Racial Inequities Influencing Admission, Disposition and Hospital Outcomes for Sickle Cell Anemia Patients: Insights from the National Inpatient Sample Database
Jayalekshmi Jayakumar, Nikhil Vojjala, Manasa Ginjupalli, Fiqe Khan, Meher Ayyazuddin, Davin Turku, Kalaivani Babu, Srinishant Rajarajan, Charmi Bhanushali, Tijin Ann Mathew, Poornima Ramadas, Geeta Krishnamoorty

TL;DR
The study finds racial disparities in hospital outcomes for sickle cell anemia patients, with African American and Hispanic patients facing worse outcomes than White patients.
Contribution
The study provides new insights into racial inequities in hospital care and outcomes for sickle cell disease using a large national database.
Findings
African American and Hispanic patients had higher rates of non-elective hospital admissions compared to White patients.
Hispanic patients had the highest in-hospital mortality rate among SCD patients.
African American and Hispanic patients faced increased risks of complications and longer hospital stays.
Abstract
Background: Sickle cell disease (SCD) significantly impacts diverse racial groups, particularly African American and Hispanic persons, who experience notable disparities in healthcare outcomes. Despite the extensive literature on SCD, studies focusing on in-hospital racial inequities remain limited. Methods: We conducted a retrospective analysis using the National Inpatient Sample (NIS) from 2016 to 2020, identifying adult hospitalizations for SCD (HbSS genotype). Hospitalizations were categorized by race—White, African American, Hispanic, and other, and analyzed for demographic variables, admission types, disposition outcomes, and complications. Statistical analyses included chi-square tests and multivariate logistic regression, adjusting for confounders. Results: Of the 1,089,270 identified hospitalizations, 90.31% were African American. African American and Hispanic patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
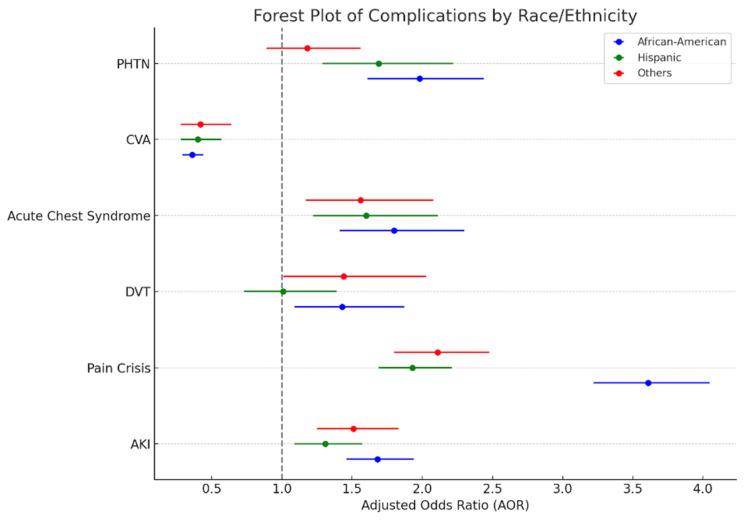 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHemoglobinopathies and Related Disorders · Healthcare Policy and Management · Food Security and Health in Diverse Populations
1. Introduction
Sickle cell disease (SCD) is an autosomal-recessive hemoglobinopathy which is caused by the replacement of negatively charged glutamine with the neutral valine at the 6th codon of the beta globin chain of Hemoglobin [1]. Historically, SCD is more prevalent in sub-Saharan Africa; however, recent data show that about 20 million people are affected by SCD worldwide and approximately 100,000 Americans have SCD [2,3]. Among African American births in the United States, the frequency of SCD is 1 in 360 live births [4]. The Centers for Disease Control and Prevention (CDC) estimates that 1 in 13 babies born to African American parents have the sickle cell trait, and 1 in 365 African Americans have SCD. Numerous studies underscore the criticality of risk stratification and the inclusion of race in elucidating disease processes. When it comes to SCD, the literature is scarce, and studies have mostly been conducted on targeted populations. Existing research focused on genetic and economic disparities among SCD patients, and studies specifically addressing in-hospital populations are rare [5,6]. Moreover, since most of the affected populations are of African American origin, existing research and therapy is focused on this subgroup which may jeopardize the outcomes of other minority populations with SCD. In this study, we analyzed the impact of race on in-hospital outcomes of SCD patients (HbSS genotype) with a focus on minority races. The study also analyzes the impact of race on admission and disposition outcomes which are known to cause a significant impact on healthcare burden and patient satisfaction [7].
2. Methods
2.1. Database—The National Inpatient Sample 2016–2020
The National Inpatient Sample (NIS) stands as the United States’ most extensive publicly accessible database for inpatient healthcare, encompassing data from various payers. It serves as a crucial tool for extensive data analysis, offering regional and national insights into inpatient usage, accessibility, costs, quality of care, insurance, demographic information, and clinical outcomes. Created through a collaborative effort between federal, state, and industry partners under the Agency for Healthcare Research and Quality’s Healthcare Cost and Utilization Project (HCUP), it includes information from approximately 20% of hospital admissions every year. As per our institution’s (Trinity Health Oakland) policy, Institutional Review Broad (IRB) approval is not required for studies utilizing deidentified database data; therefore, the use of NIS data for this study was deemed exempt.
2.2. Study Population and Study Variables
The NIS 2016–2020 was queried and International Classification of Disease—Tenth Edition—Clinical Modification (ICD-10-CM) codes were used to identify adult (age > 18 years) hospitalizations with a primary or secondary diagnosis of SCD with the HbSS genotype. This population was stratified by race into Whites, African Americans, Hispanics, and others (Asian, Native American, and Pacific Islander). Sociodemographic variables including age, sex, insurance, income quartiles, and hospital characteristics, including hospital size, location, region, and teaching status, were compared across different races. The main outcomes studied were the type of admission (elective vs. non-elective), the type of disposition (home vs. assisted living facility/home healthcare vs. died), and healthcare utilization (a length of stay greater than or less than 7 days). Complications of SCD hospitalizations like acute kidney injury (AKI), pain crisis, deep vein thrombosis (DVT), acute chest syndrome, cerebrovascular accident (CVA), and pulmonary hypertension (PHTN) were also compared across different races.
2.3. Statistical Analysis
A cross-sectional analysis was conducted using the STATA/MP 17.0 software. Categorical variables were compared using a chi-square test and continuous variables were compared using a t-test. p values < 0.05 were considered statistically significant. Multivariate logistic regression analysis was conducted to analyze the impact of race on the type of admission, the type of disposition, healthcare utilization, and complications like AKI, pain crisis, DVT, acute chest syndrome, CVA, and PHTN while accounting for pertinent confounders. These included socio-demographics, hospital characteristics, the Charlson comorbidity index [8], and other cardiac risk factors, including tobacco use, hypertension, hyperlipidemia, diabetes, cannabis use, and obesity.
3. Results
3.1. Patient- and Hospital-Level Characteristics
A total of 1,089,270 SCD hospitalizations were identified with a mean age of 35.81 years. In total, 65.29% of these patients were women. The majority of SCD hospitalizations were African American (90.31%), followed by Hispanics (4.08%), others (2.99%), and Whites (2.08%).
Less than 20% of hospitalizations among African Americans, Hispanics, and others were older than 65 years. However, among Whites, 36.22% were found to be greater than 65 years (p < 0.001). Irrespective of race, the majority of SCD hospitalizations were women (p < 0.001). In all race categories, the highest proportion of people had a median household income in the lowest income quartile, with 51.74% of African Americans and 45.91% of Hispanics in this category compared to 31.58% of Whites. Only 9.75% of African Americans SCD patients had income in the highest income quartile compared to 20.54% of Whites (p < 0.001). The majority of White SCD patients had private insurance (33.14%) whereas most African Americans (44.75%), Hispanics (53.21%), and others (45.74%) had Medicaid. (p < 0.001) Among Whites and African Americans, the majority were hospitalized in the Southern region of the United States whereas Hispanics and others were mostly hospitalized in the Northeast (p < 0.001). Irrespective of race, the majority were treated at urban teaching hospitals. (p < 0.001) (Table 1).
3.2. Primary Outcomes
In all races, most of the population had a routine discharge to home. Whites had a higher percentage of discharge to facility/home healthcare (21.09%) compared to African Americans (11.24%), Hispanics (9.97%), and others (12.3%) (p < 0.001). On univariate analysis without adjusting for confounders, Hispanics with SCD had the highest in-hospital mortality (0.82%), followed by Whites (0.8%), African Americans (0.64%), and others (0.54%). (p < 0.001). The highest proportion of hospitalizations from all races were admitted non-electively (p < 0.001) and had a length of stay less than 1 week (p < 0.001) (Table 2).
Multivariate logistic regression analysis, adjusted for confounders was performed after assigning Whites as the reference group. It showed that, compared to Whites, all other race categories had statistically significantly lower odds of being admitted electively to hospitals. It was also found that, as opposed to Whites, African Americans and others had statistically significantly higher odds of a prolonged hospital stay greater than 7 days [Adjusted Odds Ratio (AOR): 1.3 (95% Confidence Interval (CI): 1.17–1.42, p < 0.001) in African Americans and AOR: 1.2 (CI: 1.05–1.37, p = 0.006) in others]. No statistically significant associations were found between the races in terms of disposition to home vs. facility/home healthcare vs. died (Table 3).
3.3. In-Hospital Complications
Racial differences in the occurrence of the most common complications encountered in the in-patient population of SCD were analyzed using multivariate logistic regression analysis. This showed that, compared to Whites, African Americans, Hispanics, and others had statistically significantly higher odds of developing AKI, pain crisis, acute chest syndrome, and PHTN. On the contrary, the odds of the occurrence of cerebrovascular accidents were found to be lower in all other race categories compared to Whites. Higher odds of DVT were found among African Americans and others compared to Whites; however, the difference in the odds of developing DVT was not statistically significant in Hispanics compared to Whites (Table 4 and Figure 1).
4. Discussion
The findings of this study illuminate critical racial disparities affecting SCD patients in the United States during hospital admissions from 2016 to 2020. The distribution and characterization of SCD hospitalizations varied remarkably among races. In addition to having the highest proportion/burden of SCD hospitalizations, African Americans were also found to have significantly poor in-hospital outcomes compared to Whites. Previous studies had smaller sample sizes with more focus on the comparison of African Americans with Whites [9]. Our study also focused on Hispanics, the race category with the second highest prevalence of SCD in the United States (4.8%) [9], along with admission and disposition outcomes and in-hospital complications. Hispanics were also found to have notably worse in-hospital outcomes compared to Whites. This raises important questions about the systemic factors contributing to these inequities.
The analysis of the data reveals a significant disparity in the age distribution of individuals with SCD among different racial groups. Specifically, White patients exhibited a higher proportion of patients >65 years of age compared to the African American, Hispanic, and other racial categories, while the median life expectancy of SCD patients is 42 years for females and 38 years for males [10]. This higher life expectancy in White SCD patients may be due to a higher proportion of Whites in the highest income quartiles and a similar higher prevalence of private insurance among White individuals. This is supported by observations from previous research that have highlighted that SCD patients reliant on Medicare and Medicaid tend to experience lower life expectancies [11]. Additionally, it has been documented that Medicare and Medicaid beneficiaries often face limitations in their choices of nursing homes, with many options being of lower quality, leading to a higher likelihood of rejection compared to the options available to those with private insurance [12]. This may contribute to the observed pattern of higher rates of discharge to nursing homes for White patients. In contrast, other racial groups are more frequently discharged to home settings.
Compared to Whites, African Americans and Hispanics had higher odds of being admitted non-electively which contributes to higher healthcare utilization compared to elective admissions. A previous study has reported a declining trend of non-elective admissions for Whites and an increasing trend of the same for African Americans [13]. The observed a higher length of stay in African Americans can be attributed to a complex interaction between patient and healthcare-related factors like medication adherence, failure of physicians to timely recognize impending complications, difficulty with discharge planning, and suboptimal pain management [14]. The increased length of stay for African American patients could be supported by studies showing increased average wait times in emergency rooms for African American SCD patients leading to delays in care delivery [14]. A recent study also showed that patients who perceived discrimination in their care reported a higher pain burden, which could delay discharge due to an inability to achieve pain score goals [15].
African Americans, Hispanics, and others had higher odds of AKI, pain crisis, and acute chest syndrome compared to Whites. However, higher odds of developing PHTN were found only for African American and Hispanic SCD patients. This is consistent with studies showing a higher prevalence of PHTN in Hispanics and a lower incidence in Asian Americans owing to a lower left ventricular mass [16]. Compared to Whites, all other racial groups had lower odds of developing cerebrovascular accidents due to unclear reasons. An emerging body of research highlights the immune-modulating properties of young red blood cells (RBCs) (such as CD71+RBCs), which may influence complications or inflammatory responses in SCD patients. This offers insight into possible biological mechanisms underlying these disparities [17]. The socioeconomic disparities observed in African Americans in our study might also contribute to worse in-hospital complications among African Americans. While African Americans are well known to have higher disease severity in SCD due to genetic reasons, our study highlights many socioeconomic disparities involving African Americans, Hispanics, and others suggesting that systemic and socioeconomic factors also play a crucial role in driving racial disparities in healthcare.
The NIS lacks detailed patient-level data such as medications and laboratory results which could interfere with the studied outcomes. Thus, it was not feasible to eliminate these as potential confounders for the outcomes studied. The reliance on administrative data from the NIS may introduce potential inaccuracies or coding errors, which could affect the accuracy of diagnoses and identification of complications. As a cross-sectional analysis, this study can only establish associations, not causal relationships, between race and the outcomes examined. Despite efforts to control for confounding variables, there may be unmeasured or residual confounders that were not fully accounted for in the analysis. Since the NIS database only includes data from hospitalized patients in the United States, it may not fully represent the entire world population of SCD, which is more prevalent in Sub-Saharan Africa. As a result, applying our findings to a larger population could pose challenges. The cross-sectional nature of our study limits its ability to assess the frequency and impact of readmissions on the studied outcomes. However, despite these shortcomings, the compelling disparities encountered in our study provoke important inquiries into the impact on race on outcomes of SCD hospitalizations.
As we analyze these results, it is vital to consider the broader implications for healthcare delivery and policy aimed at improving the quality of care for marginalized racial groups. Understanding such health outcome variations among racial groups is crucial for developing tailored diagnostic and management protocols, ensuring equitable treatment efficacy.
5. Conclusions
In conclusion, this study reveals significant racial disparities in hospitalization outcomes for SCD patients, particularly highlighting the challenges faced by African American and Hispanic populations. The findings demonstrate that these groups experience higher rates of non-elective admissions, prolonged hospital stays, and increased complications, underscoring the need for targeted healthcare interventions. Addressing these inequities is crucial for improving patient outcomes and ensuring equitable care for all individuals affected by SCD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ehsan M. Maruvada S. Sickle Cell Anemia. Nih.gov. Stat Pearls Publishing 2023 Available online: https://www.ncbi.nlm.nih.gov/books/NBK 482164/(accessed on 12 November 2024)
- 2Naoum P.C. Sickle cell disease Rev. Bras. Hematol. Hemoter.2011337910.5581/1516-8484.2011000623284235 PMC 3521427 · doi ↗ · pubmed ↗
- 3National Heart, Lung, and Blood Institute Sickle Cell Disease—What Is Sickle Cell Disease?2023 Available online: https://www.nhlbi.nih.gov/health/sickle-cell-disease(accessed on 12 November 2024)
- 4Therrell B.L. Lloyd-Puryear M.A. Eckman J.R. Mann M.Y. Newborn screening for sickle cell diseases in the United States: A review of data spanning 2 decades Semin. Perinatol.20153923825110.1053/j.semperi.2015.03.00825979783 · doi ↗ · pubmed ↗
- 5Campbell A. Cong Z. Agodoa I. Song X. Martinez D.J. Black D. Lew C.R. Varker H. Chan C. Lanzkron S. The Economic Burden of End-Organ Damage Among Medicaid Patients with Sickle Cell Disease in the United States: A Population-Based Longitudinal Claims Study J. Manag. Care Spec. Pharm.2020261121112910.18553/jmcp.2020.2000932597290 PMC 10391152 · doi ↗ · pubmed ↗
- 6Saraf S.L. Molokie R.E. Nouraie M. Sable C.A. Luchtman-Jones L. Ensing G.J. Campbell A.D. Rana S.R. Niu X.M. Machado R.F. Differences in the clinical and genotypic presentation of sickle cell disease around the world Paediatr. Respir. Rev.20141541210.1016/j.prrv.2013.11.00324361300 PMC 3944316 · doi ↗ · pubmed ↗
- 7Fenton J.J. Jerant A.F. Franks P. Influence of Elective versus Emergent Hospital Admission on Patient Satisfaction J. Am. Board Fam. Med.20142724925710.3122/jabfm.2014.02.13017724610187 · doi ↗ · pubmed ↗
- 8Sundararajan V. Henderson T. Perry C. Muggivan A. Quan H. Ghali W.A. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality J. Clin. Epidemiol.2004571288129410.1016/j.jclinepi.2004.03.01215617955 · doi ↗ · pubmed ↗