Beyond Ulcerations: A Case of Cutaneous Polyarteritis Nodosa in a Middle-Aged Woman
Saadia Boughaleb, Hanane Baybay, Imane Fadlallah, Layla Tahiri Elousrouti, FatimaZahra Mernissi

TL;DR
A middle-aged woman with persistent leg ulcers was diagnosed with cutaneous polyarteritis nodosa and successfully treated with immunosuppressive therapy.
Contribution
This case highlights the clinical features and management of cutaneous polyarteritis nodosa in a patient with chronic lower-extremity ulcers.
Findings
The patient's histopathology confirmed necrotizing arteritis consistent with cutaneous polyarteritis nodosa.
Treatment with corticosteroids and azathioprine led to clinical remission without systemic disease progression.
The case emphasizes the need for multidisciplinary care in managing recalcitrant lower-extremity ulcers.
Abstract
Polyarteritis nodosa (PAN) is an immune-mediated necrotizing vasculitis predominantly affecting medium-sized arteries, often manifesting with systemic involvement in its classic form. However, a cutaneous variant (cutaneous polyarteritis nodosa (c-PAN)) confines the disease process to the skin and subcutaneous tissues, typically presenting with painful nodules, chronic ulcerations, and livedo reticularis while sparing major organ systems. Here, we describe a 53-year-old woman with type 2 diabetes and hypertension who developed persistent, painful ulcerative nodules on her lower legs over six months. Laboratory investigations revealed elevated inflammatory markers, negative ANCA, and slightly increased C3. Histopathology confirmed necrotizing arteritis of medium-sized arteries with lobular panniculitis, consistent with c-PAN. She was treated successfully with oral corticosteroids,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
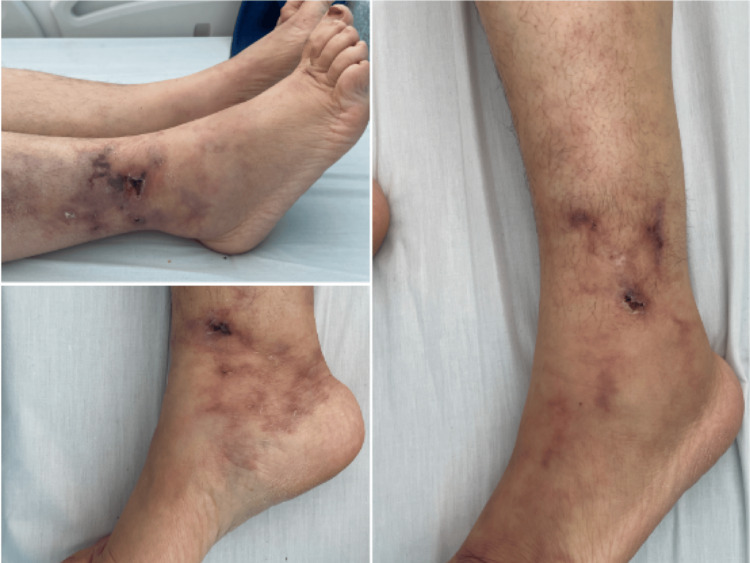 Figure 1
Figure 1 Figure 2
Figure 2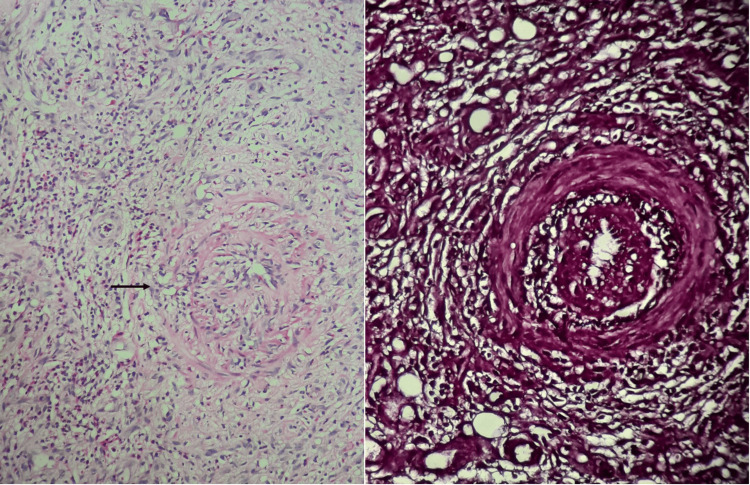 Figure 3
Figure 3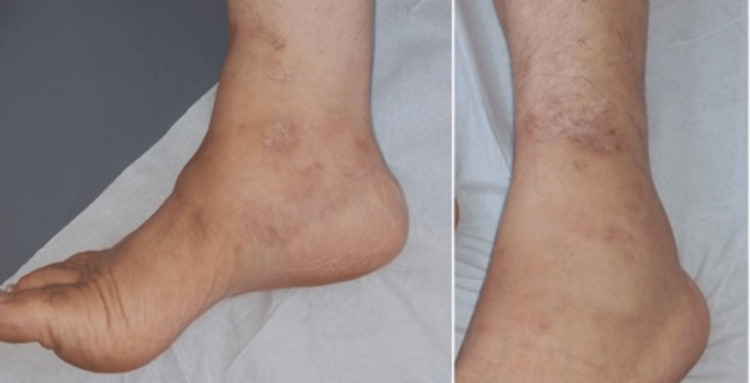 Figure 4
Figure 4| Laboratory tests | Value | Reference range |
| C3 | 1.89 g/L (slightly elevated, indicating inflammation) | 0.75 - 1.75 g/L |
| C4 | 0.38 g/L | 0.2 - 0.5 g/L |
| ESR | 150 mm/h (markedly elevated, indicating inflammation) | 0-15 mm/hr |
| CRP | 45 mg/L (markedly elevated, indicating inflammation) | 10 mg/L |
| Hepatitis B serology | Negative (no significant level of detectable) | Negative |
| Hepatitis C antibody | Negative (no significant level of detectable) | Negative |
| HIV serology | Negative (no significant level of detectable) | Negative |
| ANCA | Negative (no significant level of detectable) | < 20 |
| Cryoglobulins | Negative (no significant level of detectable) | Negative |
| Parvovirus B19 | Negative (no significant level of detectable) | < 0,9 IV |
| Cutaneous polyarteritis nodosa (c-PAN) | Livedoid vasculopathy | Necrotic angiodermatitis | |
| Epidemiology | Women in the age group of 45 to 50 years old | Women who are 45 to 50 years old with a history of diabetes and arterial hypertension | Women in the age group of 50 to 70 years with cardiovascular comorbidities |
| Common clinical presentation | Ramified livedo, purpura, necrosis, and ulceration with symmetrical involvement of the lower 1/3 of the legs, associated with white atrophy. No signs of venous insufficiency. No systemic involvement | Necrotic ulcer on the posterolateral legs. | |
| Distinct clinical findings | Subcutaneous nodules along arterial vessels, and loco-regional peripheral neuropathy | Nociceptive pain | Ragged and purpuric margins, rapidly extensive, and associated with exquisite pain |
| Histopathology | Segmental fibrinoid necrosis of medium-calibre arteries with perivascular neutrophilic infiltrate | Thrombosis of vessels in the superficial or middle dermis, with segmental hyalinization and lymphocytic perivascular infiltrate | Subcutaneous arteriosclerosis with hypertrophy of the media, thickening of the lamina, and intimal hyperplasia |
| Evolution | Chronic, relapsing-remitting course | Chronic, with no tendency to wound healing | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Amyloidosis: Diagnosis, Treatment, Outcomes · Coagulation, Bradykinin, Polyphosphates, and Angioedema
Introduction
Polyarteritis nodosa (PAN) is an immune-mediated necrotizing vasculitis that principally affects medium-sized muscular arteries and predominantly affects adults in their fifth decade. The "classic" systemic form of PAN typically involves multiple organ systems, most notably the renal, neurologic, and gastrointestinal systems, and has a male predominance. In contrast, the cutaneous-limited variant (cutaneous polyarteritis nodosa (c-PAN)) tends to affect women more frequently and, while generally confined to the skin and subcutaneous tissue, can still produce significant morbidity through painful subcutaneous nodules, livedo reticularis, and ulcerations [1,2].
The pathophysiology of systemic PAN often involves immune complex deposition, frequently associated with hepatitis B virus infection, leading to complement activation and endothelial damage. Conversely, in c-PAN, some studies have identified autoantibodies similar to those seen in antiphospholipid syndrome, suggesting distinct immunologic mechanisms [1].
Given its relative rarity and an often-overlapping clinical spectrum with conditions such as livedoid vasculopathy or other medium-to-small vessel vasculitides, diagnosing c-PAN depends on a combination of thorough systemic evaluations and characteristic histopathologic findings [3]. Herein, we report a chronic and successfully managed case of c-PAN in a middle-aged patient with metabolic comorbidities, highlighting the diagnostic considerations and therapeutic outcomes.
Case presentation
A 53-year-old married woman with a five-year history of type 2 diabetes and one year of hypertension presented with painful, progressively enlarging nodules and ulcerations on both lower legs. These lesions persisted for six months, intermittently healing and then recurring, leading to considerable discomfort and functional limitation. She reported occasional paresthesia in her feet, arthralgias, and two first-trimester miscarriages over a decade earlier, but no additional obstetric or gynecological issues.
Physical examination revealed multiple tender, round-to-irregular subcutaneous nodules that sometimes ulcerated, forming necrotic or hemorrhagic crusts, predominantly located in the perimalleolar region and the lower third of both legs. Livedo reticularis was noted, along with areas of hyperpigmentation (Figure 1).
Perimalleolar ulcerations and branching livedoid pattern on the lower legs Upper left panel showing the ulceration and livedo reticularis on the external side of the right leg. Lower right panel showing a smaller ulceration and livedo reticularis on the medial side of the left ankle. Panel on the right showing branched livedo and ulceration of the external side of the left leg.
Laboratory tests demonstrated elevated inflammatory markers (erythrocyte sedimentation rate (ESR) up to 150 mm/h, C-reactive protein (CRP) at 45 mg/L), borderline high C3 with normal C4, and negative serologies for hepatitis B/C, HIV, parvovirus B19, ANCA, and cryoglobulins (Table 1).
Imaging studies (Doppler ultrasound, abdominal angioscan) showed no arterial stenosis, aneurysms, or visceral lesions (Figure 2).
Abdominal angioscan Sagittal (A) and coronal (B) angioscanner reconstruction showing good opacification of the abdominal aorta (red arrows), its various visceral branches, and the iliac arterial axes, with a normal caliber and parallel walls, with no atheromatous, inflammatory, or additive parietal thickening. Coronal reconstruction at portal time (C) of abdominal scanner showing no digestive parietal thickening or other visceral abnormality.S: stomach; L: liver; C: colon; M: mesentery; Sp: spleen
A deep incisional biopsy at the edge of a representative ulcer confirmed necrotizing inflammation in medium-sized arterial walls with lobular panniculitis, consistent with c-PAN (Figure 3).
Histologic image of the deep incisional biopsy taken at the edge of an ulcerLeft image showing inflammatory infiltrate around medium-caliber vessels with leukocytoclasis and fibrinoid necrosis, giving an “onion-bulb” appearance (black arrow, hematoxylin, eosin, and saffron (HES) ×200). Image on the right of orcein staining highlighting the elastic fibers of an artery (orcein x200).
Electromyography indicated mild peripheral neuropathy, primarily attributed to her diabetes.
She began oral prednisone (0.5 mg/kg/day) and low-dose aspirin, later adding azathioprine as a steroid-sparing agent (200 mg/day). Daily wound care included debridement and dressing changes, which accelerated ulcer healing. Improvement in symptoms and noticeable wound healing were observed one month after treatment initiation. Over the ensuing months, prednisone was gradually tapered as lesions improved and discontinued by six months. Azathioprine was then reduced to 100 mg/day and completely stopped after one year without experiencing relapse or systemic progression (Figure 4).
Post-treatment follow-up with disappearance of livedo and subcutaneous nodules and residual atrophic whitish scarring.The left panel corresponds to the right lower leg and the right panel represents the left lower leg.
Discussion
c-PAN is a variant of PAN confined to the skin and subcutaneous tissues, sparing major organ systems in most cases [1,4]. Like systemic PAN, c-PAN is characterized by segmental necrotizing inflammation of medium-sized muscular arteries, which can lead to ischemia and infarction of the affected tissues. However, distinct from the classic systemic form, patients with c-PAN typically present with chronic or relapsing painful nodules, ulcerations, and livedo reticularis but lack systemic features such as significant renal, neurological, or gastrointestinal involvement [2].
Our patient’s profile (middle-aged, female, with comorbidities (type 2 diabetes and hypertension)) added complexity to wound healing and heightened the initial suspicion for alternative diagnoses like livedoid vasculopathy or necrotic angiodermatitis. The main distinctive features of these differential diagnoses are discussed in Table 2.
The negative ANCA in our patient, normal or only slightly altered complements, and absence of hepatic viral serologies also narrowed possibilities toward a vasculitis of medium-sized vessels rather than a small-vessel process. Finally, the key element was the histopathologic confirmation showing fibrinoid necrosis and perivascular infiltrates in medium-sized arteries within the subcutaneous fat [2, 3].
Long-term management of c-PAN typically involves corticosteroids as first-line therapy, often in conjunction with steroid-sparing agents such as azathioprine or methotrexate [1, 3, 8, 9]. This approach helps mitigate the side effects of prolonged high-dose steroid use. In our case, close follow-up ensured no systemic manifestations emerged, validating the diagnosis of a purely cutaneous-limited vasculitis. Recent studies have shown that remission and prevention of relapse can be achieved in many c-PAN cases if early, aggressive treatment is introduced, particularly in patients with comorbidities that might predispose them to worse outcomes [4, 10].
Although c-PAN is classically benign compared to systemic PAN, systemic evolution can occur in a small subset of patients, underscoring the need for routine monitoring, including laboratory screenings and clinical evaluations for evolving organ involvement [2]. The patient in this report highlights how a diligent, multidisciplinary care model, encompassing dermatology, rheumatology, and endocrinology, can optimize results. Key findings in our case include clinical presentation, absence of systemic involvement, histopathologic evidence, and favorable response to combined immunosuppressive and supportive therapies, with no relapse after gradual tapering.
Clinically, her outcome underscores the importance of early recognition and the role of a combined therapeutic strategy for sustained remission. The case also reaffirms that metabolic and vascular risk factors (diabetes, hypertension) may complicate the clinical picture by delaying ulcer healing, demanding a holistic approach to optimize comorbidity management.
Conclusions
c-PAN should be strongly considered in patients presenting with persistent, painful nodules and ulcerations confined to the lower extremities, particularly when small-vessel vasculitis and other vasculopathies have been excluded. Confirmatory biopsy, comprehensive systemic evaluation, and timely initiation of immunosuppressive therapy are crucial. This case illustrates the potential for complete remission and prevention of systemic progression with appropriate treatment and highlights the possibility of other differential diagnoses of chronic necrotic ulcerations of the lower legs in a middle-aged woman.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1High titer of anti-phosphatidylserine-prothrombin complex antibodies in patients with cutaneous polyarteritis nodosa Arthritis Rheum Kawakami T Yamazaki M Mizoguchi M Soma Y 150715135720071805017010.1002/art.23081 · doi ↗ · pubmed ↗
- 2Périartérite noueuse: état de l’art (Article in French)Rev Rhum Puéchal X 244251892022
- 3Efficacy and safety of treatments in cutaneous polyarteritis nodosa: a French observational retrospective study J Am Acad Dermatol Bettuzzi T Jachiet M Sbidian E 103510418620223422477110.1016/j.jaad.2021.06.872 · doi ↗ · pubmed ↗
- 4Intravenous immunoglobulins for cutaneous polyarteritis nodosa resistant to conventional treatment Scand J Rheumatol Breda L Franchini S Marzetti V Chiarelli F 1691704520162652603010.3109/03009742.2015.1092582 · doi ↗ · pubmed ↗
- 5Recognition and management of cutaneous polyarteritis nodosum versus livedoid vasculitis: a case report Cureus Forbes J Heydari M Kesselman MM Villacorta M 012202010.7759/cureus.6788 PMC 704599332140348 · doi ↗ · pubmed ↗
- 6Characteristics, risk factors and treatment reality in livedoid vasculopathy - a multicentre analysis J Eur Acad Dermatol Venereol Weishaupt C Strölin A Kahle B 178417913320193100911110.1111/jdv.15639 · doi ↗ · pubmed ↗
- 7Curing necrotic angiodermatitis with an intact fish skin graft in a patient living with diabetes Medicina (Kaunas) Dardari D Lequint C Jugnet AC Bénard T Bouly M Penfornis A 2925820223520861510.3390/medicina 58020292 PMC 8876191 · doi ↗ · pubmed ↗
- 8Cutaneous polyarteritis nodosa diagnosis and treatment: a retrospective case series J Am Acad Dermatol Stewart M Lo A Shojania K Au S Seidman MA Dutz JP Chan J 137013738720223571478510.1016/j.jaad.2022.06.009 · doi ↗ · pubmed ↗