Urethral Hemangioma Treated With Transurethral Coagulation Using Narrow-Band Imaging: A Case Report
Junichi Ikeda, Hisanori Taniguchi, Monta Inoue, Yuki Masuo, Takahiro Nakamoto, Katsunori Uchida, Masaaki Yanishi, Hidefumi Kinoshita

TL;DR
A man with a urethral hemangioma was successfully treated with transurethral coagulation using narrow-band imaging to avoid complications.
Contribution
Demonstrates the use of narrow-band imaging for precise diagnosis and treatment of urethral hemangiomas.
Findings
Narrow-band imaging enabled accurate visualization of the hemangioma near the urethral sphincter.
The patient had no recurrence of hematuria or urinary incontinence after treatment.
Endoscopic observation during induced erection allowed effective diagnosis and treatment.
Abstract
A 49-year-old man consulted his previous doctor, reporting occasional episodes of macroscopic hematuria after an erection. Cystourethroscopy under artificial erection revealed findings suggestive of a hemangioma in the membranous urethra. The frequency of hematuria decreased with the use of 5α-reductase inhibitors (5ARIs) and hemostatic agents but subsequently increased, leading to the patient’s referral to our department for further examination and treatment. Under general anesthesia and in the lithotomy position, an artificial erection was induced by injecting 80 mg of papaverine hydrochloride into the corpus cavernosum, and a cystourethroscopy was performed using white light. A mass was identified extending from the distal verumontanum of the prostatic urethra to the membranous urethra. Due to the proximity of the hemangioma to the urethral sphincter, narrow-band imaging (NBI) was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
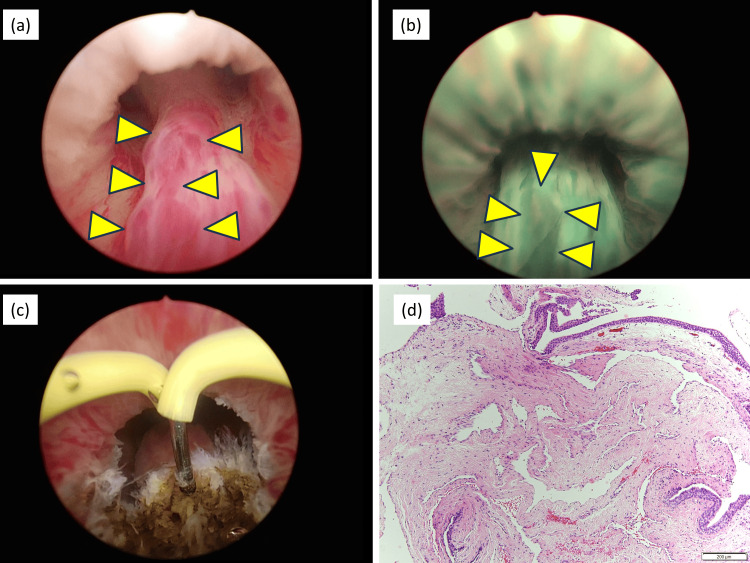 Figure 1
Figure 1| Laboratory test | Result | Normal range |
| Red blood cell count (×10⁶/μL) | 4.87 | 4.0–5.7 |
| Hemoglobin (g/dL) | 13.1 | 12.9–17.2 |
| Hematocrit (%) | 40.7 | 38.2–50.8 |
| White blood cell count (/μL) | 5,200 | 3,500–8,500 |
| Platelet count (×10³/μL) | 276 | 140–340 |
| Creatinine (mg/dL) | 0.76 | 0.6–1.0 |
| C-reactive protein (mg/dL) | 0.01 | <0.3 |
| HbA1c (NGSP) (%) | 5.5 | 4.6–6.2 |
| Activated partial thromboplastin time (sec) | 26.7 | 24–34 |
| Prothrombin time-international normalized ratio | 0.95 | Unknown |
| Prostate-specific antigen (ng/mL) | 0.5 | <4.0 |
| Case | Authors | Published year | Age | Symptom | Causes, triggers of symptom onset | Size/location of hemangioma | Treatment |
| 1 | Cattolica [ | 1982 | 31 | Hematospermia, hematuria | Unknown | Unknown | Fulguration |
| 2 | Cattolica [ | 1982 | 32 | Hematospermia, hematuria | Unknown | Unknown | Fulguration |
| 3 | Cattolica [ | 1982 | NA | Hematospermia, hematuria | Unknown | Unknown | Fulguration |
| 4 | Redman and Young [ | 1987 | 29 | Hematospermia, hematuria | Unknown | Unknown | Fulguration |
| 5 | Borrego Hernando and Maganto Pavón[ | 1996 | 45 | Urethrorrhagia | Following normal erection | Unknown | Argon laser |
| 6 | Lauvetz et al. [ | 1996 | 7 | Hematuria | Unknown | -/anterior urethra | KTP/532 laser |
| 7 | Hayashi et al. [ | 1997 | 30 | Hematospermia, hematuria | Unknown | 5 mm/between the verumontanum and external sphincter | Resection |
| 8 | Furuya et al. [ | 1997 | 53 | Hematospermia, hematuria | Postejaculation | 5 × 4 × 3 mm/distal to the vermontanum | Resection |
| 9 | Khaitan and Hemal [ | 2000 | 14 | Hematuria | Unknown | 1-5 mm/penile urethra | Nd-YAG laser |
| 10 | Parshad et al. [ | 2001 | 23 | Hematuria | Unknown | 10 × 10 mm/Bullbar urethra | Vertical penoscrotal wide excision |
| 11 | Wilson et al. [ | 2001 | 36 | Urethral bleeding | Blue rubber bleb nevus syndrome | -/anterior urethra | Conservative |
| 12 | Demircan et al. [ | 2006 | 18 | Hematuria | Unknown | 22 × 9 mm/bladder neck | Excision by cystostomy |
| 13 | Terada et al. [ | 2007 | 24 | Urethral bleeding | Klippel-Trenaunay-Weber syndrome | -/anterior urethra | Endoscopic sclerotherapy by injecting 5% solution of monoethanolamine oleate (Oldamine) |
| 14 | de León et al. [ | 2008 | 31 | Hematuria, clot expulsion, urinary retention | Unknown | -/prostatic urethra | Ho-YAG laser |
| 15 | Saito [ | 2008 | 50 | Hematospermia, hematuria | Unknown | Unknown | Resection |
| 16 | Saito [ | 2008 | 70 | Hematospermia, hematuria | Unknown | Unknown | Resection |
| 17 | Saito [ | 2008 | 38 | Hematospermia, hematuria | Unknown | Unknown | Resection |
| 18 | Saito [ | 2008 | 41 | Hematospermia, hematuria | Unknown | Unknown | Resection |
| 19 | Saito [ | 2008 | 67 | Hematospermia, hematuria | Unknown | Unknown | Resection |
| 20 | Saito [ | 2008 | 51 | Hematospermia, hematuria | Unknown | Unknown | Resection |
| 21 | Saito [ | 2008 | 80 | Hematuria | Unknown | Unknown | None |
| 22 | Saito [ | 2008 | 68 | Hematuria | Unknown | Unknown | Resection |
| 23 | Saito [ | 2008 | 75 | Hematuria | Unknown | Unknown | Resection |
| 24 | Saito [ | 2008 | 55 | Hematuria | Unknown | Unknown | Resection |
| 25 | Saito [ | 2008 | 63 | Hematuria | Unknown | Unknown | Resection |
| 26 | Saito [ | 2008 | 67 | None | Unknown | Unknown | Resection |
| 27 | Saito [ | 2008 | 56 | None | Unknown | Unknown | Resection |
| 28 | Saito [ | 2008 | 67 | None | Unknown | Unknown | Resection |
| 29 | Saito [ | 2008 | 58 | None | Unknown | Unknown | Resection |
| 30 | Saito [ | 2008 | 56 | None | Unknown | Unknown | Resection |
| 31 | Saito [ | 2008 | 67 | None | Unknown | Unknown | Resection |
| 32 | Saito [ | 2008 | 69 | None | Unknown | Unknown | Resection |
| 33 | Saito [ | 2008 | 77 | None | Unknown | Unknown | Resection |
| 34 | Saito [ | 2008 | 82 | None | Unknown | Unknown | Resection |
| 35 | Efthimiou et al. [ | 2009 | 27 | Urethral bleeding | Unknown | 5 mm/anterior urethra | Excision by biopsy forceps |
| 36 | Noviello et al. [ | 2011 | 1 | Hematuria | Unknown | - | Transurethral excision |
| 37 | Tepeler et al. [ | 2011 | 8 | Urethral bleeding | Klippel-Trenaunay syndrome | -/anterior urethra | Conservative |
| 38 | Abbinante et al. [ | 2012 | 18 | Urethral bleeding | Unknown | -/6 cm far from the external urethral meatus | Surgical removing |
| 39 | Singh and Mandal [ | 2013 | 14 | Urethral bleeding | Unknown | 5 mm/pendular urethra | Transurethral ablation using Ho-YAG laser |
| 40 | Han et al. [ | 2015 | 54 | Hematuria | After ejaculation | -/prostatic urethra | Transurethral resection |
| 41 | Han et al. [ | 2015 | 39 | Hematuria | After ejaculation | -/prostatic urethra | Transurethral resection |
| 42 | Han et al. [ | 2015 | 55 | Hematuria | After ejaculation | -/prostatic urethra | Transurethral resection |
| 43 | Han et al. [ | 2015 | 44 | Hematuria | After ejaculation | -/prostatic urethra | Transurethral coagulation |
| 44 | Han et al. [ | 2015 | 39 | Hematuria | After ejaculation | -/prostatic urethra | Transurethral resection |
| 45 | Hamada et al. [ | 2017 | 73 | Hematuria, dysuria | After ejaculation | -/prostatic urethra | Transurethral resection |
| 46 | Soleimani et al. [ | 2017 | 41 | Hematuria, urethral bleeding | Unknown | 5 mm/anterior urethra | Monopolar electrocautery, Coagulated with Ho-YAG laser |
| 47 | Soleimani et al. [ | 2017 | 22 | Hematuria | Postejaculatory hematuria | 10 mm/12 o’clock of anterior urethra | Coagulated with Ho-YAG laser |
| 48 | Soleimani et al. [ | 2017 | 14 | Urethral bleeding | Unknown | 10 mm, 15 mm/4 o’clock of anterior urethra | Coagulation by Ho-YAG laser |
| 49 | Itesako et al. [ | 2018 | 3 | Urethral bleeding | Unknown | -/bulbar urethra | Oral propranolol |
| 50 | Varea-Malo et al. [ | 2019 | 61 | Urethral bleeding | Unknown | 70 mm/anterior urethra and prostatic urethra with bulbar stricture | Conservative |
| 51 | Yong et al. [ | 2019 | 15 | Hematuria | Unknown | -/membranous urethra | Injection of pingyangmycin |
| 52 | Yong et al. [ | 2019 | 49 | Hematuria, urethral bleeding | After penile erection | 1.1 × 2.4 cm/distance of 2.4 cm from urethral meatus | Injection of pingyangmycin |
| 53 | Masood et al. [ | 2021 | 18 | Urethral bleeding | Unknown | -/5 o’clock of posterior urethra | Fulguration by diathermy and intralesional triamcinolone |
| 54 | Carolan et al. [ | 2022 | 6 | Hematuria | Unknown | 8 × 8 × 6 mm/prostatic urethra | Transurethral resection |
| 55 | Genov et al. [ | 2022 | 64 | Urethral bleeding | Unknown | 7 mm/navicular fossa | Coagulation by Thulium YAG laser |
| 56 | Qian et al. [ | 2022 | 36 | Hematuria | Postejaculatory hematuria | -/5 o’clock of posterior urethra | Excision by plasma electrodes |
| 57 | Ishikawa et al. [ | 2023 | 45 | Painless hematuria, blood clots, urinary retention | After erection/ejection | 6 × 6 mm/prostatic urethra | Transurethral resection |
| 58 | Pal et al. [ | 2023 | 14 | Hematuria | Unknown | Urethra | Coagulation by Ho-YAG laser |
| 59 | Alfentoukh et al. [ | 2023 | 35 | Urethral bleeding | Unknown | 10 mm/verumontanum | Resection |
| Our case | Ikeda et al. | 2025 | 49 | Hematuria | After erection | -/from the distal verumontanum of the prostatic urethra to the membranous urethra | Transurethral coagulation |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrological Disorders and Treatments · Urologic and reproductive health conditions · Urinary Bladder and Prostate Research
Introduction
Urethral hemangioma is a relatively rare and benign hemangioma originating within the urethra [1]. Major symptoms of urethral hemangioma include hematuria, urethral bleeding, and urinary retention; however, they may also be asymptomatic [2]. Although cystourethroscopy is considered useful for diagnosis [3], some cases are only observable during penile erection. Therefore, if diagnosis cannot be established through conventional cystourethroscopy, inducing an artificial erection is required [4]. In this report, we describe a case in which transurethral coagulation of a hemangioma near the urethral sphincter was performed safely using narrow-band imaging (NBI) during induced erection.
Case presentation
A 49-year-old married male patient with children occasionally presented with macroscopic hematuria occurring after erection. His past medical history included hypertension, and he was prescribed dutasteride and olopatadine. Five years prior, he had visited a physician with the same complaint. Cystourethroscopy under artificial erection revealed a suspected hemangioma near the membranous urethra. Due to concerns about the risk of urinary incontinence following transurethral surgery, a conservative management approach using a 5α-reductase inhibitor (5ARI) and hemostatic agents was chosen. Despite an initial decrease in the frequency of hematuria, complete resolution was not achieved, and the symptoms gradually worsened. Consequently, he visited our department in year X for further evaluation and treatment. Laboratory findings are shown in Table 1.
Urinalysis revealed no proteinuria, glycosuria, or hematuria, with red blood cell (RBC) 0-1/HPF, white blood cell (WBC) 0-1/HPF, no epithelial cells, and no bacteria detected. Urine cytology was negative. Contrast-enhanced CT revealed no apparent mass lesions in the urethra.
With the patient’s consent, we performed transurethral resection or coagulation of the urethral hemangioma under general anesthesia. To ensure accurate identification of the tumor and avoid damage to the sphincter, we used NBI.
In year X, under general anesthesia and in the lithotomy position, an artificial erection was induced by locally injecting 80 mg of papaverine hydrochloride into both corpora cavernosa. Cystourethroscopy under white light revealed a tumor extending from the distal verumontanum of the prostatic urethra to the membranous urethra (Figure 1a).
Cystourethroscopy and pathology images(a) Urethral hemangioma observed after induction of artificial erection. (b) Urethral hemangioma observed under narrow-band imaging. (c) Hemangioma after transurethral electrocoagulation with a needle electrode. (d) Histopathological examination of hematoxylin and eosin stain showing a cavernous hemangioma with dilated vessels within the stromal region.
The surface of the tumor appeared red under white light, while NBI clearly delineated the lesion as a vascular structure (Figure 1b). A biopsy of the tumor was performed, followed by coagulation with a needle electrode (Figure 1c). The patient was discharged on postoperative day 3 without complications.
Histopathological examination confirmed a cavernous hemangioma, characterized by dilated vascular structures within the stromal region (Figure 1d). At the three-month follow-up, the patient exhibited no recurrence of hematuria, urinary incontinence, or hematospermia.
Discussion
Urethral hemangioma is a relatively rare benign vascular tumor that has been reported as a cause of hematuria. Including the present case, a total of 60 cases of urethral hemangioma have been reported in men (Table 2) [1-31].
The median age of the patients was 41 years (range: 1-77 years), and 51 of the 60 cases presented with hematuria or urethral bleeding. Among the 38 cases of hematuria, 12 were associated with hematospermia. Postejaculatory hematuria was reported in 10 cases, whereas four cases (including one case with postejaculatory hematuria) experienced hematuria after erection. Hemangioma locations varied, with the prostatic urethra being the most frequently reported site (14 cases). Regarding hemostatic treatment, transurethral resection was the most commonly performed procedure, reported in 34 cases. Laser therapy was performed in 10 of the 60 cases.
The exact cause of urethral hemangioma remains unclear; congenital and acquired theories have been proposed. The congenital theory suggests that it may result from the fetal remnants of angioblastic cells [8], whereas the acquired theory attributes it to repeated increases in venous pressure [1]. According to a report by Saito [1], increased intraurethral pressure during erection or ejaculation may cause vascular rupture, leading to bleeding. Additionally, cases associated with congenital disorders such as Klippel-Trenaunay [14,17] and blue rubber bleb nevus syndromes [12] have also been reported.
Symptoms of urethral hemangiomas vary depending on their location. Cases with hemangiomas in the distal urethra are more likely to present with urethral bleeding, whereas those with hemangiomas near the proximal urethra tend to develop hematuria or urinary retention [26]. In addition, larger hemangiomas have been reported to cause urinary retention or protrusion of the hemangioma from the external urethral meatus [26].
Cystourethroscopy, typically performed in an outpatient setting under local anesthesia, remains the standard method for identifying hemangiomas; however, some cases have been reported in which the lesion could only be detected during erection. Performing cystourethroscopy after inducing an artificial erection has been suggested to improve the visualization of hemangiomas [4]. Additionally, penile ultrasonography and transrectal power Doppler ultrasonography have been reported as useful modalities for detecting enlarged soft tissue and increased blood flow [1]. NBI is a technique that enhances the visualization of blood vessels by improving image resolution and contrast [32]. In the present case, the hemangioma was identifiable under white light after inducing an artificial erection. However, observation under NBI allowed for a more accurate identification of the lesion.
The management of urethral hemangioma depends on the presence of symptoms. Asymptomatic cases can be observed without intervention, but symptomatic cases require some form of treatment, such as coagulation or resection [3]. In recent years, the use of laser coagulation for treatment has been reported [11]. Although 5ARIs have been reported to reduce perioperative bleeding during transurethral resection of the prostate [33], their efficacies in preventing spontaneous bleeding from urethral hemangiomas have not been reported. In addition, 5ARIs have been associated with an increased risk of depression [34], making long-term use difficult in this case.
In this case, we decided to perform transurethral coagulation using endoscopy. Since the hemangioma was located near the urethral sphincter, we aimed to avoid sphincter damage from a resectoscope electrode. By accurately identifying the lesion with NBI, we performed coagulation using a needle electrode and successfully completed the procedure without postoperative complications. To the best of our knowledge, this is the first report of transurethral coagulation of hemangioma using NBI.
Conclusions
This study demonstrates that NBI allowed accurate visualization of the hemangioma, enabling surgical resection without postoperative complications. This suggests that NBI improves the visibility of urethral hemangiomas. Therefore, NBI may contribute to more accurate and safer treatment of these lesions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Posterior urethral hemangioma: one of the unknown causes of hematuria and/or hematospermia Urology Saito S 16816471200810.1016/j.urology.2007.09.05818242389 · doi ↗ · pubmed ↗
- 2Urethral hemangioma: how to investigate as a cause of hematuria after male sexual activities IJU Case Rep Ishikawa K Sasaki H Shimoyama H 454457620233792830510.1002/iju 5.12646 PMC 10622190 · doi ↗ · pubmed ↗
- 3Hemangioma of penile urethra-treatment with simple transurethral excision: a case report Cases J Efthimiou I Kavouras D Vasilakis P Katsanis S 6199220091982977110.4076/1757-1626-2-6199 PMC 2740086 · doi ↗ · pubmed ↗
- 4Massive hemospermia: a new etiology and simplified treatment J Urol Cattolica EV 1511521281982710905310.1016/s 0022-5347(17)52793-7 · doi ↗ · pubmed ↗
- 5Massive post ejaculation hematuria Urology Redman JF Young JW 3rd 73301987360391510.1016/0090-4295(87)90578-4 · doi ↗ · pubmed ↗
- 6Argon laser treatment of urethral angioma. Report of the first case (Article in Spanish)Arch Esp Urol Borrego Hernando J Maganto Pavón E 859861491996 https://pubmed.ncbi.nlm.nih.gov/9065284/9065284 · pubmed ↗
- 7Treatment of extensive urethral hemangioma with KTP/532 laser Lasers Surg Med Lauvetz RW Malek RS Husmann DA 192181996885047110.1002/(SICI)1096-9101(1996)18:1<92::AID-LSM 12>3.0.CO;2-D · doi ↗ · pubmed ↗
- 8Urethral hemangioma: case report J Urol Hayashi T Igarashi K Sekine H 5395401581997922434310.1016/s 0022-5347(01)64530-0 · doi ↗ · pubmed ↗