Accuracy of Accuhaler, Ellipta, and Turbuhaler Testers in Patients with Chronic Obstructive Pulmonary Disease
Narongkorn Saiphoklang, Thiravit Siriyothipun, Sarawut Panichaporn

TL;DR
This study compares the accuracy of three inhaler testers in COPD patients and finds that they are reliable alternatives to a standard device.
Contribution
The study evaluates the accuracy of Accuhaler, Ellipta, and Turbuhaler testers in COPD patients compared to the In-Check DIAL®.
Findings
The Accuhaler tester showed the highest prevalence of optimal PIFR at 78%.
All three testers demonstrated excellent accuracy in detecting minimum PIFR.
The Turbuhaler had the lowest accuracy for optimal PIFR at 56.1%.
Abstract
Background: Peak inspiratory flow rate (PIFR) measurement is an essential tool for assessing the effectiveness of inhaler therapy in chronic obstructive pulmonary disease (COPD). This study aimed to evaluate the accuracy of three different inhaler testers compared to the In-Check DIAL® device. Methods: A cross-sectional study was conducted in clinically stable COPD patients. Participants performed PIFR measurements using the In-Check DIAL® device and three inhaler testers (Accuhaler, Ellipta, and Turbuhaler). Optimal PIFR was defined as ≥60 L/min. Minimum PIFR was defined as ≥30 L/min. Results: A total of 82 COPD patients (93.9% male) were included, with a mean age of 73.3 ± 8.8 years. Post-bronchodilator forced expiratory volume in one second was 69.2 ± 21.0%. The prevalence of optimal PIFR was 78%, 74%, and 52% for the Accuhaler, Ellipta, and Turbuhaler testers, respectively. For…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
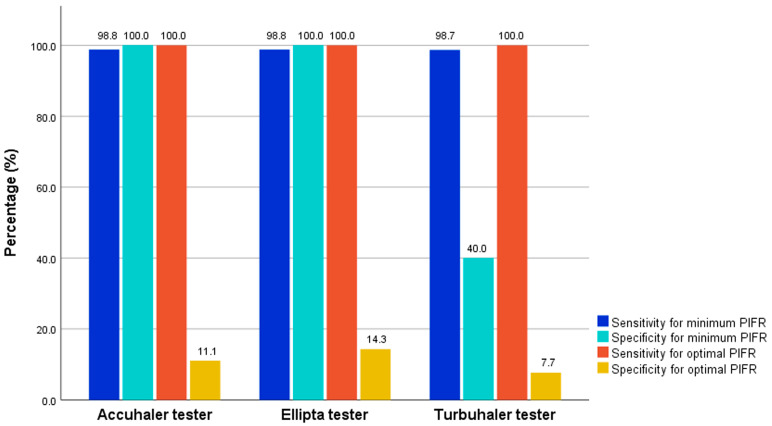 Figure 1
Figure 1- —Faculty of Medicine, Thammasat University, Thailand
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInhalation and Respiratory Drug Delivery · Chronic Obstructive Pulmonary Disease (COPD) Research · Phonocardiography and Auscultation Techniques
1. Introduction
Chronic obstructive pulmonary disease (COPD) has emerged as a key global health problem. It ranks as the third leading cause of death globally, following ischemic heart disease and cerebrovascular disease [1]. While COPD remains incurable, symptoms can be managed and exacerbations reduced by not smoking, avoiding pollution, and using appropriate medication. Inhaled medications are the cornerstone of COPD treatment according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) [2]. The mainstay medications are long-acting beta-2 agonists (LABAs), long-acting muscarinic antagonists (LAMAs), and inhaled corticosteroids (ICSs). These medications are delivered through pressurized metered dose inhalers (pMDIs), soft mist inhalers (SMIs), or dry powder inhalers (DPIs). Device selection should consider not only the appropriate medication but also the patient’s ability to generate adequate inspiratory flow.
The optimal peak inspiratory flow rate (PIFR) is the maximal flow generated during a forced inspiratory maneuver, which is crucial for optimizing the DPI effectiveness in COPD patients [3,4]. Suboptimal PIFR (≤60 L/min) is common during acute exacerbation of COPD and predicts all-cause and COPD-related readmissions [5]. Patients with suboptimal PIFR who are discharged on nebulizers have significantly lower rates of COPD readmission compared to those discharged on DPIs [5].
Optimal PIFR requirements vary across different DPI devices. The Accuhaler tester requires a minimal flow of 30 L/min and operates optimally at 60 L/min, which significantly improves drug delivery and fine particle generation [4,6,7]. Similarly, the Turbuhaler tester requires a minimum of 30 L/min and performs optimally at 60 L/min, with drug delivery strongly correlating with flow rate [4,7,8]. The Ellipta tester, a medium-resistance device, delivers adequate drug output at standardized flow rates of ≥30 L/min and performs optimally at 60 L/min for both single and combination agents [4,9,10].
The In-Check DIAL^®^ device is considered the gold standard for measuring PIFR [11]. However, its use is limited due to a lack of familiarity and availability among general practitioners [12]. Selecting appropriate inhaler devices based on patients’ PIFR has the potential to improve treatment outcomes in obstructive airway diseases, especially when using more accessible testing devices [13]. Inhaler testers may serve as alternative tools for assessing inspiratory force for COPD patients. Therefore, the purpose of this study was to evaluate the accuracy of three inhaler testers—Accuhaler, Ellipta, and Turbuhaler—compared to the In-Check DIAL^®^ device in COPD patients.
2. Materials and Methods
2.1. Study Design and Participants
Between March 2024 and December 2024, a cross-sectional study was undertaken at the pulmonary outpatient department of Thammasat University Hospital in Thailand. The inclusion criteria were (1) patients aged 40 years or older; (2) a smoking history of 10 pack-years or more; and (3) a diagnosis of COPD confirmed by a post-bronchodilator (BD) forced expiratory volume in one second (FEV_1_) to forced vital capacity (FVC) ratio of less than 0.7. The exclusion criteria were (1) COPD exacerbation within 3 months prior to study recruitment; (2) the presence of other pulmonary diseases, such as asthma, bronchiectasis, or pulmonary fibrosis; (3) a history of stroke with upper limb weakness or paresis; (4) any conditions or medications causing muscle weakness; (5) inability to perform testing with inhaler testers or In-Check DIAL^®^; (6) tracheostomy or the need for home ventilator support (both invasive and non-invasive); and (7) inability to communication or follow to instructions.
Ethics approval was obtained from the Human Research Ethics Committee of Thammasat University (Medicine), Thailand (IRB No. MTU-EC-IM-0-016/67, COA No.095/2024, date of approval: 28 March 2024), in full compliance with international guidelines, including the Declaration of Helsinki, the Belmont Report, CIOMS Guidelines, and the International Conference on Harmonization Good Clinical Practice (ICH-GCP). All methods were performed in accordance with these guidelines and regulations. Written informed consent was obtained from all participants. This study was registered on ClinicalTrials.gov with the number NCT06346678.
2.2. Study Procedures
Demographic data, respiratory symptoms, and functional capacity (assessed using the modified Medical Research Council (mMRC) dyspnea scale [14] and the COPD Assessment Test (CAT) [15]), as well as spirometry data from the past 12 months, were collected. Baseline medications, including short-acting bronchodilator (SABD), ICS, LABA, and LAMA, were also recorded.
The severity of COPD, according to the GOLD classification, was determined using the post-BD FEV_1_ value: Grade 1 represented mild (≥80% of predicted value); Grade 2 was moderate (50–79%); and Grades 3 and 4 represented severe (<50%) and very severe (<30%) impairment, respectively [2]. Based on symptom burden and exacerbation history, patients were categorized into Groups A, B, and E [2].
PIFR was measured using the In-Check DIAL^®^ device, as well as the Accuhaler, Ellipta, and Turbuhaler testers. Each device was tested three times with one-minute intervals between the tests, and the highest value was recorded. The testing sequence was randomized according to six different orders: (1) Accuhaler–Ellipta–Turbuhaler; (2) Turbuhaler–Ellipta–Accuhaler; (3) Ellipta–Accuhaler–Turbuhaler; (4) Ellipta–Turbuhaler–Accuhaler; (5) Turbuhaler–Accuhaler–Ellipta; or (6) Accuhaler–Turbuhaler–Ellipta. For each sequence, the In-Check DIAL^®^ resistance was adjusted to match the corresponding tester device before testing with that device.
2.3. Outcomes
The primary outcomes were the accuracy, sensitivity, and specificity of the three inhaler testers in identifying optimal PIFR compared to the In-Check DIAL^®^ device. The secondary outcomes included the prevalence rates of optimal, suboptimal, minimum, and insufficient PIFR. Additionally, factors associated with suboptimal PIFR were also considered secondary outcomes.
PIFR classifications were based on PIFR values [4,7,16,17]: optimal PIFR (≥60 L/min), suboptimal PIFR (<60 L/min), minimum PIFR (≥30 L/min), and insufficient PIFR (<30 L/min).
2.4. Statistical Analysis
The accuracy of inhaler testers in COPD patients has not been investigated. A study by Manuyakorn W et al. [18] reported the Accuhaler tester having a sensitivity of 95.4% in adolescents with asthma. We hypothesized that the sensitivity of the Accuhaler tester in COPD patients would be 85%. A sample size of 80 was proposed to achieve an alpha of 0.03 and a power of 0.86.
Descriptive statistics are presented as numbers (%) and mean ± standard deviation. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were reported. The chi-squared test was used to compare categorical variables between the optimal and suboptimal PIFR groups. The independent t-test or Mann–Whitney U test was used to compare continuous variables between the two groups. Statistical analyses were conducted using SPSS software (version 25.0; IBM Corp., Armonk, NY, USA), and a two-sided p-value of <0.05 was considered statistically significant.
3. Results
3.1. Participants
Eighty-two COPD patients (93.9% male) were included, with a mean age of 73.3 ± 8.8 years. Common comorbidities included hypertension (61.0%), dyslipidemia (47.6%), and diabetes mellitus (20.7%). COPD Grade 2 and a higher proportion of Group E were commonly observed (40.2% and 40.3%, respectively). Triple inhalation therapy (ICS/LABA/LAMA) was the most frequent maintenance treatment (48.8%). The CAT scores were 9.1 ± 5.7, and the mMRC scores were 1.5 ± 1.1. Post-BD FEV_1_ was 69.2 ± 21.0% (Table 1).
3.2. Primary Outcomes
For detecting optimal PIFR, the Accuhaler, Ellipta, and Turbuhaler testers demonstrated accuracies of 80.5%, 78.1%, and 56.1%, respectively. All inhaler testers exhibited 100% sensitivity but low specificity (11.1%, 14.3%, and 7.7% for the Accuhaler, Ellipta, and Turbuhaler testers, respectively) (Table 2 and Figure 1). However, the accuracy and specificity of the Accuhaler, Ellipta, and Turbuhaler testers were higher when detecting minimum PIFR (Table 2).
3.3. Secondary Outcomes
The prevalence rates of optimal, suboptimal, minimum, and insufficient PIFR were as follows: for Accuhaler, 78.0%, 20.7%, 98.8%, and 1.2%, respectively; for Ellipta, 74.4%, 25.6%, 97.6%, and 2.4%; and for Turbuhaler, 52.4%, 47.6%, 93.9%, and 6.1%, respectively (Table 3).
For the Accuhaler tester, the factors associated with suboptimal PIFR included older age, lower body weight, a higher proportion of coronary artery disease, and higher CAT and mMRC scores. For the Ellipta tester, factors included older age, lower body weight and height, a higher amount of smoking, a higher proportion of atrial fibrillation, higher CAT and mMRC scores, a higher proportion of GOLD Group E, and a higher proportion of SABD use. For the Turbuhaler tester, factors included older age, lower body weight, height, and body mass index, lower FVC, higher CAT and mMRC scores, a higher proportion of GOLD Group E, and a higher proportion of SABD use (Table 4).
4. Discussion
This is the first study to evaluate three inhaler testers compared to the In-Check DIAL^®^ device for PIFR measurement in COPD patients. Our findings revealed that all testers exhibited very high sensitivity and NPV (100%) but low specificity for optimal PIFR (7.7–14.3%). The accuracy of the Accuhaler and Ellipta testers (80.5% and 78.1%, respectively) was superior to that of the Turbuhaler tester (56.1%). The high sensitivity and NPV indicate that all the testers can be used for selecting an appropriate DPI for COPD patients. Although their low specificity indicates a tendency to produce false positives, the testers remain useful for minimizing inappropriate exclusion of patients from DPI therapy. Overall, the testers’ high sensitivity but low specificity suggests they are better suited as screening tools than replacements for the In-Check DIAL^®^ device.
Minimum PIFR detection (≥30 L/min) for all the inhaler testers is a remarkable finding in our study. The Accuhaler and Ellipta testers demonstrated identical superior accuracy (98.8%) with perfect specificity (100%) and excellent sensitivity (98.8%). With strong PPVs (100%), these testers can effectively identify patients capable of using a DPI device. The Turbuhaler tester also showed excellent accuracy (95.1%) and high sensitivity (98.7%) despite having low specificity (40.0%). These minimum PIFR detection outcomes are beneficial for selecting DPI devices to deliver inhaled medication to the lungs, thereby improving treatment effectiveness. Based on these findings, these testers may be most useful for identifying patients with insufficient inspiratory force, although their PIFR may not necessarily be optimal.
Interestingly, our findings in the COPD study correspond to those of Manuyakorn W et al. [18] in asthmatic children and adolescents, despite differences in disease pathophysiology and patient age. The Accuhaler and Turbuhaler testers in their study showed slightly lower sensitivity than ours for identifying optimal PIFR (97% vs. 100% for Accuhaler and 98% vs. 100% for Turbuhaler). These findings suggest that the Accuhaler and Turbuhaler testers can be effectively used across patients with different baseline diseases and characteristics. However, the detection of suboptimal PIFR in our COPD patients (22.0% and 47.6% for Accuhaler and Turbuhaler, respectively) was significantly higher than in asthmatic children and adolescents (0% and 0–10% for Accuhaler and Turbuhaler, respectively). This highlights the importance of measuring PIFR before selecting DPIs in COPD patients.
A study by Melani AS et al. [19], which involved 644 patients, including those with asthma and COPD, assessed PIFR using the Diskus (Accuhaler) inhaler with the In-Check DIAL^®^ device. It was found that 60% of patients with initially weak inhalation efforts had a PIFR below 30 L/min. However, after a brief instructional session emphasizing the need for more forceful inhalation, all patients achieved a PIFR of at least 30 L/min, indicating that proper technique can significantly improve inhaler performance. In contrast, when using the Turbuhaler tester, 77% demonstrated a PIF < 30 L/min. After counseling, 12% of patients still did not achieve a PIFR of at least 30 L/min.
In a study of 101 adult asthma patients by Engel T et al. [20], PIFR was measured both with and without the Turbuhaler device. While PIFR using the Turbuhaler tester was significantly lower than without it, only 4% of patients had a PIFR below 30 L/min, which is considered the minimum for effective drug delivery. This suggests that most patients can generate sufficient inspiratory flow using Turbuhaler. Another study by Brown P.H. assessed PIFR in 99 adults presenting with acute asthma exacerbations [21]. It was found that 98% of patients achieved a PIFR of at least 30 L/min using the Turbuhaler device, even before bronchodilator treatment, indicating that the majority could effectively use the device during acute episodes.
A randomized cross-over trial by Altman P et al. [22] compared PIFR among COPD patients using the Ellipta, Breezhaler, and HandiHaler devices. The study found that the mean PIFR achieved with the Ellipta inhaler was 78 L/min, which was higher than that with HandiHaler (49 L/min) but lower than with Breezhaler (108 L/min). This suggests that the Ellipta inhaler requires a moderate level of inspiratory effort, making it suitable for many COPD patients. These studies underscore the importance of assessing inspiratory flow rates when selecting an appropriate inhaler device for patients, as well as the potential benefits of patient education on inhaler technique to ensure effective drug delivery. Based on our study findings, if a patient’s test result is positive using the Accuhaler or Ellipta tester, it can be reasonably assumed that the patient has an optimal PIFR, as both devices demonstrated relatively high PPVs (80% and 77.2%, respectively). In contrast, the Turbuhaler tester showed a PPV of 54.4%, indicating a higher likelihood of false-positive results. In such cases, the In-Check DIAL^®^ device is needed to confirm optimal PIFR. However, if testing with any of these testers yields negative results, it can be reliably concluded that the patient cannot generate a flow of at least 60 L/min for optimal PIFR, as all three testers demonstrated strong NPVs.
Our study found that 22%, 25.6%, and 47.6% of patients had suboptimal PIFR using the Accuhaler, Ellipta, and Turbuhaler testers, respectively. These findings are consistent with previous studies, which reported suboptimal PIFR ranging from 20.1% to 78% [5,23,24,25,26,27]. Insufficient PIFR (<30 L/min) was identified in only 1.2% to 6.1% of patients in our study, indicating that most stable COPD patients can generate the minimum required inspiratory flow for DPI use. These results support the use of DPI devices in COPD therapy. Therefore, if treatment effectiveness remains inadequate during DPI use, inspiratory flow testing should be performed to evaluate whether the device is suitable for the patient.
The factors associated with suboptimal PIFR in our COPD patients included older age, lower body weight, height, and body mass index, a higher smoking history, higher proportions of coronary artery disease and atrial fibrillation, and higher CAT and mMRC scores. Other factors included a higher proportion of GOLD Group E, lower FVC, and a higher proportion of SABD use. In a study by Suriyakul A et al. [26], hand grip strength, age, height, and FVC were identified as predictors for Accuhaler PIFR, while hand grip strength, female gender, age, and FVC were predictors for Turbuhaler PIFR in COPD patients. Represas-Represas C et al. [23] found that age and FVC were significantly associated with suboptimal PIFR in stable COPD patients. Additionally, a study by Duarte AG et al. [28] showed that PIFR correlated with inspiratory capacity (r = 0.40, p < 0.0001) and the ratio of residual volume to total lung capacity (r = −0.19, p = 0.002), indicating that air trapping impacts PIFR in COPD patients. Our study suggests that older age, lower body mass index, higher respiratory symptoms, a history of COPD exacerbation, frequent rescue SABD use, presence of heart disease, and lower lung function were associated with lower PIFR values. These predictors could be useful for physicians when selecting the appropriate inhaler devices for individual patients. They also suggest that physicians should consider measuring PIFR before prescribing medications with DPI devices to maximize drug delivery.
This study has a few limitations. Firstly, the findings might not be applicable to the broader population of individuals with COPD, as this was a single-center study that excluded patients with recent exacerbation or significant comorbidities. Additionally, the sample was predominantly male (94%), and potential order effects—such as learning or fatigue—may have influenced the outcomes. Secondly, although the testing sequence was randomized to minimize assessment bias, patient fatigue and learning effects may have influenced the results. Multicenter studies are needed to validate the inhaler tests in heterogeneous COPD cohorts and evaluate PIFR-guided device selection.
5. Conclusions
The majority of COPD patients achieved optimal PIFR across different devices, with the Accuhaler tester showing the highest prevalence. Several factors were associated with suboptimal PIFR. All three inhaler testers demonstrated excellent accuracy in assessing PIFR in COPD patients, indicating their potential as reliable alternatives to the In-Check DIAL^®^ device in clinical practice. However, the testers’ high sensitivity but low specificity suggests they are better suited as screening tools than replacements for the In-Check DIAL^®^ device. These findings suggest that these devices could be effectively integrated into routine clinical assessments for managing COPD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Chronic Obstructive Pulmonary Disease (COPD)Available online: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd)(accessed on 1 November 2023)
- 2Global Initiative for Chronic Obstructive Lung Disease Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease 2023 Report Available online: https://goldcopd.org/2023-gold-report-2/(accessed on 1 November 2023)
- 3Laube B.L. Janssens H.M. de Jongh F.H. Devadason S.G. Dhand R. Diot P. Everard M.L. Horvath I. Navalesi P. Voshaar T. What the pulmonary specialist should know about the new inhalation therapies Eur. Respir. J.2011371308133110.1183/09031936.0016641021310878 · doi ↗ · pubmed ↗
- 4Ghosh S. Ohar J.A. Drummond M.B. Peak inspiratory flow rate in chronic obstructive pulmonary disease: Implications for dry powder inhalers J. Aerosol Med. Pulm. Drug Deliv.20173038138710.1089/jamp.2017.141628933581 PMC 5915227 · doi ↗ · pubmed ↗
- 5Loh C.H. Peters S.P. Lovings T.M. Ohar J.A. Suboptimal inspiratory flow rates are associated with chronic obstructive pulmonary disease and all-cause readmissions Ann. Am. Thorac. Soc.2017141305131110.1513/Annals ATS.201611-903OC 28406710 · doi ↗ · pubmed ↗
- 6Kamin W.E. Genz T. Roeder S. Scheuch G. Trammer T. Juenemann R. Cloes R.M. Mass output and particle size distribution of glucocorticosteroids emitted from different inhalation devices depending on various inspiratory parameters J. Aerosol Med.200215657310.1089/0894268025290859312006147 · doi ↗ · pubmed ↗
- 7Haidl P. Heindl S. Siemon K. Bernacka M. Cloes R.M. Inhalation device requirements for patients’ inhalation maneuvers Respir. Med.2016118657510.1016/j.rmed.2016.07.01327578473 · doi ↗ · pubmed ↗
- 8Abdelrahim M.E. Assi K.H. Chrystyn H. Dose emission and aerodynamic characterization of the terbutaline sulphate dose emitted from a Turbuhaler at low inhalation flow Pharm. Dev. Technol.20131894494910.3109/10837450.2011.62097021981637 · doi ↗ · pubmed ↗