Left ventricular outflow tract obstruction in transthyretin amyloid cardiomyopathy: a case report on diagnostic and treatment challenges and role of alcohol septal ablation
Ali Hussein Jaber Mejren, Sie Kronborg Fensman, Steen Hvitfeldt Poulsen

TL;DR
A case report highlights the diagnostic and treatment challenges of a heart condition involving left ventricular outflow tract obstruction and the use of alcohol septal ablation.
Contribution
Demonstrates the successful use of alcohol septal ablation in managing left ventricular outflow tract obstruction in transthyretin amyloid cardiomyopathy.
Findings
Alcohol septal ablation resolved left ventricular outflow tract obstruction in a patient with transthyretin amyloid cardiomyopathy.
Balancing diuretics and beta-blockers is crucial for managing symptoms in this condition.
Accurate diagnosis is essential to avoid mismanagement of transthyretin amyloid cardiomyopathy.
Abstract
Transthyretin amyloid cardiomyopathy (ATTR-CM) is a restrictive cardiomyopathy caused by amyloid deposition in the myocardium. Its phenotypical overlap with hypertrophic cardiomyopathy, particularly in cases involving left ventricular outflow tract obstruction (LVOTO), challenges accurate diagnosis. Medical management of LVOTO in ATTR-CM is challenged by the opposing effects of beta-blockers and diuretics. A 79-year-old male with left ventricular hypertrophy and LVOTO presented with worsening dyspnoea. Full diagnostic work-up confirmed wild-type ATTR-CM. A conservative medical approach with diuretics and beta-blockers proved challenging. Alcohol septal ablation was successfully performed without major complication, resolving the LVOTO and improving symptoms. The diagnosis and management of ATTR-CM with LVOTO are complex. A thorough diagnostic approach is needed to avoid mismanagement.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
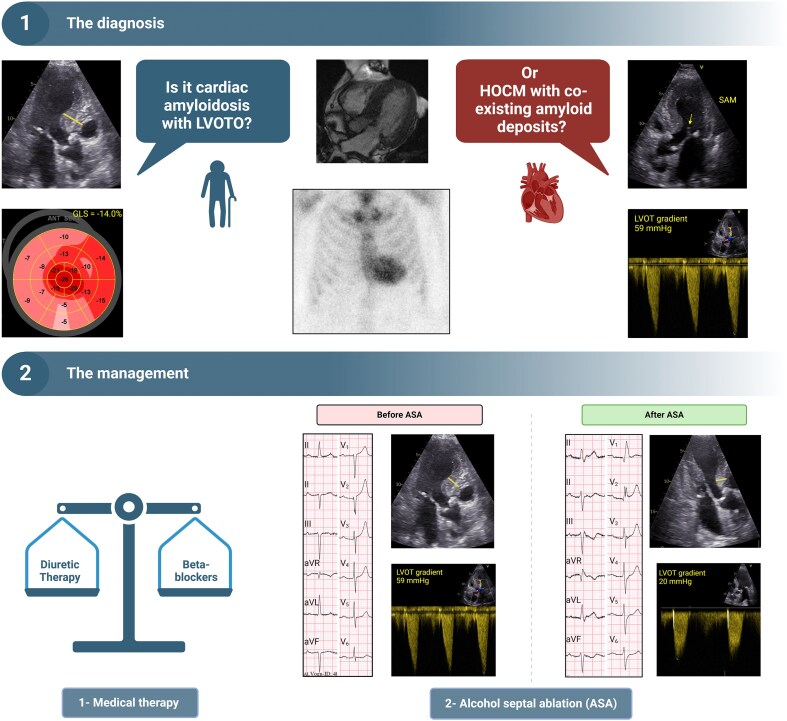 Figure 1
Figure 1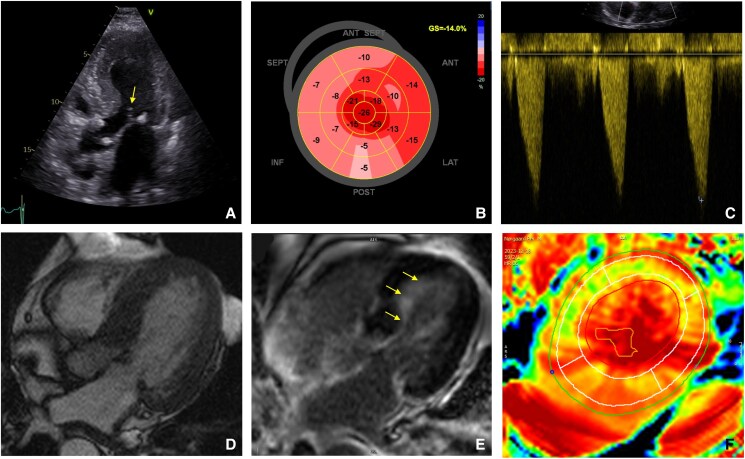 Figure 1
Figure 1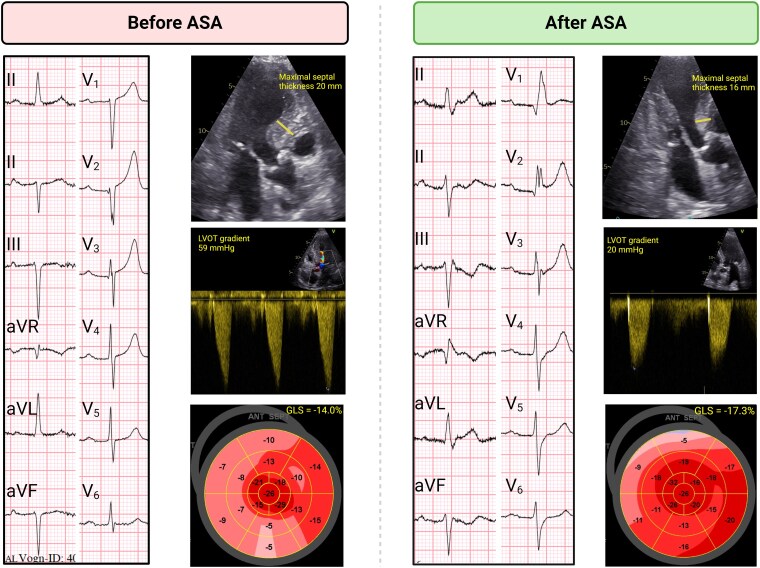 Figure 2
Figure 2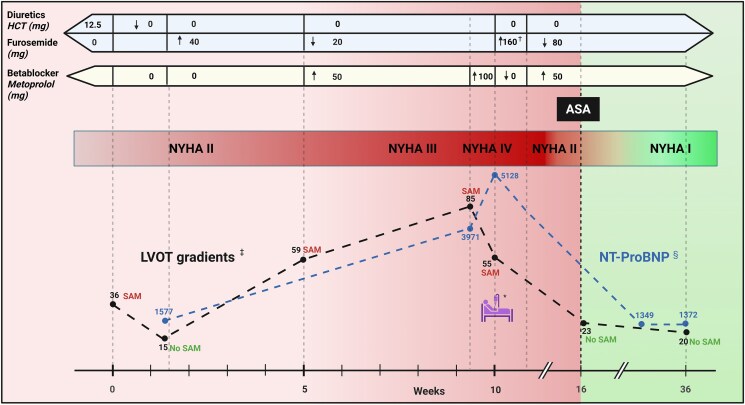 Figure 3
Figure 3| Parameter | Result | Normal range |
|---|---|---|
| EDV (mL) | 84.4 | 95–215 |
| EDV index (mL/m2) | 42.3 | 50–108 |
| ESV (mL) | 20.7 | 25–85 |
| ESV index (mL/m2) | 10.3 | 11–47 |
| LVEF (%) | 75.5 | 49–79 |
| LV mass (g) | 207.3 | 66–176 |
| LV mass index (g/m2) | 103.8 | 39–85 |
| Maximal LV wall thickness (mm) | 24.2 | ≤11 |
| Native T1, total (ms) | 1091 ± 61 | 905–1073 |
| ECV (%) | ||
| - Total | 37 ± 8 | 17–29 |
| - Basal section | 31.7 | |
| - Middle section | 36.0 | |
| - Apical section | 42.6 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParathyroid Disorders and Treatments · Amyloidosis: Diagnosis, Treatment, Outcomes · Cellular transport and secretion
Introduction
Transthyretin amyloid cardiomyopathy (ATTR-CM) is an infiltrative restrictive cardiomyopathy caused by amyloid fibril deposition in the myocardium. This leads to thickened left ventricular (LV) walls, reduced LV cavity size, and systolic and diastolic dysfunction. Transthyretin amyloid cardiomyopathy has been detected in ∼17% of elderly patients with heart failure (HF) and septal hypertrophy.^1^
The echocardiographic phenotype in ATTR-CM often mimics hypertrophic cardiomyopathy (HCM).^2^ Myocardial thickening in ATTR-CM is often most prominent in the basal septum, which can cause dynamic LV outflow tract obstruction (LVOTO) in a small subset of cardiac amyloidosis patients.^3,4^ This phenotypical overlap can challenge the differentiation between ATTR-CM with LVOTO and obstructive HCM (HOCM).
Treatment of ATTR-CM and HOCM differs due to the distinct underlying pathophysiological mechanisms. In co-existing ATTR-CM and LVOTO cases, management requires a carefully balanced approach using diuretics and beta-blockers. We present a case of LVOTO in a patient with presumed wild-type ATTR-CM, highlighting diagnostic and therapeutic challenges and evaluating the safety and efficacy of transcatheter alcohol septal ablation (ASA).
Summary figure
**
Case presentation
A 79-year-old male patient with hypertension and well-controlled moderate asthma presented with progressive dyspnoea, consistent with New York Heart Association (NYHA) Class II, and increasing leg oedema over 6 months. Baseline treatment included losartan/hydrochlorothiazide 50 + 12.5 mg/day, beta-2 agonist, and steroid inhalations.
Initial transthoracic echocardiography demonstrated significant LV hypertrophy measured 20 mm in the septum, preserved LV ejection fraction (LVEF) of 60%, systolic anterior motion of the mitral valve (SAM), and mild mitral regurgitation. Doppler flow over the LV outflow tract (LVOT) showed classic dagger-shaped curves with a maximum resting gradient of 36 mmHg, suggesting HOCM. Losartan/hydrochlorothiazide was discontinued, and the patient was referred to our tertiary cardiac centre.
At our centre, transthoracic and transoesophageal echocardiography showed LVOT flow acceleration by colour Doppler, with an LVOT gradient of 15 mmHg at rest and 31 mmHg during Valsalva. No SAM was detected. Global longitudinal strain (GLS) was −16.6% with a relative apical sparing (RELAPS) pattern (Figure 1A–C).
Imaging. (A–C) Echocardiography images: (A) apical five-chamber view displaying systolic anterior motion of the mitral valve (arrow). (B) Bull’s-eye map of the left ventricular global longitudinal strain pattern with relative apical sparing. (C) Continuous wave Doppler showing typical dagger-shaped signal of left ventricular outflow tract gradient. (D–F) Cardiac magnetic resonance images. (D) Cine Cardiac magnetic resonance image showing asymmetrical left ventricular hypertrophy. (E) Inversion recovery sequence showing late gadolinium enhancement with subendocardial late gadolinium enhancement pattern (yellow arrows). (F) Extracellular volume map.
Cardiac magnetic resonance (CMR) revealed severe LV hypertrophy, preserved LVEF, and subendocardial late gadolinium enhancement that did not follow an ischaemic pattern (Figure 1D–F). Detailed CMR measurements are shown in Table 1.
Transthyretin amyloid cardiomyopathy was suspected due to several red flags, including advanced age, male sex, and slightly reduced GLS with RELAPS. Classic low-voltage electrocardiogram (ECG) was absent; however, discordance between normal QRS voltage and severe LV hypertrophy raised suspicion. Other common red flags, such as carpal tunnel syndrome, spinal stenosis, and peripheral neuropathy, were absent. Wild-type ATTR-CM diagnosis was confirmed by high myocardial uptake on ^99m^Tc- 3,3-diphosphono-1,2-propanodicarboxylic acid (DPD) scintigraphy (Perugini Grade 3), normal plasma free-light chain quantification, and absence of plasma and urine monoclonal protein. Endomyocardial biopsies showed Congo-red positive amyloid deposition, confirmed by mass spectrometry as ATTR. There were no signs of myocardial disarray. Genetic testing was negative for mutations associated with hereditary ATTR-CM and HCM. Oral furosemide 40 mg/day was initiated due to leg oedema.
One month later, there was no clinical improvement. Echocardiography showed a peak resting LVOT gradient of 59 mmHg, and SAM reoccurred with mild mitral regurgitation. Global longitudinal strain decreased further to −14%. Furosemide was reduced to 20 mg/day, and metoprolol 50 mg/day was initiated.
While attempting to balance diuretics and beta-blockers, the patient’s symptoms remained poorly controlled and progressively worsened to NYHA Class III. Left ventricular outflow tract gradients increased to 85 mmHg at rest and 105 mmHg during Valsalva. In response, metoprolol was increased to 100 mg/day. Although LVOT gradients decreased, the patient’s condition deteriorated, leading to hospitalization a few days later due to decompensated HF. Intravenous diuretics and pleural drainage resulted in a significant clinical improvement (NYHA Class II) at discharge.
Following discharge, the persistence of LVOTO, combined with the continued need for diuretic therapy, prompted the decision to perform ASA.
Alcohol septal ablation was performed without complications, resolving LVOTO and reducing proximal septal wall thickness. However, the patient developed a post-ASA right bundle branch block in addition to a pre-existing left anterior fascicular block and first-degree atrioventricular (AV) block. No advanced AV block was detected neither during monitoring at hospital admission nor during post-ASA Holter.
At a 5-month post-ASA clinical follow-up, the patient reported significant improvement, with almost no functional symptoms, thus classified as NYHA Class I. Echocardiography showed no signs of increased LVOT gradients or SAM, neither at rest nor during Valsalva, preserved LVEF, and significant improvement in GLS (−17.3) (Figure 2).
Before and after alcohol septal ablation. ASA, alcohol septal ablation; GLS, global longitudinal strain; LVOT, left ventricular outflow tract.
Discussion
This case illustrates the complexities of diagnosing and managing ATTR-CM patients when complicated by co-existing LVOTO.
The first challenge was to establish the correct diagnosis. The initial echocardiography suggested HOCM, but a positive DPD scintigraphy (Perugini Grade 3) contradicted this perception. A key dilemma was whether this was HOCM with co-existing amyloid deposits or cardiac amyloidosis with concurrent LVOTO. Helder et al.^6^ identified amyloid deposits in septal myomectomy specimens of 0.9% of patients undergoing septal myomectomies for HOCM. However, the authors concluded that these mild deposits were insufficient to explain LVOTO, thus reinforcing the primary diagnosis of HOCM. In contrast, our patient had biopsy-confirmed ATTR depositions and Perugini Grade 3 DPD scintigraphy, indicative of a high amyloid burden.^7^ Coupled with reduced GLS and RELAPS, negative genetic testing for HCM, patient's sex, and advanced age, these findings strongly favour a diagnosis of wild-type ATTR-CM.^2,8^
Notably, CMR revealed the highest extracellular volume values in the apex. This may contradict the theory of a base-to-apex amyloid gradient as the cause of RELAPS.^9^ However, De Gaspari et al.^10^ suggested that RELAPS pattern may not reflect a base-to-apex amyloid gradient but rather a more complex epiphenomenon.
The next challenge was developing an appropriate treatment plan. Transthyretin amyloid cardiomyopathy is characterized by elevated filling pressures at rest and especially during exercise, which usually leads to clinical signs of fluid overload requiring diuretic therapy.^11^ In contrast, diuretics are relatively contraindicated in HOCM as they may exacerbate LVOTO due to small LV cavity and hypercontractile myocardium. Beta-blockers are first-line therapy for HOCM due to their ability to decrease contractility and heart rate, allowing for better diastolic filling, and minimizing LVOTO.^12^ However, beta-blockers are generally avoided in ATTR-CM as the condition is associated with low stroke volume, necessitating a higher heart rate to maintain adequate cardiac output.^13^
This opposing effect of treatment strategies was demonstrated in our patient. Left ventricular outflow tract obstruction was highly sensitive to changes in preload. Flow acceleration and SAM were detected whenever the patient was on diuretic therapy and resolved or minimized when diuretics were discontinued. However, reducing diuretics likely worsened hypervolaemia. Although metoprolol reduced LVOT gradients, it may have further contributed to clinical deterioration due to its negative inotropic and chronotropic effects (Figure 3).
*Timeline. Admission to the ward because of decompensation. †Intravenous diuretics. ‡Resting left ventricular outflow tract gradients (mmHg). §Normal range for N-terminal pro-B-type natriuretic peptide <300 ng/L. ASA, alcohol septal ablation; HCT, hydrochlorothiazide; LVOT, left ventricular outflow tract; NT-proBNP, N-terminal pro-B-type natriuretic peptide; NYHA, New York Heart Association; SAM, systolic anterior motion of the mitral valve.
Given these considerations, ASA was deemed the best treatment option. Data on efficacy and safety of ASA in this subset of patients are limited. However, this case demonstrated the long-term efficacy and safety of ASA in managing this complex case as it ensured complete resolution of LVOTO without major complications.
Alcohol septal ablation has been reported in a few cases of LVOTO in cardiac light chain amyloidosis, with satisfactory clinical results and without safety concerns.^14,15^ To our knowledge, this is the first case report describing ASA in ATTR-CM patients. This emphasizes the need for further research to explore and validate treatment strategies for managing LVOTO in ATTR-CM.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ruiz-Hueso R, Salamanca-Bautista P, Quesada-Simón MA, Yun S, Conde-Martel A, Morales-Rull JL, et al Estimating the prevalence of cardiac amyloidosis in old patients with heart failure—barriers and opportunities for improvement: the PREVAMIC study. J Clin Med 2023;12:2273.36983274 10.3390/jcm 12062273 PMC 10057876 · doi ↗ · pubmed ↗
- 2Maurizi N, Rella V, Fumagalli C, Salerno S, Castelletti S, Dagradi F, et al Prevalence of cardiac amyloidosis among adult patients referred to tertiary centres with an initial diagnosis of hypertrophic cardiomyopathy. Int J Cardiol 2020;300:191–195.31371117 10.1016/j.ijcard.2019.07.051 · doi ↗ · pubmed ↗
- 3Longinow J, Chedid El Helou M, Finet JE, Moudgil R, Jaber W, Thamilarsan M, et al Left ventricular outflow tract obstruction in cardiac amyloidosis. J Card Fail 2024;30:233–234.
- 4Mookadam F, Haley J, Olson L, Cikes M, Mookadam M. Dynamic left ventricular outflow tract obstruction in senile cardiac amyloidosis. Eur J Echocardiogr 2006;7:465–468.16236554 10.1016/j.euje.2005.09.002 · doi ↗ · pubmed ↗
- 5Kawel-Boehm N, Hetzel SJ, Ambale-Venkatesh B, Captur G, Francois CJ, Jerosch-Herold M, et al Reference ranges (“normal values”) for cardiovascular magnetic resonance (CMR) in adults and children: 2020 update. J Cardiovasc Magn Reson 2020;22:87.33308262 10.1186/s 12968-020-00683-3PMC 7734766 · doi ↗ · pubmed ↗
- 6Helder MRK, Schaff HV, Nishimura RA, Gersh BJ, Dearani JA, Ommen SR, et al Impact of incidental amyloidosis on the prognosis of patients with hypertrophic cardiomyopathy undergoing septal myectomy for left ventricular outflow tract obstruction. Am J Cardiol 2014;114:1396–1399.25217455 10.1016/j.amjcard.2014.07.058 · doi ↗ · pubmed ↗
- 7Ungericht M, Groaz V, Messner M, Schuetz T, Brunelli L, Zaruba MM, et al Correlation of 99m Tc-DPD bone scintigraphy with histological amyloid load in patients with ATTR cardiac amyloidosis. Amyloid 2024;31:22–31.37530216 10.1080/13506129.2023.2239986 · doi ↗ · pubmed ↗
- 8Arbelo E, Protonotarios A, Gimeno JR, Arbustini E, Barriales-Villa R, Basso C, et al 2023 ESC guidelines for the management of cardiomyopathies. Eur Heart J 2023;44:3503–3626.37622657 10.1093/eurheartj/ehad 194 · doi ↗ · pubmed ↗