self-sample, cervical cancer screening, perception/view, attitude, and SSA using sub-regions within SSA (West Africa OR East Africa OR Central Africa OR Southern Africa), and by specific country names. Boolean terms AND/OR were used to separate the keywords during the search. Medical Subject Headings (MeSH) terms were used in the search terms. The references and bibliographies of relevant articles were manually searched. The search was conducted between December 2023 and March 2024 including articles with publication dates in 2013–2023 (S1 Data).
Selection of sources of evidence
The search was initially conducted by UAB verified by the two senior authors on 20^th^ March 2024 and finalized on 28th March 2024. The titles were imported into EndNOTE software to compile results from all the databases. UAB and DOO independently screened the articles/titles using PICO criteria for eligibility while IMB served as the tiebreaker. After, UAB and DOO screened all full texts of selected articles for eligibility and those found to meet the criteria were included for data extraction and mapping (S2 Data).
Data charting process
Eligible studies were presented on a Preferred Reporting Items for Systematic Reviews and Meta-Analyses-extension (PRISMA) Flow chart diagram for scoping review (Fig 1) to summarise the process and number of articles that were finally selected for chart abstraction [20,21].
Preferred Reporting Items for Systematic Reviews and Meta-Analyses-extension (PRISMA) Flow chart diagram for scoping review.
Data items and synthesis of results
We created a two-data abstraction form with Microsoft Excel sheets using the following data charting fields. Sheet 1 includes data on authors, date, country, study population/ sample size, method of recruitment, type of cervical screening, and procedure for sample collection (Table 2). Sheet 2 includes data on authors, date, country, aim/objectives, measurement of perception (quantitative/qualitative/mixed), assessment for perception (descriptive/multivariate/test of association), methods of cervicovaginal sample collection conducted, outcome measure, and summary of key findings (Table 3). The data extracted were presented in Tables 2–3 to summarise eligible articles, description of perceptions and attitudes towards CC screening, and methods of collecting cervicovaginal samples.
Table 2: Description of included studies, method of participant’s recruitment, and type of cervical screening conducted.
Table 3: Selected studies on perception and attitude of self-sampling in sub-Saharan Africa reporting key findings.
Results
Selection of sources of evidence
One hundred and thirty-seven (137) articles were reviewed, six (6) met the inclusion criteria [1,16,18,22–24]. The flow chart for screening and reasons for exclusion were shown in (Fig 1).
Characteristics of sources of evidence
Each included source of evidence has been charted on (Fig 1). Two (2) of these manuscripts were from Southern Africa (Botswana [23] and South Africa [22]); two (2) from Central Africa (Cameroon (2) [1,24]); One (1) from West Africa (Ghana) [16] and one from East Africa (Tanzania) [18]. Five (5) of eligible articles were conducted over five years ago (2017–2022) [1,16,18,22,23] and only one (1) study was conducted over ten (10) years ago [24]. The age range of participants were between 18 and 65 years old. Three (3) studies included women 25 years and above [18,23,24], two (2) included women 30 and above [1,22], and one (1) 18 and above [16]. All six (6) studies were hospital-based [1,16,18,22–24]. Of the four (4) studies that conducted quantitative analyses, two (2) studies were face-to-face interviews [16,23], while two (2) studies used self-administered questionnaires to collect data [22,24].
Synthesis of results
Quality of DNA sample collected.
Six (6) studies assessed the quality of DNA samples [1,16,18,22–24]. Overall, women felt that the quality of DNA collected by HCP was more reliable compared to those collected during SS [1,16,18,22–24]. Some participants (76.1%) [1] and (23.1%) [23] believed that the quality of DNA collected by HCP was better because they were regarded as experts [1,23]. In a South African study, 45.1% women felt that the HCP could detect abnormalities aside from precancerous lesions [22]. A qualitative study conducted in Tanzania reported that most women perceived they were capable of collecting accurate samples in the presence of a nurse [18]. However, two studies reported a similar DNA quality in the cervicovaginal samples collected by HCPs and during SS [16,18]. Lastly, a study reported a sensitivity of 92.6% sensitivity and a specificity of 95.9% [16].
Perception and attitude of women about self-sampling.
Perception, attitude, perspective, and acceptability were used interchangeably in many studies [8,16,18,19,22–24]. The themes used to describe perception and attitude include privacy and comfortability; willingness to self-sample; pain experienced; embarrassment; anxiety; and confidence [8,16,18,19,22–24].
Privacy and comfortability: Five (5) studies reported that women perceived SS as a form of protection for their privacy and had better comfort when compared to clinician sampling methods [1,18,22–24]. A study reported that 16.1% of women preferred SS over HCP sampling due to the possibility of increased privacy [1]. In another study conducted among women living with HIV (WLWH) in Botswana, 90% of the women agreed that SS was more comfortable than HCP sampling [23].
Willingness to self-sample: Three (3) studies reported the willingness of women to self-sample [1,22,23]. A study conducted in South Africa reported that 93.9% women were willing to self-sample [22]. In a comparative study in Cameroon, 76.9% women willingness to self-sample compared to 23.1% women willing to present for provider sampling [1]. The same study reported that 99% of women were willing to self-sample again and refer other women for similar method of sample collection [1]. This is similar to findings from another study that reported 95% of women willing to self-sample again [23].
Pain and anxiety: Five (5) studies assessed the level of pain experienced during SS compared with provider sampling [1,18,22–24]. Overall, the majority of the studies reported that women perceived that SS was less painful relative to provider sampling [18,22–24]. A study reported that SS was associated with lesser pain while more than a third had a negative painful experience (37.5%) and physical discomfort (36%) [23]. Also, majority of women in two studies felt less anxious about SS 73% [24] and 96.5% [1]. However, 2 out of 11 women in a Tanzanian study reported per vaginam after SS [18]. Experience of bleeding was not reported during and after provider sampling.
Embarrassment: Four (4) studies assessed embarrassment as a measure of women’s perception [1,22–24]. A study in South Africa reported that 93.6% of women felt less embarrassed during SS compared with 88.2% of women during provider sampling [22]. Another study conducted in Cameroon reported that 99.3% of women felt less embarrassed during SS compared with 98.6% of women during provider sampling [1]. Also, another study in Cameroon reported that 84% of women felt less embarrassed to self-sample compared with the clinician sample [24]. These findings were corroborated by the FDG participants stating that they felt shy to open up to a clinician [22]. However, another study reported that an equal proportion of women felt embarrassed during SS and provider sampling (3%) [23].
Confidence: Five (5) studies assessed confidence as a measure of women’s perception [1,18,23,24]. A study conducted in Cameroon reported that 57.6% of women felt moderate or high confidence when they SS [24]. This is similar to a study among WLWH in Botswana which reported that 90.3% of women felt somewhat or extremely confident while SS [23]. A study in Cameroon reported a slightly greater proportion of women (SS: 98.9%; HCP: 99.4%) confident for provider sampling compared to SS [1]. However, a study conducted among Tanzanian women reported that the participants were not confident to self-sample except in the presence of a nurse [18]. Also, women were more confident when the sample was taken by a clinician (64.7%) than SS (59.5%) [22].
Procedure for self-sampling.
Five (5) studies reported women’s perception of SS collection procedures [16,18,22–24]. Overall, 76.3% [16], 82% [24], and 89% [23] women reported that SS was easy compared to provider sampling. The women were also satisfied with the content of the instructions given for SS [22,24]. A study conducted in Tanzania showed that women were more comfortable with SS when nurses or other healthcare workers were present than when they were left alone to self-collect [18].
Location for self-sampling for CC screening.
Three (3) studies reported preference for collecting cervicovaginal samples in the hospital rather than at home [1,18,22]. A study conducted in Cameroon reported that 96.6% of women preferred SS in a medical center over home-based screening [1]. This was because 36% of women were scared of performing the test inappropriately and 12% were scared of contamination if performed at home [1]. Other studies reported reassurance by clinicians [18,22], and the financial burden associated with visiting the health facility twice [22] as reasons women preferred SS in the hospital. However, a study conducted in Cameroon reported that 39% of women agreed to SS at home if introduced to regular screening [24].
Discussion
Summary of evidence
This scoping provides a synthesis of information on the perception and attitude of women towards sampling methods for CC screening. Our results confirmed the paucity of research on the subject in SSA. All the six studies were hospital-based and they described perception and attitudes using the following themes: Privacy and comfortability; Willingness to SS; Pain; Anxiety; Embarrassment and Confidence [1,16,18,22–24].
Self-sampling method was generally reported to protect their privacy and provided a better comfort than HCP-initiated sampling of cervicovaginal samples [1,18,22–24]. Privacy protection and comfort are important drivers that motivate clients to consent for gynaecological procedures particularly when it involves exposure of genital areas [25,26]. The presence of HCPs sometimes might create tension, anxiety, and feelings of intrusion when clients have not had any encounter or speak the same language with them [27,28]. It is also plausible that women could have mentioned privacy because of their feeling of being in control of themselves while collecting their samples. To mitigate this challenge, several strategies were employed including enforcement of using chaperons, counseling sessions before the procedure/examination, and use of audiovisual aids [29,30]. In other settings, women expressed similar reasons for privacy and comfort as a motivation for preferring self-sampling to provider-initiated sampling [14,31,32].
Three (3) studies showed that women were willing to self-sample [1,22,23]. Studies have shown that SS for HPV testing promises to increase screening rates because more women will be willing to self-sample compared to the HCP method [33–36]. However, 23.1% of women in one of the studies were willing to undergo provider sampling [1]. This could be a result of the confidence people/patients have in their HCPs [37].
Another important motivation for preferring SS is the perception by women that it is less painful than HCP-initiated sampling. Although none of the studies objectively assessed pain perception between SS and HCP-initiated sampling, the feeling of having lesser pain could be due to the general feeling of self-control during sample collection. It is also possible that the bleeding and pain experienced by participants could be suggestive that the screening instruction was not properly communicated to the study participants. Several other studies have reported similar findings regarding less pain during SS compared to more pain during provider sampling [31,33,38,39]. However, the bleeding experienced by WLWH could be attributed to the strong trust that exists between WLWH and their provider [40]. Hence, these women were nervous to self-collect samples. We recommend educational interventions tailored to providers to educate and encourage patients on the importance of SS options, especially providers working with WLWH.
Four studies reported that most of the participants believed that self-sampling made them feel less embarrassed compared to HCP sampling [1,22–24]. It is common knowledge that women had always expressed concerns such as feelings of embarrassment during any clinical scenarios that involve the insertion of instrument or examination of their vagina or cervix [41]. The incentive of allowing women to collect their samples may obviate this feeling of embarrassment including the extreme situation of vaginismus or frigidity.
The confidence to self-collect their samples for CC screening was overwhelmingly reported in four studies that were included in this review [1,18,23,24]. Some studies in this review showed that a few women that had secondary medical conditions such as HIV infections preferred health provider-initiated sampling relative to SS [1,22]. These women were not confident to perform SS and would rather want clinicians to examine them in addition to collecting their cervicovaginal samples. However, some women might require the assistance of healthcare providers to reinforce their confidence to perform SS [1,23,24]. Some studies outside SSA have reported similar findings that women with immunocompromised medical conditions have low self-confidence [42–44].
Overall, most of the women in the six studies perceived that the quality of DNA samples collected by the HCPs was more reliable compared to those self-collected [1,18,22–24]. This finding contrasts with findings from studies that tested the quality of DNA between specimen collected from SS and those collected by HCP [16,18]. For example, a study showed that the cervicovaginal samples collected by SS and HCP had similar high sensitivity (92.6%) and specificity (95.9%) [16].
Another important benefit of SS mentioned by women is the relatively lower overall cost of using this technique than the HCP-initiated sampling. For example, the cost of consumables for SS is generally lower and there might not be any need for hospital visitation [22,45,46].
Limitations
The interpretation of findings from this scoping review is limited because of the following reasons. First, this scoping review did not include published manuscripts from non-English journals, and this omission could have introduced some bias. Second, out of the eligible studies, there was no community-based study which might have implication on the generalisability of our findings. Third, we did not assess for risk of bias in this review as it was not a systematic review. Despite these limitations, this review provided the first synthesis of evidence to compare SS and HCP initiated collection of cervicovaginal samples.
Conclusion
In conclusion, this review showed an increasing preference for SS for collecting cervicovaginal sample for CC screening relative to HCP methods by women in SSA. It is important that clinicians and program planners increased sensitization of SS and encourage women to self-collect cervicovaginal samples as a motivation for increasing the uptake of CC screening in SSA. Future studies should explore motivations and barriers as well as possible integration of SS into different health system involved in CC screening.
Supporting information
S1 TableTable showing eligibility criteria for the review using PICO format.(DOCX)
S2 TableDescription of included studies, method of participant’s recruitment, and type of cervical screening conducted.(DOCX)
S3 TableSelected studies on perception and attitude of self-sampling in sub-saharan africa reporting key findings.(DOCX)
S1 DataDetails of search strategy.(DOCX)
S2 DataResult from different databases.(XLSX)
S1 ChecklistPreferred reporting items for systematic reviews and meta-analyses extension for scoping reviews (PRISMA-ScR) checklist.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sormani J, Kenfack B, Wisniak A, Moukam Datchoua A, Lemoupa Makajio S, Schmidt NC, et al. Exploring factors associated with patients who prefer clinician-sampling to HPV self-sampling: a study conducted in a low-resource setting. Int J Environ Res Public Health. 2021;19(1):54. doi: 10.3390/ijerph 19010054 35010314 PMC 8744711 · doi ↗ · pubmed ↗
- 2Louie KS, de Sanjose S, Mayaud P. Epidemiology and prevention of human papillomavirus and cervical cancer in sub-Saharan Africa: a comprehensive review. Trop Med Int Health. 2009;14(10):1287–302. doi: 10.1111/j.1365-3156.2009.02372.x 19772550 · doi ↗ · pubmed ↗
- 3Aerssens A, Claeys P, Beerens E, Garcia A, Weyers S, Van Renterghem L, et al. Prediction of recurrent disease by cytology and HPV testing after treatment of cervical intraepithelial neoplasia. Cytopathology. 2009;20(1):27–35. doi: 10.1111/j.1365-2303.2008.00567.x 18510550 · doi ↗ · pubmed ↗
- 4Castle PE, Einstein MH, Sahasrabuddhe VV. Cervical cancer prevention and control in women living with human immunodeficiency virus. CA Cancer J Clin. 2021;71(6):505–26. doi: 10.3322/caac.21696 34499351 PMC 10054840 · doi ↗ · pubmed ↗
- 5Yang L, Boily M-C, Rönn MM, Obiri-Yeboah D, Morhason-Bello I, Meda N, et al. Regional and country-level trends in cervical cancer screening coverage in sub-Saharan Africa: a systematic analysis of population-based surveys (2000-2020). P Lo S Med. 2023;20(1):e 1004143. doi: 10.1371/journal.pmed.1004143 36634119 PMC 9882915 · doi ↗ · pubmed ↗
- 6Bruni L, Serrano B, Roura E, Alemany L, Cowan M, Herrero R, et al. Cervical cancer screening programmes and age-specific coverage estimates for 202 countries and territories worldwide: a review and synthetic analysis. Lancet Glob Health. 2022;10(8):e 1115–27. doi: 10.1016/S 2214-109X(22)00241-8 35839811 PMC 9296658 · doi ↗ · pubmed ↗
- 7Denny L, Quinn M, Sankaranarayanan R. Chapter 8: screening for cervical cancer in developing countries. Vaccine. 2006;24 Suppl 3:S 3/71-7. doi: 10.1016/j.vaccine.2006.05.121 16950020 · doi ↗ · pubmed ↗
- 8Oketch SY, Kwena Z, Choi Y, Adewumi K, Moghadassi M, Bukusi EA, et al. Perspectives of women participating in a cervical cancer screening campaign with community-based HPV self-sampling in rural western Kenya: a qualitative study. BMC Womens Health. 2019;19(1):75. doi: 10.1186/s 12905-019-0778-2 31196175 PMC 6567898 · doi ↗ · pubmed ↗