Prevalence of VZV Reactivation and Effectiveness of Vaccination with Recombinant Adjuvanted Zoster Vaccine in Allogeneic Hematopoietic Stem Cell Recipients—A Single-Center Analysis
Ewa Karakulska-Prystupiuk, Magdalena Feliksbrot-Bratosiewicz, Maria Król, Agnieszka Tomaszewska, Wiesław Wiktor Jędrzejczak, Grzegorz Władysław Basak

TL;DR
This study examines how often shingles (VZV) reactivates in patients after a stem cell transplant and how effective a new vaccine is in preventing it.
Contribution
The study provides preliminary evidence on the safety and effectiveness of RZV vaccination in allo-HSCT recipients.
Findings
VZV reactivation occurred in 33% of patients, mostly after acyclovir prophylaxis ended.
RZV vaccination showed over 80% effectiveness in preventing shingles in this population.
Despite vaccination, 19% of recipients still developed herpes zoster.
Abstract
Background: Secondary immunodeficiencies in allo-HSCT (allogeneic hematopoietic stem cell transplantation) recipients increase the risk of viral reactivation, making vaccinations a vital issue. There is a paucity of data on the use of recombinant vaccine against herpes zoster (RZV) after allo-HSCT. Methods: This analysis included 149 recipients of allo-HSCT, transplanted in 2012–2022, mainly due to hematological malignancies (>95%). RZV was used from 2021 to 2023 according to the current recommendations of ACIP. The ELISA method was used to assess the VZV IgG antibody titers. Results: VZV reactivation was diagnosed in 49 out of 149 (33%) patients before vaccination, including 5 (3%) patients with reactivation within the first year after transplantation and the remaining 44 (30%) within the subsequent three years. At that time, the majority of patients were not receiving acyclovir…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
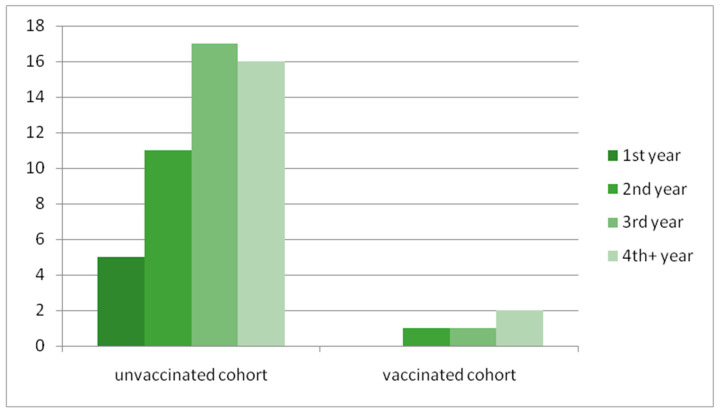 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHerpesvirus Infections and Treatments · Cytomegalovirus and herpesvirus research · Virus-based gene therapy research
1. Introduction
Recipients of allogeneic hematopoietic stem cell transplantation (allo-HSCT), especially those with graft-versus-host disease (GvHD), constitute a unique group of patients with secondary immunodeficiency (SID). Ablation of the hematopoietic system and damage to lymphopoietic organs due to toxic conditioning chemo-radiotherapy before transplantation lead to the impairment of cellular and humoral immunity. Restoring the total efficiency of the immune system is a multi-stage process spread over time. Cellular immunity deficiencies in allo-HSCT recipients significantly increase the risk of viral infections.
Varicella zoster virus (VZV) is a human alpha herpes virus surviving latent in ganglionic neurons and reactivating to produce herpes zoster (HZ, shingles). According to the literature data, over 90% of the world population harbors latent VZV [1]. At least 50% of infected individuals will reactivate this virus by 85 years of age to develop zoster [2]. During reactivation, VZV spreads transaxonally, but in immunosuppressed patients, may also be detected in peripheral blood mononuclear cells(PBMCs), which promote its dissemination [1,2,3,4,5]. Long-lasting postherpetic neuralgia may be an essential complication in many recipients [1]. The first objective of our study was to assess the incidence of HZ in recipients after HSCT.
Vaccination is a vital way to prevent symptomatic infection in HSCT recipients. However, the response to immunization in these SID patient populations may not be sufficient. There are two zoster vaccines: a live-attenuated vaccine, which is contraindicated in this setting, and the recombinant glycoprotein E vaccine. The efficacy of the recombinant HZ vaccine after autologous stem cell transplantation has been documented [6], but the data on its use after allo-HSCT are still limited. The Advisory Committee on Immunization Practices (ACIP) does not explicitly comment on these patients, choosing to await additional information [6,7,8,9,10,11,12]. Therefore, we considered it important to report our experience with recombinant vaccine against herpes zoster in this patient population.
2. Materials and Methods
2.1. Study Population
This is a retrospective analysis of patients after allo-HSCT was performed in the years 2012–2022 who remained under the care of the Outpatient Service in the single transplantation center. All patients signed written consent to receive vaccinations. The follow-up time for VZV reactivation in the unvaccinated patients was the first eight years after transplantation.
2.2. Allo-HSCT
The type of conditioning was chosen at the responsible physician’s discretion and depended on the underlying hematological disease. Immunosuppressive treatment (GvHD prophylaxis) was a combination of a calcineurin inhibitor (cyclosporin or tacrolimus) and an antiproliferative drug—a short course of either methotrexate or mycophenolate mofetil. All patients with unrelated or mismatched donors received anti-T-cell globulin (2.5–5 mg/kg daily) in a conditioning regimen for 2–3 days prior to transplantation. Diagnosis and grading of acute and chronic GvHD were performed based on clinical symptoms and/or biopsies according to established criteria. Grading of acute GvHD was performed according to the Glucksberg score, while the severity of chronic GvHD was determined according to the National Institutes of Health (NIH) Consensus Criteria 2014 [13,14,15].
All patients received anti-infective prophylaxis, including prophylactic antiviral treatment with acyclovir (Hasco-Lek, Wrocław, Poland) (400–800 mg twice daily) or with letermovir (Merck Sharp & Dohme B.V., Haarlem, The Netherlands) (240–480 mg daily) for the first 100 days after allo-HSCT followed by acyclovir (in doses as above) or valganciclovir (Accord Healthcare, North Harrow, Great Britain) (in the case of CMV reactivation, in doses adjusted for creatinine clearance). Immunosuppressive therapy was discontinued after 6–8 months following allo-HSCT if there was no significant GvHD. All patients who have been receiving immunosuppressive therapy due to cGvHD were advised to continue acyclovir treatment [7,12].
2.3. Types and Doses of Vaccine
Recombinant adjuvanted herpes zoster vaccine (RZV) was used in 2021–2023 in patients according to the current recommendations of the Advisory Committee on Immunization Practices (ACIP) for Immunocompromised Adults aged ≥19 years [10]. Vaccination included two doses of the vaccine given 1–2 months apart. The follow-up for efficacy was 1–3 years [8,9,10,11].
2.4. Methods
The anti-VZV (IgG) ELISA test(Euroimmun, Lübeck, Germany) was primarily used, with the result expressed as a ratio (the optical density (OD) of the patient sample divided by the OD of the cut-off). A ratio ≤ 0.8 was considered negative, 0.8–1.1 equivocal, and >1.1 positive. A direct chemiluminescent immunoassay (CLIA) by DiaSorin (analyzer LIAISON XL) (DiaSorin, Saluggia, Italy) was used in three patients, with quantitative results expressed in international units per milliliter (IU/mL). A titer ≥ 150 mIU/mL was considered a positive result. The comparison of the results of these two tests may only be qualitative because the ELISA ratio is a relative value and is not standardized to the WHO international unit. Peripheral blood lymphocyte subpopulations were analyzed using flow cytometry. The reference intervals were 309–1139 cells/μL for CD3+4+ cells, 137–823 cells/μL for CD3+8+ cells, 70–460 cells/μL for NK cells, and 80–430 cells/μL for CD19+ B-lymphocytes, and 1.0–5.0 for the CD4+ to CD8+ ratio. Post-vaccination complications were graded according to CTCAE5.0 criteria. Patients gave written consent to the intervention.
3. Results
3.1. Patients
The analysis included 149 patients, including 85(57%) males, with a median age of 47 years (range 18–73) at allo-HSCT. For twelve patients, this was their second allo-HSCT. The most prevalent diagnoses were acute myeloid leukemia (AML)—55%—then myelodysplastic syndrome (MDS) and acute lymphoblastic leukemia (ALL)—both 11.5%.
The patients’ baseline characteristics are shown in Table 1.
3.2. Transplantations
HLA-identical siblings were used for 49 (33%) patients, matched unrelated donors for 83 (56%), mismatched unrelated donors for 12 (8%), and haploidentical related donors for 5 (3%). In total, 104 (70%) patients received myeloablative conditioning (MAC), 40 (27%) reduced-intensity conditioning (RIC), and 5 (3%) non-myeloablative conditioning (NMA).
3.3. GvHD
A total of 64 (43%) patients suffered from acute and 85 (57%) from chronic GvHD. Altogether, 67 (45%) patients required chronic immunosuppressive therapy (mostly calcineurin inhibitors) because of moderate or severe chronic GvHD.
3.4. The Prevalence of VZV Reactivation in the Entire Group Before Vaccination
VZV reactivation was diagnosed in 49 out of 149 (33%) patients, including 5 (3%) patients with reactivation within the first year after transplantation and the remaining 44 (30%) within the subsequent three years.
At this time, the majority of patients no longer received acyclovir prophylaxis, including five patients who stopped recommended prophylaxis despite receiving immunosuppressive treatment (three due to chronic GvHD, two for its prevention). The most common clinical manifestation of VZV reactivation involving intercostal nerves was diagnosed in 40 (81%) patients. The remaining patients had unusual locations, including three patients with cranial nerve involvement, two with ophthalmicus, two with ulnar nerves, one with sacral plexus involvement, and one with a disseminated form of herpes zoster (HZ, diagnosed in a patient with Wiskott–Aldrich syndrome). Four patients required hospitalization: one due to disseminated herpes zoster, one due to ophtalmicus, and two others for infectious complications (1—pneumonia, 1—bronchitis). Postherpetic neuralgia was an essential complication in many of them. There was no intercurrent infection with Epstein–Barr virus or cytomegalovirus in patients with HZ, but in two of them, shingles appeared 24 h after the SARS-CoV2 mRNA vaccine. Figure 1 shows the time from allo-HSCT to VZV reactivation in unvaccinated and vaccinated cohorts. Table 2 summarizes the course of HZ in unvaccinated patients.
3.5. The Assessment of the Vaccinated Group
Twenty-one recipients (median age: 41) received two doses of RZV (median time 34 months after transplantation (range, 12–84 months)). Patients were vaccinated when the vaccine became available, which resulted in variability in time duration between transplantation and vaccination. There were 11 seronegative, 2 equivocal, 1 seropositive, and 7-unassessed patients before vaccinations (all with a history of chickenpox in childhood). Eighteen of them had been vaccinated at an interval of 1 month, and the remaining three at an interval of 2 months. Several patients complained about mild pain, erythema, swelling, or fatigue—CTCAE grade 1 after injection.
At the time of vaccination, four patients had been receiving chronic immunosuppressive treatment due to severe (three patients) or moderate (one patient) chronic cGvHD. The serological post-vaccination response (measured 2–3 months after vaccination) was confirmed in 12 (57%) recipients, with a ratio of 2.38–8.3 (median 5.095). Despite vaccination, four patients developed HZ. These patients were not receiving immunosuppressive therapy at the time of disease onset. One of them, who initially had myelodysplastic syndrome, had received rituximab a year earlier for PRCA (pure red cell aplasia) after transplantation. Three others underwent transplantation for lymphoid malignancies (two—B-cell ALL, one—DLBCL), including one who required IgG supplementation until 3 months before disease onset. Three of these patients had a positive serological response to vaccinations.
The median counts of total blood cells in the vaccinated group 1–4 months before vaccination were 451 (range 309–1139) for CD3+4+, 855 (range 137–823) for CD3+8+, 406 (range 70–460) for CD19+, and 211 (range 80–430) for NK cells. None of the vaccinated patients had decreased counts of total CD3+8+, or CD19+ below LLN. All but three (86%) had a lower CD4/CD8 ratio. Six vaccinated patients had absolute counts of total CD3+CD4+cells below LLN, including two who developed clinical disease. Three vaccinated patients had absolute counts of total NK cells below LLN, including one with clinical disease. The vaccinated patients’ characteristics are shown in Table 3.
4. Discussion
Secondary immunodeficiencies observed in HSCT recipients increase the risk of VZV reactivation, according to the Hope-Simpson hypothesis that a person’s immune status determines their likelihood of developing HZ [1]. Pre-, peri-, and post-transplant factors, especially multi-stage immune reconstitution, lead to humoral and cellular deficiencies that may promote the occurrence of HZ.
Another critical issue may be immunosenescence, a documented factor that causes virus-specific cellular immunity to wane with age [2,3,4]. Faster-aging lymphoid-biased HSCs (Ly-HSCs) in post-HSCT do not efficiently generate lymphoid progeny and can weaken VZV-specific CMI (T-cell-mediated immune) response [15,16,17,18,19].
The first objective of our study was to assess the incidence of HZ in recipients after HSCT, and VZV reactivation was diagnosed in 33% of patients within the first four years after transplantation. Apparently, acyclovir prophylaxis during the first year post-transplantation, used according to the EBMT guidelines, reduced the frequency of VZV reactivation during this time. Still, the frequency of the disease in the later period after transplantation (without prophylaxis) was a significant challenge [7,12].
According to the literature data, a delayed increase in VZV reactivation may be explained by the underlying immunosuppression rather than a possibility of a “rebound” effect. However, randomized studies suggest that subclinical VZV reactivation (endogenous and exogenous amplification) continues independently of acyclovir prophylaxis and that antigen exposure is sufficient for VZV-specific immune reconstitution [20,21].
The frequency of VZV reactivation varies depending on the transplant center; it was reported to be between 20% and 53%, with an increasing frequency in subsequent years (5% in the first year after HSCT, 21% in the second year, 22.9% in the third year, and 37% in the fifth year). This rate of VZV reactivation in the analyzed group of HSCT recipients is significantly increased compared to people of similar age in the non-HSCT population, where the frequency is reported to be only 7–8‰ [1,4,22].
Nineteen percent of our patients had unusual clinical manifestations of VZV reactivation, including two who developed ulnar nerve involvement after COVID-19 vaccination. VZV reactivation is a known potential adverse event for all COVID-19 vaccines [23]. However, manifestation involving dermatomes of the vaccinated arm has not yet been described.
Four (8.1%) of our patients required hospitalization, a significantly higher number compared to the non-HSCT population (0.05‰) [22]. One of these cases was a man initially suffering from primary immunodeficiency (PID) who developed severe disseminated HZ. It is known that PID recipients may experience poorer T- and B-cell reconstitution after allo-HSCT, which may complicate the course of the disease [19,24].
It is also worth mentioning that having shingles exposes this vulnerable group of patients to the risk of long-term transplant complications, such as increased risk of secondary cancer, stroke, myocardial infarction, and, crucially, persistent postherpetic neuralgia [24,25,26,27,28,29,30,31,32,33,34].
The second part of our study was devoted to the problem of vaccination with the recombinant, adjuvanted zoster vaccine.
The efficacy of this vaccine in the analyzed group, measured by the number of HZ occurrences after vaccination, was over 80%. There are not many data on the effectiveness of the recombinant vaccine against herpes zoster after allo-HSCT. In a randomized clinical trial of auto-HSCT recipients, the efficacy of vaccines was 63.8%. In contrast, in a single-center prospective study of allo-HSCT recipients published by Baumrin et al., it was 97.5% [27]. The comparison of the obtained results is difficult, considering the different vaccination schedules and different elapsed times between transplantation and the start of vaccination.
It is essential to determine the optimal time to administer vaccinations, considering immune reconstitution, especially the counts of CD4+ and CD8+ effector and memory T cells (because of their importance in T-cell-mediated VZV-immune (CMI) responses). None of the analyzed vaccinated patients had decreased counts of total CD3+8, whereas six of the CD3+4+ counts were diminished. Among four patients who developed HZ, two had absolute CD3+CD4+ counts below the LLN, and one had a deficiency of NK cells.
According to the literature, detection of VZV memory T cells is usually possible by 9 to 12 months after HCT, while VZV recurrence correlates significantly with their deficiency [28].
The potential clinical efficacy of VZV subunit vaccines containing glycoprotein E in HCT recipients is related to driving VZV-specific CD4+ and CD8+ T-cell reconstitution [4]. Therefore, having a CD4+ T-cell count ≥200 cells/μL may be necessary for successful vaccination [4].
An insufficient count of NK cells may also have great importance in the susceptibility to HZ. Nonspecific antiviral immunity, especially via IFN-α and granulysin made by NK cells, has direct antiviral activity against VZV and enhances the early destruction of VZV-infected cells [28].
In our analysis, we used serological testing to check post-vaccination responses, aware that no data for immunocompromised patients could guide cut-offs for positive antibody titers. The serological post-vaccination response was confirmed in 12 (57%) recipients, including 4 who developed overt disease despite vaccinations. Three of these four patients initially had lymphoid malignancies before transplantation, and the fourth had been treated with rituximab after allo-HSCT (due to pure red cell aplasia). According to the literature, patients with B-cell malignancies are particularly vulnerable to total and/or functional post-transplant hypogammaglobulinemia, which results from disease-related effects and treatment-related side effects [27,30]. Functional immunoglobulin deficiencies in these recipients may play a role in the expected efficacy of vaccinations in post-transplant care. However, results of a prospective trial by Jotschke et al. suggests that patients with hematological malignancies with insufficient humoral responses might still benefit from vaccinations through cellular responses (regarding the SARS-CoV-2 vaccine) [35]. The importance of cellular response to vaccinations following allo-HSCT requires further investigations.
It is worth mentioning that four vaccinated patients with cGvHD did not develop clinical zoster disease. They were in the chronic phase, on stable, partially reduced doses of immunosuppressive therapy, and all had regenerated lymphocyte subpopulations.
Due to the small group of recipients (RZV was not reimbursed for allo-HSCT recipients in Poland at that time) and the short follow-up period, our results are preliminary. Still, they may contribute to the discussion around the validity and effectiveness of vaccinations against VZV in these SID patients.
5. Conclusions
Herpes zoster is a common complication after allo-HSCT and occurs in over 30% of recipients, mainly in the late period after transplantation after completion of acyclovir prophylaxis. The preliminary results indicate that RZV vaccination after allo-HSCT was safe and more than 80% effective at preventing HZ, but some vaccinated individuals did experience HZ.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Orenstein W.A. Offit P.A. Edwards K.M. Plotkin S.A. Plotkin’s Vaccines 8th ed.Elsevier Amsterdam, The Netherlands 2022 Hardback ISBN: 9780323790581, table Chapter 63 Varicella Vaccines 12151250
- 2Patel S.Y. Carbone J. Jolles S. The Expanding Field of Secondary Antibody Deficiency: Causes, Diagnosis, and Management Front. Immunol.2019103310.3389/fimmu.2019.0003330800120 PMC 6376447 · doi ↗ · pubmed ↗
- 3Jones D. Como C.N. Jing L. Blackmon A. Neff C.P. Krueger O. Bubak A.N. Palmer B.E. Koelle D.M. Nagel M.A. Varicella zoster virus productively infects human peripheral blood mononuclear cells to modulate expression of immunoinhibitory proteins and blocking PD-L 1 enhances virus-specific CD 8+ T cell effector function Plo S Pathog.201915 e 100765010.1371/journal.ppat.100765030870532 PMC 6435197 · doi ↗ · pubmed ↗
- 4Lee C.J. Savani B.N. Ljungman P. Varicella Zoster Virus Reactivation in Adult Survivors of Hematopoietic Cell Transplantation: How Do We Best Protect Our Patients?Biol. Blood Marrow Transplant.2018241783178710.1016/j.bbmt.2018.04.00329653205 · doi ↗ · pubmed ↗
- 5Bastidas A. de la Serna J. El Idrissi M. Oostvogels L. Quittet P. López-Jiménez J. Vural F. Pohlreich D. Zuckerman T. Issa N.C. ZOE-HSCT Study Group Collaborators. Effect of Recombinant Zoster Vaccine on Incidence of Herpes Zoster After Autologous Stem Cell Transplantation: A Randomized Clinical Trial JAMA 2019322123133 Erratum in JAMA 2019, 322, 78510.1001/jama.2019.905331287523 PMC 6618796 · doi ↗ · pubmed ↗
- 6Curran D. Matthews S. Rowley S.D. Young J.-A.H. Bastidas A. Anagnostopoulos A. Barista I. Chandrasekar P.H. Dickinson M. El Idrissi M. ZOE-HSCT Study group collaborators. Recombinant Zoster Vaccine Significantly Reduces the Impact on Quality of Life Caused by Herpes Zoster in Adult Autologous Hematopoietic Stem Cell Transplant Recipients: A Randomized Placebo-Controlled Trial (ZOE-HSCT)Biol. Blood Marrow Transplant.2019252474248110.1016/j.bbmt.2019.07.03631394276 · doi ↗ · pubmed ↗
- 7Christopeit M. Schmidt-Hieber M. Sprute R. Buchheidt D. Hentrich M. Karthaus M. Penack O. Ruhnke M. Weissinger F. Cornely O.A. Prophylaxis, diagnosis and therapy of infections in patients undergoing high-dose chemotherapy and autologous haematopoietic stem cell transplantation. 2020 update of the recommendations of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Medical Oncology (DGHO)Ann. Hematol.202110032133610.1007/s 00277-020-04297-833079221 PMC 7572248 · doi ↗ · pubmed ↗
- 8Reynolds G. Hall V.G. Teh B.W. Vaccine schedule recommendations and updates for patients with hematologic malignancy post-hematopoietic cell transplant or CAR T-cell therapy Transpl. Infect. Dis.202325(Suppl. S 1)e 1410910.1111/tid.1410937515788 PMC 10909447 · doi ↗ · pubmed ↗