Coexistence of Tuberculous Lymphadenitis and Hodgkin Lymphoma: A Diagnostic Challenge
Mridima Chandra, Maitri Parmar, Ajeet K Khilnani

TL;DR
A 10-year-old boy had both tuberculosis and Hodgkin lymphoma, showing how similar symptoms can make diagnosis difficult.
Contribution
This case highlights the rare coexistence of tuberculous lymphadenitis and Hodgkin lymphoma.
Findings
The patient was initially diagnosed with tuberculosis but showed no improvement with treatment.
Repeated biopsies confirmed the presence of both tuberculosis and Hodgkin lymphoma in the same lymph node.
The case underscores the need to consider malignancies in persistent lymphadenopathy in TB-endemic regions.
Abstract
Hodgkin lymphoma (HL) and tuberculosis (TB) share overlapping clinical features, such as lymphadenopathy, fever, weight loss, and night sweats, which can complicate the diagnostic process, particularly in endemic regions. This case report describes a 10-year old boy with persistent cervical lymphadenopathy, initially diagnosed as tuberculous lymphadenitis based on fine-needle aspiration cytology (FNAC). The child was promptly started on anti-tubercular therapy (ATT), but his condition showed no improvement. Repeated biopsies ultimately revealed mixed cellularity HL, with the same lymph node testing positive for Mycobacterium tuberculosis, confirming a rare coexistence of both diseases. This case highlights the challenges clinicians face when both TB and HL are present, as the clinical symptoms may overlap. It also emphasizes the importance of considering malignancies as differential…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
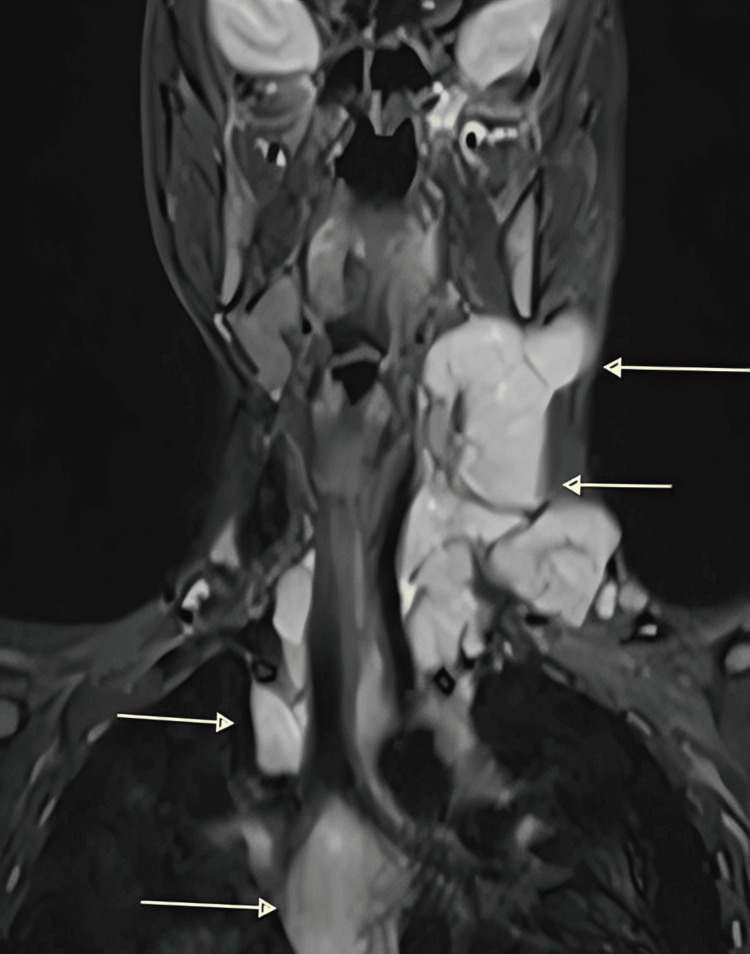 Figure 1
Figure 1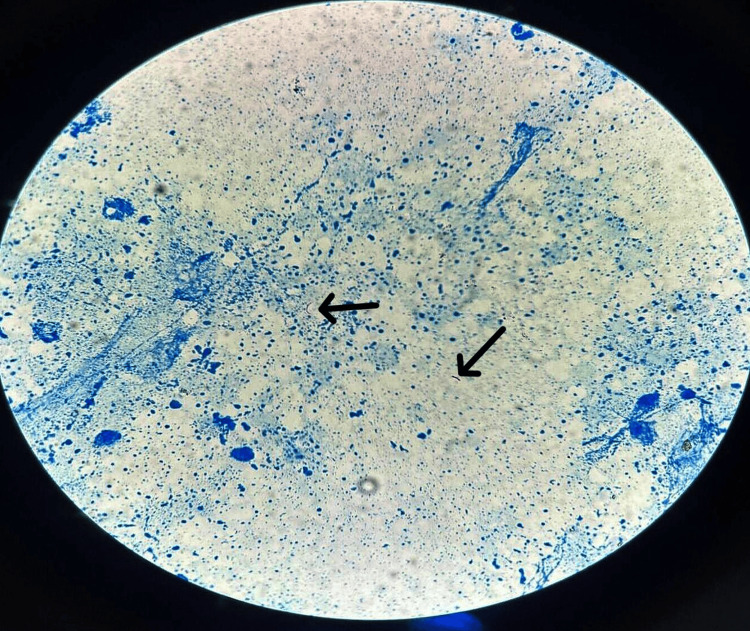 Figure 2
Figure 2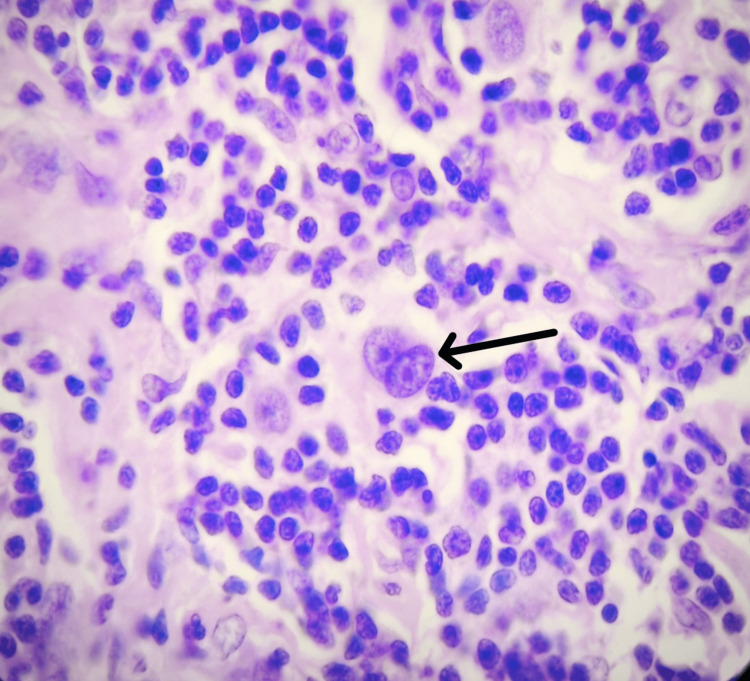 Figure 3
Figure 3| Date | Investigation | Report | Action taken | Time duration since initial presentation |
| June 29, 2022 | CECT Neck | Suspicious for lymphoma | 0 | |
| June 29, 2022 | 1st FNAC | Granulomatous lymphadenitis | ATT Started | 0 |
| June 29, 2022 | Culture and sensitivity of sputum | No organism reported | - | 3 days |
| August 11, 2022 | 1st CBNAAT |
| ATT continued | 1.5 months |
| October 17, 2022 | 2nd FNAC | Reactive lymphadenitis | ATT Continued | 3.5 months |
| June 15, 2023 | 1st excision biopsy | Tuberculous lymphadenitis with hyalinized lymphoid parenchyma (due to ATT therapy) | ATT Continued | I year |
| January 29, 2024 | 3rd FNAC | Lymphadenitis, granulomatous lesion cannot be ruled out | 18 months | |
| January 29, 2024 | 2nd CBNAAT |
| ATT stopped | |
| February 1, 2024 | CECT Neck and MRI Neck | Koch's lymphadenitis or neoplastic etiology | ||
| February 3, 2024 | 2nd excision biopsy | Classic Hodgkin lymphoma, mixed cellularity subtype | Chemotherapy advised awaiting IHC report | |
| February 20, 2024 | IHC | Positive for CD 30 and PAX-5 (Classic Hodgkin lymphoma, nodular sclerosis subtype) | Chemotherapy started | |
| December 20, 2024 | Follow-up | Patient took six cycles of Adriamycin, Bleomycin, Vinblastine and Dacarbazine and was symptom free | Chemotherapy stopped |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Infectious Diseases and Tuberculosis · Diagnosis and treatment of tuberculosis
Introduction
Hodgkin lymphoma (HL) and tuberculosis (TB) are significant health challenges in TB-endemic regions where their clinical and histopathological features overlap, often leading to diagnostic dilemmas [1]. HL is a B-cell malignancy characterized by Reed-Sternberg (RS) cells in an inflammatory background, while TB presents with granulomas, necrosis, and Langhans giant cells. Both conditions share symptoms such as fever, weight loss, night sweats, and lymphadenopathy [2]. In TB-endemic areas, clinicians often lean toward TB as the initial diagnosis, particularly when granulomatous inflammation is seen on fine-needle aspiration cytology (FNAC). Diagnostic pitfalls are further exacerbated in resource-limited settings where access to molecular tools and immunohistochemistry (IHC) is restricted. However, this overlap can obscure RS cells, delaying HL diagnosis and treatment. Conversely, HL itself can induce granulomatous reactions that mimic TB histologically [3,4]. Immunohistochemistry, particularly with CD 15 and CD 30 markers, is crucial in distinguishing HL from TB, as these specifically highlight RS cells. Similarly, advanced imaging, including contrast-enhanced computed tomography (CECT) or positron emission tomography-computed tomography (PET-CT), can help delineate the disease and guide targeted biopsies [5].
The literature highlights multiple cases of HL coexisting with TB, with the diagnosis of HL only made after anti-tubercular therapy (ATT) failure or post-mortem. These cases underscore the importance of a multidisciplinary approach involving clinicians, pathologists, and radiologists. Our case highlights the need to consider HL as diagnosis in unresolved lymphadenopathy, especially when patients fail to respond to ATT. Repeat biopsies, IHC, and advanced imaging must be prioritized in such cases. Early and accurate diagnosis of HL is critical to initiating timely treatment, preventing disease progression, and improving patient outcomes.
Case presentation
A 10-year-old boy presented to the Ear, Nose and Throat Outpatient Department of the Gujarat Adani Institute of Medical Sciences, Bhuj, Gujarat, India, with a complaint of left-sided neck swelling for two months. The patient was relatively asymptomatic two months ago and then he developed left neck swelling, which was insidious in onset, gradually progressive in nature, associated with occasional pain, fever, decreased appetite, weight loss and generalized weakness. It was not associated with cough, difficulty in swallowing, pain while swallowing, difficulty in breathing or change of voice. There were no skin lesions, abdominal pain or discomfort. He had no other co-morbidities and no other addiction history.
On inspection, multiple globular swellings were present in left neck, largest measuring approximately 5 cm x 2 cm. The margins were regular with a smooth surface, the skin over it being non-erythematous and non-edematous. The swelling did not move on deglutition or protrusion of tongue. There was no discharge, abnormal pulsations or venous prominence over the swelling. Inspection findings were confirmed on palpation. On palpation, multiple globular matted swellings were present, the largest measuring 5 cm x 2 cm x 2 cm, present over left side of neck at levels II and III. It was non-tender with normal temperature and margins merging into surrounding structures, firm in consistency, non-fluctuant, non-reducible, non-trans-illuminant, non-compressible, not fixed to underlying soft tissues and no pulsations felt over it. On percussion, a dull note was heard and on auscultation, no bruit was heard.
CECT of the neck was performed using submillimeter thin contiguous plain and contrast axial scan of neck with thorax, which was suggestive of multiple enlarged, homogeneously enhancing lymph nodes on left side at level II, III, IV and V stations as well as left occipital stations with mild displacement of the left internal jugular vein. Few homogenously enhancing lymph nodes were also seen on the right side. These findings raised suspicion for lymphoma (Figure 1).
Contrast-enhanced computed tomography (CECT) of the neck showing multiple enlarged, homogeneously enhancing lymph nodes (arrow marked)
FNAC, performed in June 2022, showed granulomatous lymphadenitis with well-formed epithelioid granulomas. Ziehl-Neelsen (ZN) staining was negative for acid-fast bacilli (AFB), and ATT was initiated based on clinical suspicion and cytology, as the patient’s relatives did not consent for excision biopsy at that time. A repeat FNAC (October 2022) indicated reactive lymphadenitis with a reduced node size. Excision biopsy in June 2023 showed hyalinization and fragmented tubercle bacilli, consistent with tuberculous lymphadenitis (Figure 2).
Acid-fast bacilli (AFB) (black arrow) seen in the background of necrosis (ZN stain, 1000x)ZN: Ziehl-Neelsen
The patient continued taking ATT. A third FNAC in January 2024 showed persistent lymphadenopathy with necrosis and Langhans giant cells, though ZN staining remained negative, and malignancy could not be excluded. A second biopsy in February 2024 revealed thickened nodal capsules, effaced architecture, and RS cells, confirming the diagnosis of classic HL, mixed cellularity subtype (Figure 3).
Classical RS cell (black arrow) (H&E, 400x)
Table 1 summarizes the sequence of events leading to the diagnosis of HL.
Discussion
The coexistence or diagnostic overlap between HL and TB presents a significant challenge due to their similar clinical presentations and overlapping histopathological features. Both diseases commonly present with symptoms such as fever, weight loss, and lymphadenopathy, which can easily lead to diagnostic confusion, particularly in areas where TB is endemic [3]. Additionally, granulomatous inflammation is a hallmark of TB and can sometimes be observed in HL as well, further complicating the differentiation between these two conditions. In the case discussed, the initial FNAC revealed granulomatous lymphadenitis, a finding typically suggestive of TB. This led to the initiation of ATT. However, the patient's failure to improve clinically and the persistence of lymphadenopathy raised suspicion of an alternative diagnosis, such as HL [4]. TB can mimic HL, and in such cases, misdiagnosis is not uncommon. Granulomatous inflammation and caseation necrosis, commonly seen in TB, may obscure the presence of RS cells, which are the hallmark of HL. In some instances, HL itself can induce a granulomatous reaction in response to RS cells, creating a histological appearance that resembles TB [6].
Several reports highlight the diagnostic challenges in such cases. For example, Banerjee et al. reported a similar case where HL was initially misdiagnosed as TB due to granulomatous inflammation. It was only after multiple biopsies and the patient's deterioration despite ATT that the correct diagnosis of HL was established [1]. Kunnumbrath et al. described a post-mortem diagnosis of HL in a patient who had been treated for TB, emphasizing the importance of accurate diagnosis, as delayed or missed diagnoses can have severe consequences [6]. Agarwal et al. demonstrated how IHC can be pivotal in distinguishing between HL and TB, especially in ambiguous cases. Markers such as CD 15 and CD 30 specifically identify RS cells, making them critical for confirming HL and distinguishing it from TB, where such markers are absent [7].
In resource-limited settings, where advanced diagnostic tools like IHC and molecular assays are not readily available, the challenge of differentiating HL from TB becomes even more pronounced. In such environments, repeated biopsies, advanced imaging techniques like CECT scans or PET-CT, and clinical expertise are crucial. Multidisciplinary collaboration involving clinicians, radiologists, pathologists, and oncologists is essential for making an accurate diagnosis. Clinicians should maintain a high level of suspicion for malignancies like HL in patients with persistent or unexplained lymphadenopathy, particularly if there is no clinical response to standard TB therapy. The use of advanced diagnostic techniques, even when resources are limited, can significantly improve diagnostic accuracy and patient outcomes.
The consequences of misdiagnosing HL as TB can be dire. HL is a malignancy that typically requires chemotherapy and/or radiation therapy for effective treatment. If treated as TB without considering the possibility of HL, the disease can progress unchecked, leading to worsening clinical conditions and potentially fatal outcomes. On the other hand, timely diagnosis and appropriate treatment of HL often result in favorable outcomes, especially in early-stage disease, where cure rates are high. This case highlights the importance of maintaining a high index of suspicion for HL in patients with persistent lymphadenopathy and underscores the need for early and accurate diagnosis through a combination of clinical judgment, advanced imaging, repeated biopsies, and, where possible, IHC studies [8,9].
Conclusions
This case underscores the critical diagnostic challenge of distinguishing HL from TB in TB-endemic regions, where overlapping clinical and histopathological features often lead to treatment delays. The persistence of lymphadenopathy despite appropriate ATT should prompt clinicians to reconsider the diagnosis and pursue further investigations. As demonstrated in our patient, repeated biopsies, advanced imaging, and IHC played a pivotal role in identifying HL after an extended diagnostic journey. Early recognition and differentiation between HL and TB are vital to initiate timely oncological treatment, and ultimately improve prognosis. Clinicians must maintain a high index of suspicion and adopt a multidisciplinary approach in evaluating unresolved or atypical cases of lymphadenopathy, especially in resource-limited settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diagnostic dilemma of Hodgkin's lymphoma versus tuberculosis: a case report and review of the literature J Med Case Rep Banerjee A Bhuller K Sudhir R Bajaj A 3511520213427547910.1186/s 13256-021-02927-x PMC 8287740 · doi ↗ · pubmed ↗
- 2Association of multifocal Hodgkin's lymphoma and tuberculosis infection: a challenging entity Int J Surg Case Rep El Bouhmadi K Oukessou Y Rouadi S Abada R Roubal M Mahtar M 1067119020223495231010.1016/j.ijscr.2021.106711 PMC 8715107 · doi ↗ · pubmed ↗
- 3Hodgkin lymphoma masquerading as tuberculosis in a young chronic smoker Indian J Hematol Blood Transfus Badyal RK Sharma P Prakash G Malhotra P Varma N 4284323020142533263810.1007/s 12288-014-0450-9PMC 4192257 · doi ↗ · pubmed ↗
- 4Correction Leuk Lymphoma 1060642023
- 5Differentiation between tuberculosis and lymphoma in mediastinal lymph nodes: evaluation with contrast-enhanced MDCT Clin Radiol Tang SS Yang ZG Deng W Shao H Chen J Wen LY 8778836720122248394510.1016/j.crad.2012.02.006 · doi ↗ · pubmed ↗
- 6Necrotising granulomas masking Hodgkin lymphoma: report of a rare case Hematol Transfus Cell Ther Kunnumbrath A Chandra H Azad S Balasubramanian P 06045202310.1016/j.htct.2021.08.010PMC 1043329734896017 · doi ↗ · pubmed ↗
- 7Role of immunohistochemistry in the era of genetic testing in MYC-positive aggressive B-cell lymphomas: a study of 209 cases J Clin Pathol Agarwal R Lade S Liew D 2662706920162630707310.1136/jclinpath-2015-203002 · doi ↗ · pubmed ↗
- 8Tuberculosis coexistence in pediatric Hodgkin's lymphoma: a tropical country experience South Asian J Cancer Padma M Kumar N Munireddy J Kumar A Gujjal PC Premalata SC 236239920203413157510.1055/s-0041-1723629 PMC 8197653 · doi ↗ · pubmed ↗