Medical School Faculty Diversity and the Liaison Committee on Medical Education’s Diversity Standards
Mytien Nguyen, Tonya L. Fancher, Sarwat I. Chaudhry, Alan Dardik, Laura Castillo-Page, Gbenga Ogedegbe, Paris Butler, Mayur M. Desai, Shruthi Venkataraman, Olivia Marie Campa, Amy Sage, Dowin Boatright

TL;DR
This study examines how the introduction of diversity standards by a medical education committee affected faculty diversity in US medical schools.
Contribution
The study provides empirical evidence on the impact of diversity standards on faculty diversity in US medical schools.
Findings
The study found changes in faculty diversity following the introduction of the diversity standards.
Results indicate that the standards influenced the demographic composition of medical school faculties.
Abstract
This cross-sectional study evaluates US medical school faculty diversity before and after introduction of the Liaison Committee on Medical Education’s diversity standards.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
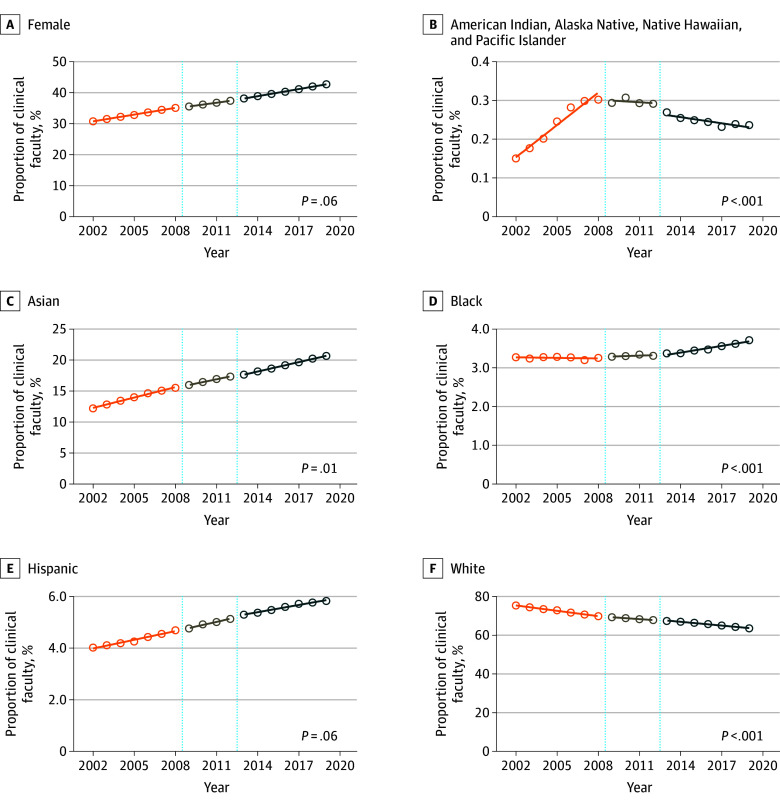 Figure 1
Figure 1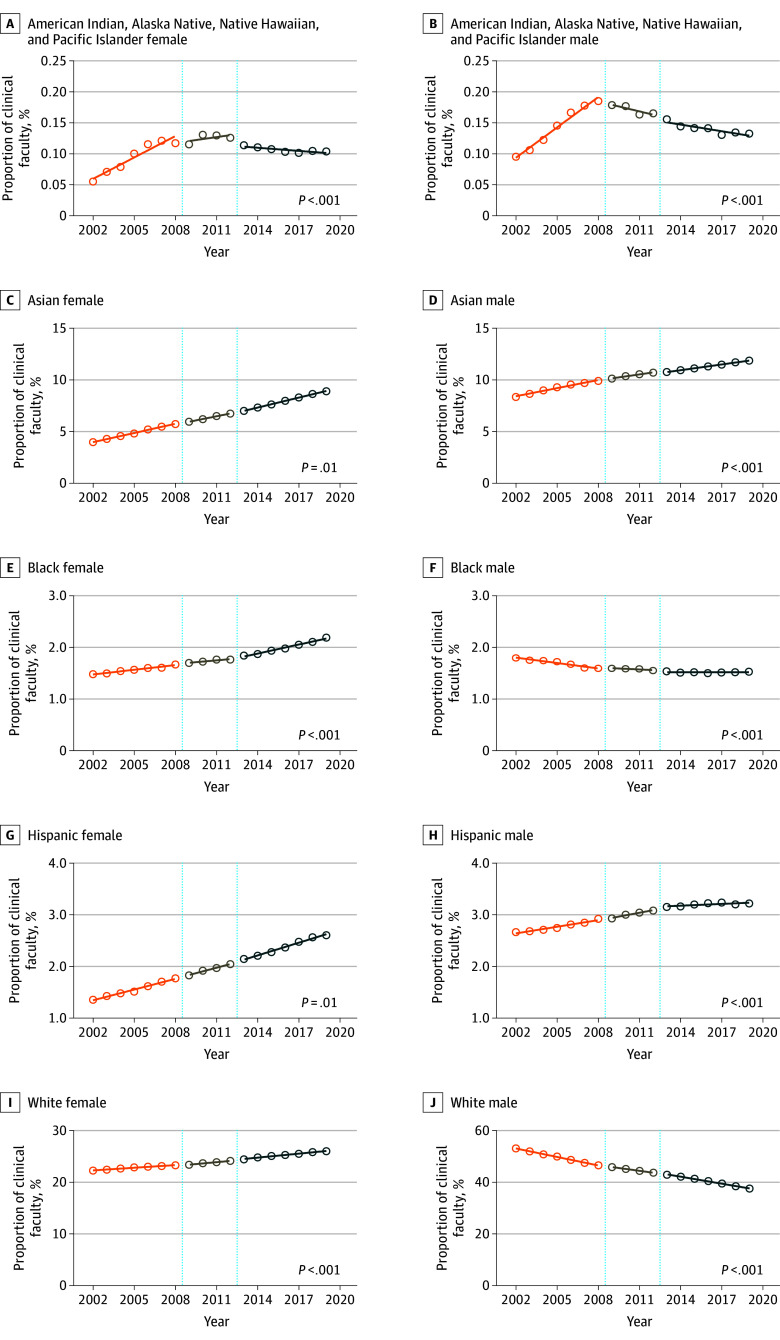 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiversity and Career in Medicine · Medical Education and Admissions · Global Health Workforce Issues
Introduction
Diversity among medical school faculty is critical to provide support, belonging, and mentorship to all students, particularly those from marginalized backgrounds.^1,2^ In 2009, the Liaison Committee on Medical Education (LCME) introduced 2 diversity accreditation standards requiring every medical school to implement “policies and practices to achieve appropriate diversity among its students and faculty.”^3^ Implementation of these standards led to an increase in female, Black, Hispanic, and Asian medical students.^4^ However, beginning in 2025, the revised standards will not require medical schools to implement policies relating to faculty diversity. This study examines faculty diversity after introduction of the 2009 LCME diversity standards.
Methods
We used deidentified data from the Association of American Medical Colleges (AAMC) faculty roster, which includes full-time faculty across schools of medicine and affiliated hospitals from 2002 to 2019. This study follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross sectional studies and met criteria to be exempt from review and need for informed consent by the New York University Grossman School of Medicine’s institutional review board because data were deidentified. Sex, race, and ethnicity were self-reported and defined on the AAMC Faculty Roster website.^5^ Race and ethnicity included American Indian, Alaska Native, Native Hawaiian, and Pacific Islander; Asian; Black; Hispanic; and White.
We defined 3 critical periods for analysis: pre-LCME introduction (2002-2009), implementation (2009-2012), and post-LCME introduction (2012-2019). We calculated annual percentage change (APC) by gender, race, ethnicity, and their intersections, and compared pre-LCME and post-LCME periods using interrupted time series analysis. Statistical significance was defined as a 2-sided P < .05. Statistical analyses were performed using STATA version 18 (StataCorp). Data were analyzed from September to October 2024.
Results
The total number of medical school faculty increased from 112 247 in 2002 to 187 838 in 2019. APC in female faculty did not change after the introduction of the 2009 LCME diversity standards (APC 0.72%; 95% CI, 0.68% to 0.76%; vs 0.76%; 95% CI, 0.73% to 0.79%; P = .06) (Figure 1A).
Faculty Representation by Sex, Race, and Ethnicity From 2002 to 2019Annual faculty representation during 3 critical Liaison Committee on Medical Education (LCME) periods: pre-LCME diversity standards introduction from 2002 to 2009, implementation period from 2009 to 2012, and post-LCME diversity standards introduction from 2012 to 2019. P-values within graphs indicate significance from interrupted time series comparison between pre- and post-LCME diversity standards introduction periods (2002-2009 vs 2012-2019).
Among racial and ethnic groups, the decline in APC for White faculty significantly decreased after implementation (−0.92%; 95% CI, −0.98% to −0.86%; vs −0.64%; 95% CI, −0.72% to −0.57%; P < .001) (Figure 1B). APC for White female faculty increased after implementation (0.25%; 95% CI, 0.22% to 0.28% vs 0.17%; 95% CI, 0.14% to 0.19%; P < .001). The decline in APC for White male faculty decreased after implementation (−1.09%; 95% CI, −1.14% to −1.04% vs −0.90%; 95% CI, −0.96% to −0.85%; *P *< .001) (Figure 2). APC in overall Asian faculty significantly decreased after implementation, while there was an APC decrease for Asian male faculty, and an increase for Asian female faculty (Asian: APC, 0.55%; 95% CI, 0.51 to 0.60% vs 0.50%; 95% CI, 0.49% to 0.52%; P = .01; Asian male: APC, 0.26%; 95% CI, 0.22% to 0.30% vs 0.18%; 95% CI, 0.17% to 0.19%; P < .001; Asian female: APC, 0.29%; 95% CI, 0.28% to 0.31% vs 0.32%; 95% CI, 0.31% to 0.33%; P = .01) (Figure 1C, Figure 2).
Faculty Representation by Intersection of Sex, Race, and Ethnicity From 2002 to 2019Annual faculty representation by sex during 3 critical Liaison Committee on Medical Education (LCME) periods: pre-LCME diversity standards introduction from 2002 to 2009, implementation period from 2009 to 2012, and post-LCME diversity standards introduction from 2012 to 2019. P-values within graphs indicate significance from interrupted time series comparison between pre- and post-LCME diversity standards introduction periods (2002-2009 vs 2012-2019).
LCME standards were associated with an APC increase for Black faculty (0.00%; 95% CI, −0.01% to 0.00%; vs 0.05%; 95% CI, 0.04% to 0.07%; P < .001) (Figure 1D). While APC in Black male faculty was decreasing before 2009, this decline halted after the LCME diversity standards were introduced (−0.03%; 95% CI, −0.04% to −0.02%; vs 0.00%; 95% CI, 0.00% to −0.01%; P < .001). After the standards were introduced, APC in Black female faculty slightly increased (0.03%; 95% CI, 0.02% to 0.04%; vs 0.05%; 95% CI, 0.05% to −0.06%; P < .001) (Figure 2).
While the LCME standards were not associated with APC difference for Hispanic faculty (0.11%; 95% CI, 0.09% to 0.13% vs 0.09%; 95% CI, 0.08% to 0.10%; P = .06)., APC increased for Hispanic female (0.06%; 95% CI, 0.05% to 0.08%; vs 0.08%; 95% CI, 0.07% to 0.09%; P = .03) and decreased for Hispanic male faculty (0.04%; 95% CI, 0.03% to 0.05%; vs 0.01%; 95% CI, 0.00% to 0.02%; P < .001) (Figure 2).
APC in American Indian, Alaska Native, Native Hawaiian, and Pacific Islander faculty significantly decreased after implementation (0.02%; 95% CI, 0.02% to 0.03%; vs −0.01%; 95% CI, −0.01% to 0.00%; P < .001) (Figure 1F). Similar associations were found for both female and male faculty within this group (female: 0.01%; 95% CI, 0.007% to 0.01% vs −0.001%; 95% CI, −0.002% to −0.003%; P < .001; male: 0.01%; 95% CI, 0.01% to 0.01% vs −0.003%; 95% CI, −0.005% to −0.001%; P < .001) (Figure 2).
Discussion
Findings from this study suggest that while the 2009 LCME diversity standards were associated with gains in racial and ethnic diversity for medical students,^4^ the gains for faculty were not uniform. LCME diversity standards’ greater association with student diversity than faculty diversity may be because medical schools have more direct control over admissions policies, and potentially a more intentional focus on student diversity compared with faculty diversity, while faculty diversity may be constrained by slower hiring cycles and a more limited pool of underrepresented candidates. While representation of Black faculty increased with LCME standards introduction, the overall percentage of Black faculty remain small, and there was no gain for Black male faculty. The lack of Black male faculty in medicine limits role models for all students, particularly Black male students, making it difficult to mitigate the persistent lack of growth of Black men entering medicine. There is a persistent decline in Indigenous faculty, which highlights the need to promote Indigenous matriculants, graduates, and faculty.^6^ This study is limited by other potential factors that may influence faculty hiring, such as a rise in cluster hiring practices. However, with LCME removing faculty diversity requirements in 2025, future research is critical to assess its impact on hiring processes and faculty diversity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Boatright D, Nguyen M, Hill K, . Development of a tool to measure student perceptions of equity and inclusion in medical schools. JAMA Netw Open. 2024;7(2):e 240001. doi:10.1001/jamanetworkopen.2024.000138381434 PMC 10882418 · doi ↗ · pubmed ↗
- 2Anderson N, Nguyen M, Marcotte K, Ramos M, Gruppen LD, Boatright D. The long shadow: a historical perspective on racism in medical education. Acad Med. 2023;98(8S):S 28-S 36. doi:10.1097/ACM.000000000000525337071703 PMC 10584990 · doi ↗ · pubmed ↗
- 3Liaison Committee on Medical Education. Liaison Committee on Medical Education (LCME) standards on diversity. 2009. Accessed August 19, 2024. https://health.usf.edu/~/media/Files/Medicine/MD%20Program/Diversity/LCME Standardson Diversity 1.ashx?la=en
- 4Boatright DH, Samuels EA, Cramer L, . Association between the Liaison Committee on Medical Education’s Diversity Standards and changes in percentage of medical student sex, race, and ethnicity. JAMA. 2018;320(21):2267-2269. doi:10.1001/jama.2018.1370530512090 PMC 6583477 · doi ↗ · pubmed ↗
- 5Association of American Medical Colleges. Faculty roster: U.S. medical school faculty. Accessed December 15, 2024. https://www.aamc.org/data-reports/faculty-institutions/report/faculty-roster-us-medical-school-faculty
- 6Brodt E, Bruegl A, Miller MF, . The indigenous faculty forum: a longitudinal professional development program to promote the advancement of indigenous faculty in academic medicine. Hawaii J Health Soc Welf. 2019;78(12)(suppl 3):8-13.31930195 PMC 6949475 · pubmed ↗