Lipidomic profiling of the cerebrospinal fluid in moyamoya angiopathy patients
Antonella Potenza, Gemma Gorla, Tatiana Carrozzini, Giuliana Pollaci, Michele Dei Cas, Francesco Acerbi, Ignazio G. Vetrano, Paolo Ferroli, Isabella Canavero, Rita Paroni, Nicola Rifino, Anna Bersano, Laura Gatti

TL;DR
This study identifies specific lipid changes in cerebrospinal fluid of moyamoya angiopathy patients, suggesting potential biomarkers for diagnosis and understanding disease mechanisms.
Contribution
The study provides novel lipidomic profiling of CSF in moyamoya angiopathy patients, identifying potential biomarkers and revealing a pro-inflammatory environment.
Findings
Sphingolipids and phospholipids are significantly increased in CSF of moyamoya patients.
Monoacylglycerols are markedly decreased in CSF of moyamoya patients compared to controls.
Phosphatidylcholines are commonly decreased in plasma but increased in CSF of moyamoya patients.
Abstract
Moyamoya angiopathy (MA) is a rare cerebrovascular disorder which can occur in both children and young adults, characterized by progressive occlusion of the intracranial carotid arteries, leading patients to ischemic and haemorrhagic strokes. Despite decades of research, the mechanisms underlying MA remain poorly clarified and current gaps in the understanding of pathogenesis have hampered the development of suitable preventive strategies and therapeutic options. Moreover, clinically approved biomarkers for MA patients’ stratification are missing. The unknown pathophysiology and the lack of reliable biomarkers prompted us to investigate cerebrospinal fluid (CSF) lipidome through state-of-the-art lipidomics. Intraoperative CSF from a subgroup of MA patients in comparison to age/sex matched controls (CTRL) was analysed through LC–MS/MS, by an untargeted lipidomic approach. Receiver…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
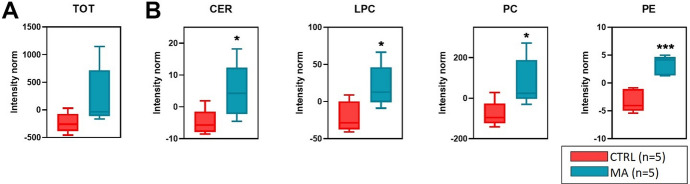 Figure 1
Figure 1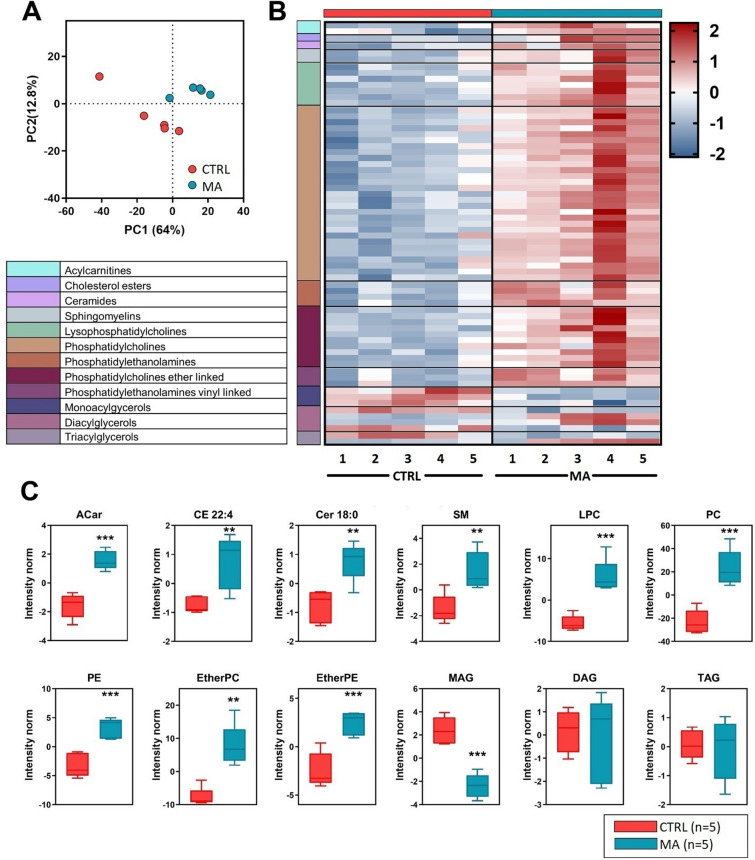 Figure 2
Figure 2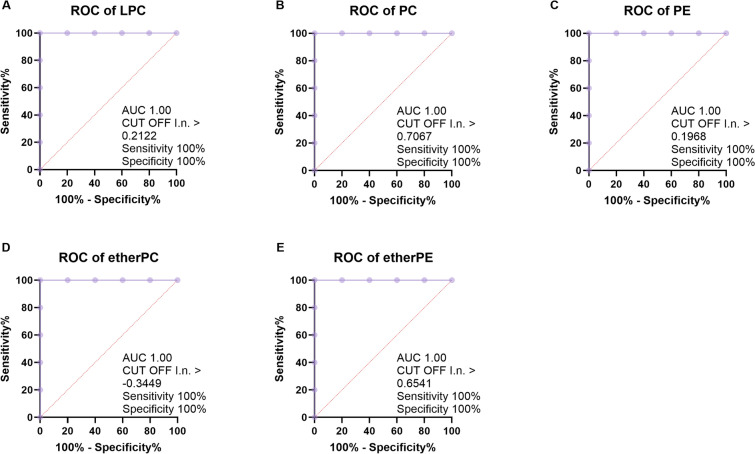 Figure 3
Figure 3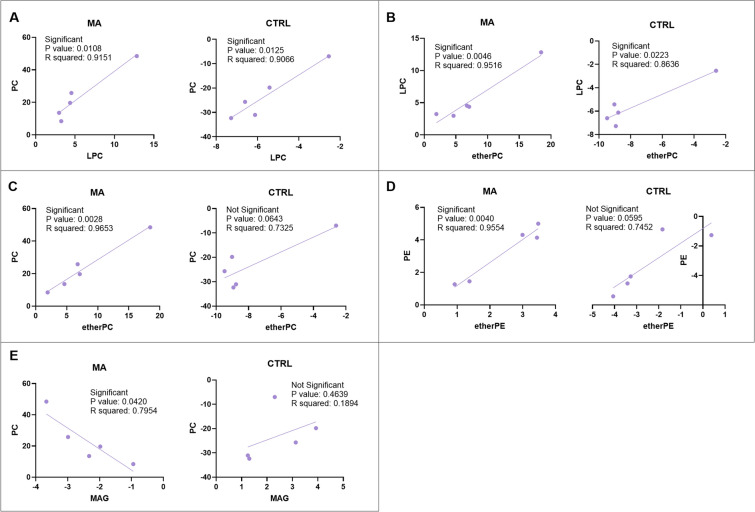 Figure 4
Figure 4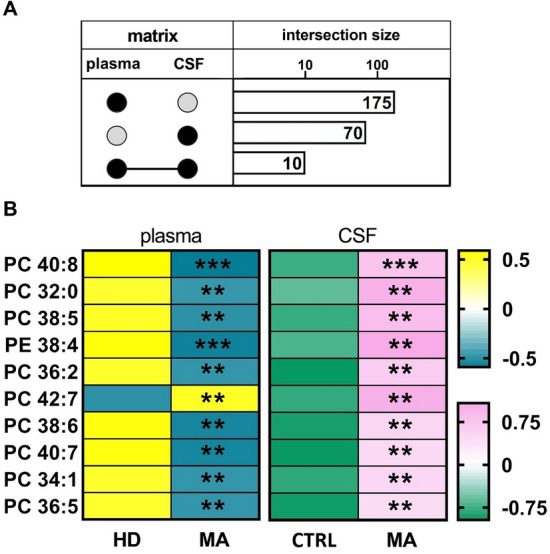 Figure 5
Figure 5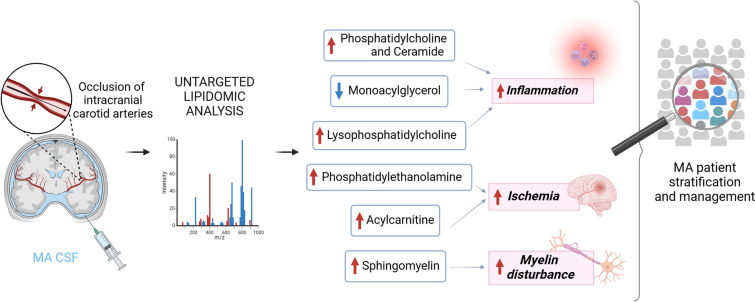 Figure 6
Figure 6- —http://dx.doi.org/10.13039/501100003196Ministero della Salute
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMoyamoya disease diagnosis and treatment · Intracranial Aneurysms: Treatment and Complications · Neurological Complications and Syndromes
Background
Moyamoya angiopathy (MA) is an uncommon non-atherosclerotic cerebrovascular disease, characterized by progressive stenosis of the terminal internal carotid artery and its proximal branches, and formation of hazy collateral vessels at the base of the brain. The main clinical manifestations of MA are recurrent ischemic or haemorrhagic strokes and cognitive impairment, which can occur in both children and young adults [1–3]. Despite decades of research, the etiology and pathophysiological mechanisms underlying MA remain poorly clarified. Previous studies have highlighted the potential involvement of inflammation as a cause or progressive factor of MA, although the role of inflammation has not been rigorously explored [4, 5]. Inflammatory processes have been suggested to instigate or exacerbate this rare condition, particularly in pediatric patients [6]. MA is also emerging as an immune-related angiopathy, since an increasing number of reports describes the development of MA associated with infection or autoimmune disorders [7, 8]. Several studies have identified a variety of autoimmune diseases associated to MA [9, 10]. Besides, recent reports suggested that a more aggressive MA course is associated with the presence of thyroid autoantibodies [11]. Together, this growing body of molecular and clinical evidence points towards immune-related responses as second hits to trigger MA onset and may hint at therapeutic opportunities.
Current gaps in the understanding of disease pathogenesis have hampered the development of suitable preventive strategies and therapeutic options. Surgical revascularization, including superficial temporal artery (STA) to middle cerebral artery bypass (MCA), has been proven as an effective treatment to prevent subsequent strokes of MA patients [12]. The prevalence of MA varies widely among ethnic groups, thus genetic factors have been implicated in disease development [13, 14]. Specifically, a high prevalence of MA patients has been reported among the descendants belonging to East Asian countries, of whom the three most common are Japan, Korea and China. The estimated prevalence of MA in Japan is 10.5/100,000 individuals and the incidence rate is 0.94/100,000; conversely, the incidence rate is almost 10-fold lower accounting for 0.09/100,000 individuals in Western regions, including North America [15]. Additionally, the incidence of MA in female subjects has been reported to be higher than that in males. Furthermore, a bimodal age distribution has been described is MA patients, referring to a highest peak observed at 45–49 years and a smaller peak observed at 5–9 years [16]. The main susceptibility gene variant identified in East Asian patients encodes for the ubiquitin-ligase Ring Finger Protein 213 (RNF213) [17]. So far, no animal or cellular preclinical model accurately recapitulates the pathological changes observed in vascular intimal hyperplasia of MA patients [18]. Moreover, there are no clinically approved biomarkers for distinguishing among the different subtypes of MA.
The previous investigations aimed at biomarker discovery mainly addressed peripheral blood, which may not reflect the real pathological changes of MA cerebral vessels. Since the challenging sampling of cerebral artery specimens for transcriptomic studies, other ultrasensitive techniques were recently carried out for molecular profiling of circulating biomarkers [19–21]. In this regard, multi-omic approaches may turn out to be crucial in patients’ risk stratification and precision medicine, allowing for the selection and customization of medical treatment based on individual signatures [22]. Despite numerous findings in the proteomics and metabolomics field [23–27], very little is known about changes in the lipid composition in patients’ circulating fluids, although it has been already reported that RNF213 is involved in lipid metabolism [28]. Lipids are a significant part of the neural molecular environment, constituting approximately 50% of the dry weight of the brain [29]. They are essential for proper brain function, being required for axon growth and potentiation, membrane trafficking, myelin formation, synaptogenesis and accounting for critical components of cell membranes [30]. It is not surprising that changes that affect brain lipid metabolism and/or its delicate vascular network, have profound implications in tissue homeostasis and have been implicated as underlying mechanisms for many cerebrovascular diseases. The alterations in the MA vasculature induced by ischemic insult and oxygen deprivation can cause the loss of astrocytes and microglia, reduce neuronal function and increase neuroinflammation. These changes may be coupled with intense lipid remodeling in CSF, and affect also cholesterol metabolism, which is essential for neuronal growth and survival since they need cholesterol to repair and build more membranes.
Recently, a lipidomic analysis of cerebral arteries in MA and intracranial atherosclerotic disease patients identified distinct lipid species for distinguishing between the two conditions [31]. Our previous gene expression analyses of MA pathological cerebral vessels also underlined the relevance of specific biomarkers for patient’s stratification, as well as a novel potential therapeutic target for MA care [32]. However, the poor availability and difficulty in collecting arterial tissue specimens prompted us to search for valuable biomarkers in circulating fluids, mainly plasma and CSF. We previously performed an untargeted lipidomic analysis showing a cumulative depletion of lipid asset in plasma of MA as compared to healthy donors [33]. These promising but preliminary results encouraged us to investigate cerebrospinal fluid (CSF) as an alternative biomarker source. The identification of changes in metabolic profiles, providing valuable biomarkers and shedding light on mechanisms of diseases could have a crucial role in patients’ risk stratification and precision medicine, allowing for the selection and customization of medical treatment based on individual metabolic profiles. In this pilot study, we aimed to elucidate the MA CSF lipidome, by identifying altered lipids in a representative sample of a typical Caucasian MA population. We consider that a better understanding of specific lipid changes and their eventual correlation with clinical outcomes could help to guide patients’ stratification approaches, with a possible impact also in the prevention of MA evolution.
Methods
Cohort selection and sampling
This was an observational study conducted on MA patients, diagnosed following the literature criteria [34]. The full methodology of the study has been previously reported [35]. From the original population of 160 patients, consecutively enrolled between November 2014 and December 2022 at the Neurology IX Unit of the Fondazione IRCCS Istituto Neurologico “C. Besta” (Italy, Milan), a subgroup of five adult Caucasian patients was selected, exclusively based on CSF availability and demographic/clinical features typical of MA cohort. CSF samples were obtained after the neurological insult that determined the STA-MCA neurosurgical bypass, according to European Stroke Organisation (ESO) Guidelines on moyamoya angiopathy [36]. The study design was approved by the Ethics Committee of the Fondazione IRCCS Istituto Neurologico “C. Besta” of Milan (GEN-O-MA clinical study, report no. 12, 10/01/2014). Informed written consent for study participation and sample collection from all patients and controls were mandatory for study inclusion. Demographic and clinical characteristics, including cerebrovascular risk factors, were collected. MA was classified into bilateral or unilateral types as observed on conventional angiography. Diagnosis of ischemic or haemorrhagic stroke was confirmed by computerized tomography scan and magnetic resonance imaging. The MA severity was assessed by Suzuki and modified Rankin scale according to standard clinical practice and international guidelines [35–37]. A population of five adult Caucasian subjects admitted to our Institution and suffering from MA-unrelated hemodynamic insufficiency, secondary to arterial stenosis due to atherosclerotic diseases or due to isolated intracranial aneurysms, was collected as control group (CTRL). Control CSF was sampled during surgical procedure, in patients undergoing STA-MCA bypass for hemodynamic cerebrovascular insufficiency or a craniotomy to clip intracranial aneurysm in the anterior circulation, mostly MCA or anterior communicating artery. No further procedures apart from the surgical treatment were necessary to obtain CSF. A multidisciplinary team discussed surgical indications in all the patients, both MA and CTRL. CSF was collected from MA patients and CTRL subjects from cisternal spaces, mainly sylvian fissure, after arachnoid incision, in compliance with ethical regulations of ESO Guidelines on moyamoya angiopathy [36]. After collection, samples were briefly centrifuged to remove any cellular debris and stored in aliquots at − 80 °C. Twenty-four milliliters of peripheral blood were collected in tubes containing EDTA (Vacuette®, Preanalitica s.r.l., Caravaggio, Italy). Blood samples were analyzed for levels of triglycerides (TG), total cholesterol (CHOL) and high-density lipoprotein (HDL) CHOL by standard clinical laboratory methods; low-density lipoprotein (LDL) CHOL concentrations were estimated as CHOL—(HDL + TG/5). After 10 min at 200 g centrifugation, plasma was stored in aliquots at − 80 °C.
Chemicals and reagents
The chemicals acetonitrile, 2-propanol, methanol, chloroform, formic acid, ammonium acetate, ammonium formate and dibutylhydroxytoluene (BHT) were purchased from Sigma-Aldrich (St. Louis, MO, USA). All aqueous solutions were prepared using purified water at a Milli-Q grade (Burlington, MA, USA).
Untargeted lipidomics
CSF and plasma were diluted with water (1:2 CSF, 1:4 plasma v/v) and lipids were extracted by a mixture of methanol/chloroform (850 µL, 2:1, v/v). The samples were extracted with an oscillator thermo-mixer (60 min, 1000 rpm, 4 °C). After centrifugation (25 min at 13400 rpm), the organic phase was evaporated under a stream of nitrogen. The residues were dissolved in 100 µL of methanol + 0.1% BHT and withdrawn in a glass vial. Extraction and analysis performances were checked by the use of a preconstituted internal standards mix (Equisplash Lipidomix, 150 ng per sample, Avanti Polar, Alabaster, AL, USA). The extracts were analysed by LC-MS/MS consisting of a Shimadzu UPLC coupled with a Triple TOF 6600 Sciex (Concord, ON, CA) [33]. All samples were analyzed in duplicate in positive and negative electrospray ionization. Spectra were contemporarily acquired by full-mass scan from 200 to 1500 m/z and top-20 data-dependent acquisition from 50 to 1500 m/z. Declustering potential was fixed to 50 eV, and the collision energy was 35 ± 15 eV. The chromatographic separation was reached on a reverse-phase Acquity CSH C18 column 1.7 μm, 2.1 × 100 mm (Waters, Franklin, MA, USA) by a gradient between (A) water/acetonitrile (60:40) and (B) 2-propanol/acetonitrile (90:10), both containing 10 mM ammonium acetate and 0.1% of formic acid.
LC-HR-MS data processing
The spectra deconvolution, peak alignment, and sample normalization were attained using MS-DIAL [38]. MS and MS/MS tolerance for peak profile was set to 0.01 and 0.05 Da, respectively. Identification was achieved matching spectra with LipidBlast database or in-house built mass spectral library. Intensities of analytes were normalized by Lowless algorithm and those with a CV% superior to 30% in the QC pool sample were excluded. The lipid classes considered were acylcarnitines (ACar), cholesterol (chol), cholesterol esters (CE), monoacylglycerols (MAG), diacylglycerols (DAG), triacylglycerols (TAG); dihydroceramides (DHCer), ceramides (Cer), hexosylceramides (HexCer), lactosylceramides (LacCer), globotriaosylceramide (Gb3), sulfatides (SULF), gangliosides (GM3), sphingomyelins (SM), lysophosphatidylcholines (LPC), lysophosphatidylethanolamines (LPE), phosphatidylcholines (PC), phosphatidylethanolamines (PE), phosphatidylinositoles (PI) and plasmalogens – that are ether linked phosphatidylcholines (EtherPC) and vinyl linked phosphatidylethanolamines (EtherPE). The lipids are indicated throughout the paper by their total number of carbon atoms and degree of unsaturation (i.e. PC 40:2) or eventually specifying the acyl chains detected (i.e. PC 18:0/18:1). The study raw data supporting lipidomic reported results can be found in the public repository MetaboLights [39].
Statistical analyses
Graphs and statistical analyses were prepared with GraphPad Prism 8.0, and with MetaboAnalyst5.0 [40]. Statistical significance was evaluated by comparing ranks with non-parametric Mann-Whitney U test and Fisher’s exact test. Multivariate analysis partial least squares discriminant analysis (PLS-DA) was performed to increase the group separation and investigate the variables with a high Variance Importance in Projection score (VIP > 1.5). P <0.05 was considered statistically significant. P values are schematized as follows: * < 0.05; ** < 0.01; *** < 0.001. Data are shown as mean ± SD. To explore factors affecting the lipid composition within MA patients, receiver operating characteristic (ROC) curves and simple linear regression model were used. Sensitivity and specificity were defined to estimate the performances of the candidate lipid to discriminate between MA patients and CTRL. The authors were blinded to the experimental protocol while performing the experiments and the statistical calculations.
Results and discussion
Demographic characteristics of the study cohorts
According to the GEN-O-MA project and ESO Guidelines [35, 36], a small but representative subgroup of subjects was enrolled for the present study, since untargeted lipidomics requires a very homogeneous group that would allow identifying any potetial difference in lipidome profiles between MA patients and CTRL subjects. Specifically, we included five MA Caucasian patients, based on CSF availability and demographic/clinical features typical of our MA cohort (Caucasian, females, mean age of 47 years, bilateral MA presentation) [33, 41]. Of note, these characteristics are precisely representative of the whole MA population in Western countries, which is a relevant aspect considering the rarity of the disease [42]. We summarized MA patient information in Table 1, by reporting the mean age (± SD); Sex (female %); cerebrovascular disease (CVD) type (hemorrhagic stroke, ischemic stroke, transient ischemic attack TIA); National Institutes of Health Stroke Scale (0–5; 6–10); MA presentation (Unilateral or Bilateral); Suzuki grading (I–III; IV–VI); modified Rankin Scale (0–1; 2–3). The patients (100% females) had a mean age of 45.56 ± 4.2 years (range 38.8–49.6). The disease presented with a haemorrhagic stroke in 40% of patients, an ischemic event in 40% and a TIA in 20% of the cases. Five control patients (100 % females; mean age of 66.2 years, range 44.0–76.0) underwent conventional catheter digital subtraction angiography and morphological imaging by MRI, likewise MA patients. Computerized tomography scan and MRI showed an ischemic stroke in three controls out of five (corresponding to a percentage of 60%) and a TIA in one control subject out of five (corresponding to a percentage of 20%), representing patients with hemodynamic cerebrovascular impairment, deeply distinct and unrelated from MA. The hemorrhagic phenotype was reported in one control patient out of five (corresponding to a percentage of 20%), who exhibited an intracranial aneurysm with previous small bleeding (Table 1).Table 1. Participant characteristics^a^MACTRLP valueN55Mean age (y ± SD)45.56 ± 4.266.2 ± 12.770.095 (ns)Sex (% F)100%100%1 (ns)CVD typeHS40%20%1 (ns)IS40%60%1 (ns)TIA20%20%1 (ns)NIHSS0–580%na#6–1020%na#MA presentationU0%na#B100%na#Suzuki gradingI–III40%na#IV–VI60%na#mRS0–1100%100%1 (ns)2–300#CHOL (mg/dl)168.6217.70.571 (ns)TG (mg/dl)102.2176.30.589 (ns)HDL (mg/dl)40350.467 (ns)LDL (mg/dl)92.25920.999 (ns)^a^Demographic, clinical, and neuroradiological features of MA patients and control subjects. Statistical significance was evaluated by comparing ranks with Mann–Whitney U test or Fisher’s exact test. B, bilateral; CHOL, total cholesterol; CTRL, controls; CVD, cerebrovascular disease; F, female; HDL, high-density lipoprotein—cholesterol; HS, haemorrhagic stroke; IS, ischemic stroke; LDL, low-density lipoprotein—cholesterol; MA, moyamoya angiopathy; mRS, modified rankin scale; N, number of subjects; na, not available; NIHSS, national institutes of health stroke scale; ns, not significant; TIA, transient ischemic attack; TG, triglycerides; U, unilateral; y, years
No statistical difference has been evidenced when comparing peripheral blood lipid levels determined by standard clinical laboratory methods, in MA patients and CTRL (CHOL; HDL; LDL; TG; Table 1).
Increase of the overall lipid content in CSF of MA patients.
A total of n = 623 different lipids were identified and quantified in CSF from MA and CTRL populations, by an untargeted lipidomic approach. The overall CSF lipid content of MA patients was higher in comparison to CTRL, although not statistically significant (Fig. 1A).Fig. 1. Overall CSF lipid content. A Total CSF lipid content in MA patients and in CTRL subjects with unrelated cerebrovascular diseases B Lipid classes significantly increased in CSF of MA patients. Statistical significance is evaluated by comparing ranks with Mann–Whitney U test. P values are schematized as follows: * < 0.05; *** < 0.001
Among the most altered lipid categories, we found the sphingolipids (Ceramides, Cer) and phospholipids (i.e., LPC; PC; PE). In particular, we observed significant increases for Cer (*p *< 0.05), LPC (*p *< 0.05), PC (*p *< 0.05) and PE (p < 0.001; Fig. 1B) classes. A list of the main lipid classes emerging from our analysis was shown (Table 2). Of note, although characterized by a different time lapse (25 ± 13 months) between disease onset and CSF sampling during the neurosurgical procedure, the lipidome profile of our MA cohort is quite homogeneous (see Additional File 1). Moreover, when we performed appropriate statistical analyses (non-parametric Mann-Whitney U test), to evaluate the profile of specific CSF lipid classes/species in MA patients in relation to CVD type (HS vs IS/TIA), Suzuki grading (I–III vs. IV–VI) and NIHSS (0–5 vs. 6–10), we did not find any statistically significant difference between the analysed subgroups (see Additional Files 2, 3, 4).Table 2. Nomenclature of CSF lipid classes/species emerging from lipidomicsACarAcylcarnitinesMAGMonoacylglycerolsCer 18:0Ceramide 18:0LPCLysophosphatidylcholinesCE 22:4Cholesterol ester 22:4PCPhosphatidylcholinesDAGDiacylglycerolsPEPhosphatidylethanolaminesEther PCPhosphatidylcholine EthersSMSphingomyelinsEther PEPhosphatidylethanolamine EthersTAGTriacylglycerols^^Cer 18:0 and CE 22:4 were included in Table because were found as single lipid altered species of their respective lipid classes
Ceramides, beyond being an essential constituent of cytomembrane, play a key role as signaling mediators in many cell processes and stress responses. Interestingly, a marked relation has been documented between ceramides and cerebrovascular diseases [43]. PC act as principal components of cell membranes, playing a role in cell signalling and ameliorating neuronal damage under inflammatory stress, by re-establishing plasticity of neural stem cells [44, 45]. LPC, as well as PC, are bioactive compounds associated with oxidative stress and inflammatory processes, with a potential effect in preventing ischemic injury or neuronal death in patients with stroke [46, 47]. Interestingly, an untargeted metabolomic approach recently carried out has been able to identify a distinct metabolite expression, mostly dealing with LPC, in serum samples from MA patients when compared to controls [27]. Specifically, LPC 16:1-2 expression was found as significantly lower in ischaemic MA patients than in healthy controls. The LPC-enriched CSF lipid content reported in the present study might counterbalance the corresponding LPC depletion identified in plasma samples of the same MA cohort [33].
Differential lipid analysis
A PLS-DA was performed to identify deregulated lipids associated with MA (Fig. 2A). This analysis clearly separated MA patients and CTRL subjects by 64% on Principal Component 1 (PC1). The PC1 represents the new dimension in which the initial variables are compressed and depicts the maximum of the separation that can be reached within these clusters and variables. The Variance Importance in Projection (VIP) scores derived from PLS-DA were used for ranking the discriminating features, taking a cut-off value ≥ 1.5. Those lipid species (n = 70) with a VIP ≥ 1.5 that significantly contributed to the separation of MA patients and CTRL are visualized by a heatmap and ordered according to their lipid classes (Fig. 2B). Fig. 2C shows a univariate analysis with the twelve lipid classes displaying significant modulations due to the disease. Features exhibiting VIP ≥ 1.5 and variance p-value ≤ 0.05 were selected as significantly differentially abundant lipids. Of note, Cer 18:0 and CE 22:4 are the only VIP lipids found in their corresponding lipid classes (i.e., sphingolipids and neutral lipids), and therefore the boxes represent the trend of these single species.Fig. 2CSF untargeted lipidomics. CSF lipid alteration in MA patients (n = 5) in comparison to age and sex matched controls with unrelated cerebrovascular diseases (CTRL, n = 5). A Discriminant analysis (score plot) of the lipidome in MA and CTRL subjects. The axes are ranked according to their importance in the group discrimination. In the x-axis, component 1 (PC1, 64%) represents the maximum of the separation that can be reached within these clusters and variables, whereas, in the y-axis, component 2 (PC2, 12.8%) represents the direction that contains the most remaining variance. B Heatmap of the top 70 significantly altered lipid species highly correlated with the disease, chosen within those with a Variance Importance in Projection (VIP) score > 1.5, and ordered by lipid classes, coded by different colors. Each horizontal row represents a molecular lipid; each vertical column represents a sample. The concentrations were autoscaled and log- transformed for visualization. The color code bar indicates the log of the fold change of the mean concentration for a given lipid. The color-scale differentiates values as high (red), average (white) and low (blue). C VIP lipid classes concentrations in MA and CTRL subjects. Boxplots represent the trends in lipid class concentrations in MA and CTRL patients, except for Cer 18:0 and CE 22:4 which are the only VIP lipids found in their classes and therefore the boxes represent the trend of these single species. The boxes represent data obtained in the range 25th-75th percentile; the line across the boxes indicates the median value; the lines above and below the boxes indicate extreme values (10th or 90th percentile). Outliers are displayed as separate points. Statistical significance is evaluated by comparing ranks with Mann–Whitney U test. P values are schematized as follows: ** < 0.01; *** < 0.001
The high sphingolipid/phospholipid content as well as the finding of pro-inflammatory lipid classes were confirmed by PCA. By evaluating both multivariate and univariate analyses, it has been found a particular increase in many phospholipids (PC, PE, LPC, Ether PC and Ether PE) and in Acylcarnitines (ACar; *p *< 0.001). The increased levels of ACar among acute ischemic stroke patients indicate a major energy requirement due to a negative feedback from the brain hypoxic state [48]. ACar are also related to the recovery of stroke [49], and carnitines are associated with ischemic strokes [50]. Moreover, a previous targeted metabolomic approach suggested a biomarker pattern including ACar for differential diagnosis of acute ischemic stroke [51]. Higher plasma ACar levels were observed in individuals with an increased cardiovascular disease risk, as shown by a greater mitochondrial production of reactive oxygen species, which increase vascular inflammation [52]. Ether-PC and ether-PE contain high amounts of arachidonic acid required for the biosynthesis of eicosanoids, bioactive lipids with a great role in inflammation. In hypertensive patients, a deficiency in plasma ether lipids has been demonstrated, specifically in ether-PC and ether-PE [53]. Moreover, an accelerated PC turnover in macrophages promotes adipose tissue inflammation in obesity [54]. Additionally, the role of LPC in promoting the release of inflammatory factors has been described in a wide range of diseases [55], thus raising the hypothesis that LPC-targeting might be a valuable therapeutic approach for inflammation-related diseases, including MA. The observed Cer 18:0 increase is a worse condition in several neurological diseases, due to proinflammatory and neurodegenerative functions [56]. Increased plasma levels of Cer (18:0) and SM have been implicated in insulin resistance, whereas inflammation may contribute to its long-term maintenance, especially in models of obesity-induced insulin resistance [57]. SM is reported to be a biomarker of demyelination [58], which is coherent with the occurrence of a myelin damage, observed in the white matter of MA patients [59]. The impact of sphingolipids is evident in acute lung injury, or chronic lung pathologies such as cystic fibrosis and chronic obstructive pulmonary disease, where inflammation has a major role [60]. CE in the human brain are sequestered as lipid droplets, primarily used for the transport and storage of CHOL [61], a process occurring allosterically in response to surplus CHOL within the cell [62]. CE are increased in several neurological disorders such as multiple sclerosis, Alzheimer’s disease, brain injury, Huntington’s disease and stroke [63, 64]. Recently, a shotgun lipidomic analysis reported that CHOL was inefficiently converted to CE in the blood of cardiovascular disease patients [65]. Interestingly, endogenously generated lipid mediators (branched FA esters of hydroxy FA) promote the resolution of inflammation and attenuate the microvascular and macrovascular complications of obesity and diabetes mellitus in chronic kidney disease [66]. This evidence highlights novel opportunities for potential therapeutic intervention through the targeting of pro-resolution, rather than anti-inflammatory pathways.
MAG was the only lipid class displaying a markedly significant (p < 0.001) decrease in CSF of MA patients as compared to CTRL subjects (Fig. 2C). MAG is a neutral lipid that is degraded to glycerol and fatty acids by MAG-lipase (MAGL), a proinflammatory enzyme with highest expression in brain [67, 68], where it constitutes the major source of arachidonic acid and proinflammatory prostaglandins [69]. The marked decrease of MAG in MA CSF might result in induction of pro-inflammatory signals. Interestingly, MAGL inhibition protects against inflammation and lesions induced by ischaemia/reperfusion injury [70]. Accordingly, inhibition of MAGL has emerged as an anti-inflammatory and protective option in several experimental models of chronic inflammatory diseases, by a mechanism that relies on a shift of lipid metabolism in inflammatory cells [67].
ROC and simple linear regression analysis of lipid biomarkers
In order to determine whether these candidate CSF biomarkers could have any clinical utility as potential patient selection markers, we performed ROC curve and simple linear regression analysis for prospective follow-up and for diagnostic use. Twelve lipid classes showing significant alterations in CSF (i.e., with VIP ≥ 1.5) between MA and CTRL subjects were selected for individual ROC analysis. According to ROC analysis, 10 out of 12 classes proved to be candidate diagnostic biomarker, since they displayed high sensitivity and specificity performances (Table 3). All these 10 lipid classes presented area under the ROC curve (AUC) values higher than 0.9, and 7 out of 10 classes showed a perfect performance, by exhibiting an AUC = 1. Specifically, 5 out of 9 lipid classes showing a significant increase in MA patients belonged to the category of phospholipids (Table 3 and Fig. 3).Table 3ROC analysis of lipid biomarkers^a^Lipid classTrendAUCP valueCIACar**↑10.0091.000–1.000LPC↑10.0091.000–1.000PC↑10.0091.000–1.000PE↑10.0091.000–1.000EtherPC↑10.0091.000–1.000EtherPE↑10.0091.000–1.000MAG↓10.0091.000–1.000SM↑0.960.0160.843–1.000CE 22:4↑0.920.0280.739–1.000Cer 18:0↑0.930.0280.739–1.000DAG↑0.520.9170.122–0.918TAG↑0.520.9170.135–0.905^a^Main lipid classes selected for individual receiver operating characteristic (ROC) curve analysis. The trend described by the analysis has been defined as enhanced (↑) or decreased (↓**). P values and confidence interval (CI) values are reported. AUC, area under the ROC curve. Cer 18:0 and CE 22:4 are the only VIP lipids found in their classes and therefore they were reported as single species. The nomenclature of lipid classes/species was reported above (see Table 2)Fig. 3ROC analysis of phospholipid biomarker candidates. The performance of five lipid classes belonging to the phospholipid category (A–E), showing significant alterations in CSF (i.e., with VIP ≥ 1.5), for discriminating MA patients from CTRL subjects was evaluated by the area under the ROC curve (AUC) and by the determination of specificity (percentage of true negatives) and sensitivity (percentage of true positive). The nomenclature of lipid classes was reported above (see Table 2)
A simple linear regression model assayed the five phospholipid classes showing VIP ≥ 1.5 and exhibiting good performance after ROC analyses, to establish the reciprocal relationships among them (Fig. 4). Specifically, the expression levels of PC/LPC (Fig. 4A) and LPC/ether PC (Fig. 4B) increased proportionally in CSF of both MA patients and CTRL subjects. On the contrary, the relationships between PC/ether PC (Fig. 4C) and PE/ether PE (Fig. 4D) are directly proportional in CSF of MA patients but not in CTRL subjects. Other tested lipid classes showing linear correlation are shown in Additional File 5.Fig. 4. Simple linear regression model. Statistically significant simple linear regression analyses of selected lipid classes that showed VIP ≥ 1.5 in CSF of MA patients as compared to CTRL subjects; A PC/LPC; B LPC/ether PC; C PC/ether PC; D PE/ether PE; E PC/MAG. The nomenclature of lipid classes was reported above (see Table 2)
As we reported above, MAG was the only lipid class displaying a markedly significant (p < 0.001) decrease in CSF of MA patients as compared to CTRL subjects (Fig. 2C). Interestingly, PC/MAG (Fig. 4E) were correlated by an inverse proportionality only in MA patients’ CSF. Overall, we can hypothesize that the peculiar and significant correlation between PC increase and MAG decrease in patient’s CSF (Fig. 4E) could be suggestive of a MA-associated inflammatory environment.
Discovery of lipids simultaneously altered in plasma and CSF of MA
By comparing current and previous data on plasma lipidomic profile of the same population of MA patients, we found that in CTRL subjects the overall CSF lipid content was 3% of the overall plasma lipid content [33]. Interestingly, in MA patients the CSF lipid content was 14% of the overall plasma lipid content, possibly due to the reported increase of Cer, LPC, PC and PE in MA CSF. Besides, a cumulative depletion of the plasma lipid asset was previously found in MA patients [33]. Conversely, the current lipidomic analyses depicted an overall lipid enrichment for MA CSF. Plasma and CSF lipid pools could be deeply different, since the first one is more prone to change, whereas the blood-brain barrier (BBB) isolates the central nervous system microenvironment from the peripheral vasculature under homeostasis [71, 72]. The relation between lipid decrease at the systemic and local levels still need to be established. It is therefore crucial to gain further insights into the lipid metabolism in inflammatory BBB disruption and the involved mechanisms. Upon the occurrence of strokes, vessels undergo several adverse stimuli that enhance their permeability and instability. CSF may better reflect the pathological changes observed in vascular intimal hyperplasia of MA patients, due to its proximity with the stenotic arteries and the compensatory network of “moyamoya” vessels. Using a myelin-sensitive MR imaging technique, Hara and colleagues found that myelin damage and axonal damage may exist in MA patients [59]. Accordingly, a BBB impairment was demonstrated in MA patients, mainly due to the typical fragile vascular system, to the Angiopoietin-2-related vascular plasticity and to endothelial dysfunction [32, 73].
We finally searched for simultaneously altered lipids in plasma and CSF. The discriminant analysis returned n = 175 (plasma) and n = 70 (CSF) lipids respectively, and n = 10 lipids -belonging to the class of PC- resulted as commonly modulated species in plasma and CSF (Fig. 5A). The concentration of these lipid species was decreased in plasma and augmented in CSF (Fig. 5B), except for PC 42:7 that displayed an opposite trend. Thus, the previously reported lipid depletion in plasma was now counterbalanced by a CSF lipid enrichment. Such evidence seems to be of great relevance, as it was possible to identify PC as the unique class responsible for this peculiar finding. Our findings are in agreement with those previously reported by an untargeted metabolomic approach that identified a distinct LPC decrease in serum samples from MA patients, when compared to controls [27].Fig. 5. Common lipid features between plasma and CSF of MA. A Intersection size graph showing the number of lipids altered in both plasma [33] and CSF of the same MA population. B Heatmap of lipids (n = 10) altered in both plasma and CSF. The concentrations were auto-scaled and log-transformed for visualization. The color-scale for plasma samples differentiates values as high (yellow) and low (blue), whereas for CSF as high (pink) and low (green). HD, healthy donors; CTRL, controls subjects with unrelated cerebrovascular diseases. Statistical significance is evaluated by comparing ranks with Mann–Whitney U test. P values are schematized as follows: ** < 0.01; *** < 0.001
Limitations
The main critical limitation of our study is the small sample size. Indeed, our pilot study focused only on a limited subset of MA patient’s samples (Caucasian, females, mean age of 47 years, bilateral MA presentation) in whom it was possible to collect CSF, because they underwent neurosurgical revascularization procedures. However, such a selected panel precisely represented the whole MA population in Western countries, which is a relevant aspect considering the rarity of the disease. Accordingly, the control subjects were numerically limited because the large part of patients suffering cerebrovascular diseases do not require neurosurgical intervention allowing CSF sampling.
In addition, we have collected data at only one time-point, after the neurological insult that determined this therapeutic option of utmost importance, thus the lack of longitudinal data prevented us from providing information on how lipid levels change over time. It is therefore rather premature to establish correlations between MA patient’s lipidomic profiles and their clinical/demographical characteristics (e.g., disease severity, as assessed by neuroimaging and Suzuki grading), given the limited case history. However, since the disease affects many of our patients bilaterally, they will undergo a double neurosurgical operation months/years apart, and this will allow us to carry out this type of investigation in the future. Nevertheless, we are gradually completing an exhaustive and up-to-date clinical database, including information on disease follow-up that will be useful, in the next future, to correlate our results with the disease status/progression, with the final goal of building a framework to guide therapeutic and preventive approaches for MA management. Most certainly, the implications of our findings are worth considering to be extended to a more numerous cohort.
Conclusions
There is an urgent need for translational research on circulating biomarkers for MA patients’ stratification, to drive personalized therapies and provide prognostic/progression advice to patients and relatives. Thus, the determination of the link between a specific measurable biomarker and significant clinical endpoints is mandatory. By capturing the intricate and multifaceted landscape of the lipidome and tracking changes in circulating lipid levels, lipidomics can depict distinct molecular phenotypes indicative of the physiological and pathological states of an organism [71, 73–76]. Based on our knowledge, this study represents the first attempt to investigate the lipidome profile of CSF samples from a small subgroup of MA patients. Indeed, this study reveals that MA CSF lipid asset is homogeneous per se, but distinctly different from that of control subjects. Interestingly, the category of phospholipids showed a significant increase in MA CSF. Phospholipids are key players in cellular phenotyping, signaling, and homeostasis, maintaining a balance between structural integrity and dynamic responsiveness [77]. Modified phospholipids can change the properties of membranes, and modulate cellular responses, or participate in signaling pathways regulating inflammation and immune response, recently suggested as second hits to trigger MA onset [4, 7]. Specifically, PC emerged as the unique class implicated in the opposite trend between plasma and CSF of the same MA cohort. Thereby, abnormally high- (in CSF) and low- (in plasma) concentrations of this lipid class may play a critical role in MA onset and progression [78] (Fig. 6). Future efforts would be focused on validating these biomarkers using a larger sample size and a targeted lipidomic approach. We will extend the correlation betweeen a panel of selected circulating biomarkers (proteins and lipids) and disease outcome, with the final goal of building a framework to guide therapeutic and preventive approaches for MA management.Fig. 6MA CSF lipidome profile analysis. The main deregulated lipid classes/species, associated with distinct pathological traits, are showed. Red arrows indicate the detection of increasing levels while the blue one stands for decreasing levels as compared to CSF of control subjects. CSF, cerebrospinal fluid; MA, moyamoya angiopathy (Figure created with BioRender)
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Research Committee on the Pathology and Treatment of Spontaneous Occlusion of the Circle of Willis; Health Labour Sciences Research Grant for Research on Measures for Infractable Diseases. Guidelines for diagnosis and treatment of moyamoya disease (spontaneous occlusion of the circle of Willis). Neurol Med Chir (Tokyo). 2012;52(5):245–66. 10.2176/nmc.52.24510.2176/nmc.52.24522870528 · doi ↗ · pubmed ↗
- 2Bersano A, Bedini G, Nava S, Acerbi F, Sebastiano DR, Binelli S, et al.; GEN-O-MA study group. GEN-O-MA project: an Italian network studying clinical course and pathogenic pathways of moyamoya disease-study protocol and preliminary results. Neurol Sci. 2019;40(3):561–570. 10.1007/s 10072-018-3664-z.10.1007/s 10072-018-3664-z 30604336 · doi ↗ · pubmed ↗
- 3MS-DIAL ver. 4.0. RIKEN Center for Sustainable Resource Science, Suehiro-cho, Tsurumi-ku, Yokohama City, Kanagawa, Japan. http://prime.psc.riken.jp/compms /msdial/main.html. Accessed 29 Dec 2023.
- 4Metabo Lights Database. EMBL-EBI, Wellcome Genome Campus, Hinxton, Cambridgeshire, UK. https://www.ebi.ac.uk/metabolights/editor/study/MTBLS 9744/descriptors. Accessed 15 May 2024
- 5Metabo Analyst ver. 5.0. Mc Gill Data Center and Compute Canada, Montréal, Canada. https://www.metaboanalyst.ca. Accessed 17 Dec 2023