Predicting patient-reported outcomes of radiofrequency uvulopalatoplasty with tonsillectomy in adult obstructive sleep apnea
Samuel Tschopp, Danilo Esaltato, Kurt Tschopp, Khalid Azalmad, Marco Caversaccio, Urs Borner

TL;DR
This study shows that radiofrequency uvulopalatoplasty with tonsillectomy reduces daytime sleepiness and snoring in adults with sleep apnea, with baseline symptom severity predicting improvement.
Contribution
The study identifies baseline symptom severity as the key predictor of patient-reported outcome improvements after the procedure.
Findings
ESS scores decreased significantly from 8.4 to 4.1 after surgery.
Snoring VAS scores dropped from 7.9 to 3.3 postoperatively.
Baseline ESS and snoring scores were the strongest predictors of improvement.
Abstract
Uvulopalatopharyngoplasty with tonsillectomy is one of the most commonly performed procedures for sleep-disordered breathing, with most studies focusing on objective sleep measurement outcomes. Daytime sleepiness and snoring are important patient-reported outcome measures (PROMs); however, little is known about patient-specific predictors to individualize treatment and guide patient counseling. Patients undergoing radiofrequency uvulopalatoplasty with tonsillectomy between 2015 and 2021 were retrospectively analyzed. Patients underwent a standardized clinical head and neck examination. Preoperatively and three months after surgery, sleep apnea testing and questionnaires were administered. Daytime sleepiness and snoring were evaluated using the Epworth Sleepiness Scale (ESS) and a visual analog scale (VAS, 0–10) preoperatively and three months postoperatively. Primary endpoints were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
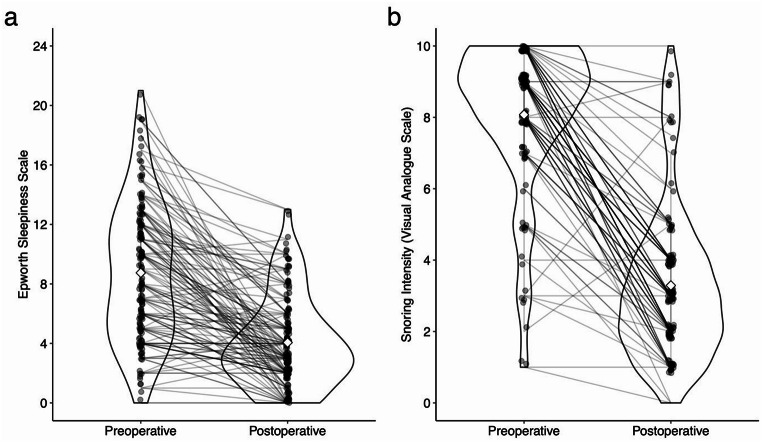 Figure 1
Figure 1- —University of Bern
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObstructive Sleep Apnea Research · Neuroscience of respiration and sleep · Gastroesophageal reflux and treatments
Introduction
Uvulopalatopharyngoplasty with tonsillectomy (UPPP) is the most commonly performed surgical intervention for obstructive sleep apnea and snoring [1, 2]. Traditionally, surgical outcomes have been evaluated primarily using objective measures, notably the apnea-hypopnea index [2]. However, many patients prioritize subjective symptom relief. For individuals with snoring or mild obstructive sleep apnea, improvements in snoring intensity and daytime sleepiness often influence their decision to undergo UPPP. Snoring, in particular, can lead to significant social consequences and negatively affect the sleep quality of bed partners [3, 4]. Additionally, excessive daytime sleepiness markedly impairs daily functioning and impacts quality of life [5–7]. Consequently, evaluating these patient-reported outcomes is essential and of great clinical importance.
Most research predominantly addresses changes in the apnea-hypopnea index. However, objective sleep testing might not adequately capture patient symptoms [6, 8]. Patient-reported outcome measures (PROMs), such as daytime sleepiness [6] and snoring severity [8], have demonstrated weak correlations with objective sleep testing and remain under-investigated following UPPP [9]. A large randomized controlled trial by Browaldh et al. showed significant improvements in daytime sleepiness and quality of life following UPPP with tonsillectomy [5]. Additionally, several studies evaluating various modifications of UPPP have reported similar enhancements in snoring and daytime sleepiness [10–16]. Nonetheless, predictors for individual patient success remain unclear.
To date, little is known about patient-specific predictors, which are crucial to inform personalized patient counseling regarding anticipated improvements in PROMs.
This study aims to identify outcome predictors specifically for daytime sleepiness and snoring, emphasizing PROMs since objective sleep measures have already been extensively studied [12, 13].
Materials and methods
Patient selection
This study included consecutive adult patients undergoing radiofrequency uvulopalatoplasty with tonsillectomy (rfUPP + TE) between 2015 and 2021 for snoring and obstructive sleep apnea at our institution to evaluate PROMs. Exclusion criteria were combined surgical procedures (except nasal surgery), central sleep apnea, neurological comorbidities, non-consent for data use, and missing primary endpoint data.
The study received approval from the local ethics committee (Ethikkommission Nordwestschweiz EKNZ 2021–02324) and was conducted in accordance with the Declaration of Helsinki [17]. Reporting follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [18].
Data collection
All patients underwent a comprehensive preoperative head and neck examination using standardized documentation. The examination included anthropometric measurements, such as weight and height, and detailed assessments of upper airway anatomy, explicitly focusing on Friedman tongue position [19], pharyngeal webbing, uvula size, Brodsky tonsil grading [20], and nasal septum deviation. In cases of asymmetrical tonsil sizes, the higher-grade tonsil was recorded. Patient-reported symptoms were assessed through standardized questionnaires using the Epworth Sleepiness Scale (ESS) for daytime sleepiness [21] and a visual analog scale (0–10) for snoring intensity. Home sleep apnea tests using respiratory polygraphy (Nox T3, Nox Medical, Reykjavik, Iceland) and peripheral arterial tonometry (WatchPAT^®^, Itamar Medical, Caesarea, Israel) were performed preoperatively and repeated three months postoperatively to evaluate surgical outcomes.
Surgical procedure
All patients underwent pharyngeal surgery under general anesthesia. An extracapsular cold-steel tonsillectomy was performed in all patients with tonsillar tissue, irrespective of tonsil size. Elongated uvulae were shortened, preferentially utilizing submucosal resection technique whenever feasible. Hemostasis was achieved through bipolar coagulation. The palatopharyngeal arches were subsequently incised to facilitate mobilization and tension release of the soft palate. Finally, radiofrequency ablation (Erbe VIO 3 electrosurgical unit, Tübingen, Germany) was then performed using a bipolar probe, delivering four to five treatments per side of the palate.
Statistical analysis
Statistical analyses were performed using R version 4.4.3 (R Foundation for Statistical Computing, Vienna, Austria) following guidelines by Steyerberg et al. [22] and the TRIPOD recommendations [23] for model building.
The primary endpoints were the reduction in daytime sleepiness on the ESS and snoring on a VAS, which was measured as the absolute difference between pre- and postoperative values. Secondary endpoints were the responder status to daytime sleepiness and snoring, which were defined analogously to the commonly used Sher criteria for apnea-hypopnea response [24]. For snoring, we considered a patient a responder if postoperative snoring VAS ≤ 3 and reduced by 50% from baseline. ESS responders were defined as a reduction of 50% from baseline and a postoperative ESS < 11.
Univariate analysis was performed with linear regression models for the ESS and snoring reduction for each biologically plausible variable. Univariate logistic regression models assessed predictors for achieving responder status. P values were adjusted for multiple testing using the Benjamini-Hochberg method [25] and considered significant below 0.05. For the multivariate analyses, missing data were handled through multiple imputations, employing predictive mean matching for numerical variables, logistic regression for binary variables, and polytomous regression for categorical variables over 50 iterations [26]. Predictors were selected using backward stepwise regression, which was applied to the stacked imputed datasets and pooled according to Rubin’s rules. The multivariate logistic regression model underwent bootstrapping for internal validation to adjust for optimism and provide corrected performance estimates.
Results
Patient characteristics
Of 306 patients undergoing rfUPP + TE, 142 had a complete data set and were included in the analysis. The median follow-up was 102 days (interquartile range 91–136 days). Table 1 gives an overview of the baseline characteristics. Online Resource Table S1 compares patients included and lost to follow-up, showing no significant differences. Complete data for the snoring follow-up were available in 109 patients, and for ESS in 138 patients. Detailed pre- to postoperative parameters are given in Table 2, showing a significant overall reduction in objective and subjective parameters. A subgroup analysis of patients with (n = 62) and without (n = 80) concomitant nasal surgery was performed (Online Resource Table S2). Besides impaired nasal breathing and septal deviation, pharyngeal webbing was the only significant difference between the patients with and without nasal surgery. No differences in pre- and postoperative sleep testing and PROMs were observed.
Table 1. Baseline characteristics of the study population. Continuous variables are presented as mean ± standard deviation, and categorical variables are given as numbers (percentages)Number of patients142Age (years)47.1 ± 11.8Gender, female13 (9%)Height (cm)177.0 ± 8.2Weight (kg)89.2 ± 14.1Body mass index (kg/m2)28.5 ± 4.2Neck circumference (cm)41.3 ± 3.5Impaired nasal breathing33 (48%)Tonsil grade 00 (0%) 139 (28%) 272 (51%) 327 (19%) 44 (3%)Friedman tongue position 114 (11%) 243 (36%) 345 (35%) 426 (20%)Friedman stage 19 (8%) 260 (56%) 338 (36%) 40 (0%)Pharyngeal webbing normal51 (38%) mild55 (40%) moderate30 (22%)Uvula normal37 (27%) long55 (40%) wide12 (9%)long and wide33 (24%)Tongue base hyperplasia normal45 (76%) mild12 (20%) moderate2 (3%)Epiglottis form normal49 (69%)omega-shaped12 (17%) retroflected10 (14%)Occlusion Angle Class 113 (21%) Class 2 A1 (2%) Class 2B49 (78%) Class 30 (0%)Nasal septum deviation50 (63%)Turbinate hypertrophy31 (51%)
Table 2. Pre- and postoperative sleep study results and Patient-Reported outcome measures. Data are presented as mean ± standard deviation. Comparisons between pre- and postoperative values were performed using paired t-tests, with P values adjusted for multiple comparisons using the Benjamini-Hochberg methodPreoperativePostoperativeAbsolute DifferenceRelative Difference (%)p value adjustedEpworth Sleepiness Scale (0–24)8.4 ± 4.74.1 ± 3.0-4.4-52< 0.01Snoring Index (VAS 0–10)7.9 ± 2.03.3 ± 2.3-4.6-580.02Body mass index (kg/m2)28.6 ± 4.328.5 ± 4.100< 0.01Recording time (hours)7.2 ± 1.47.4 ± 1.10.340.08Apnea-hypopnea index (events/hour)23.8 ± 18.516.4 ± 14.9-7.4-31< 0.01Apnea index (events/hour)9.2 ± 12.94.2 ± 7.6-4.9-54< 0.01Central Apnea-hypopnea index (events/hour)2.5 ± 4.40.9 ± 1.6-1.6-630.01Oxygen desaturation index (events/hour)18.3 ± 18.213.2 ± 12.5-5.1-28< 0.01Mean oxygen saturation (%)93.3 ± 1.993.3 ± 1.9000.88Time below 90% oxygen saturation (%)6.1 ± 12.56 ± 13.2-0.1-20.88Cartwright Index1.8 ± 1.51.8 ± 1.3020.88Supine time (% of total sleep time)38.4 ± 24.939.8 ± 25.41.440.31Apnea-hypopnea index supine (events/hour)34.5 ± 24.826.2 ± 22.7-8.4-24< 0.01Oxygen desaturation index supine (events/hour)28.1 ± 24.221.5 ± 19.0-6.6-24< 0.01Heart rate (beats/minute)62.9 ± 7.464 ± 7.6120.12VAS, visual analog scale
Epworth sleepiness scale
Across the entire cohort, we observed a significant postoperative improvement in daytime sleepiness, with mean ESS scores decreasing from 8.4 ± 4.7 to 4.1 ± 3.0 (p < 0.01; Fig. 1a). Univariate linear regression analysis revealed that a higher preoperative ESS score was significantly associated with greater ESS reduction (β = 0.79; 95% CI: 0.68–0.90; p < 0.01; Online Resource Fig. S1). Uncorrected models initially indicated associations between ESS reduction and gender (Online Resource Fig. S2), snoring intensity, preoperative AHI (Online Resource Fig. S3), and preoperative apnea index; however, these associations were not significant after correction for multiple comparisons (Table 3). Multivariate analysis demonstrated that adding additional predictors did not enhance the accuracy beyond the univariate model. Notably, the ESS reduction did correlate with the AHI reduction (β = 0.07; 95% CI: 0.02–0.11; p = 0.004; Online Resource Fig. S4). However, because the reduction in AHI is only known after the surgery, it cannot serve as a predictor.
Among ESS responders, defined as those achieving a postoperative ESS score below 11 with at least a 50% ESS reduction from preoperative, a significant association with the preoperative ESS was found (odds ratio = 1.15; 95% CI: 1.06–1.25; p < 0.01, Online Resource Table S3). No other predictors or combination of predictors showed significant associations in univariate and multivariate analyses.
Fig. 1. Violin plots illustrating Pre- and Postoperative Values for the Epworth Sleepiness Scale (a) and Snoring Intensity on a Visual Analog Scale (b). Individual patient data points are represented by dots and connected by lines to show paired changes. Diamonds indicate the mean values of the whole cohort for pre- and postoperative measurements
Table 3. Univariate analysis for predictors of Epworth sleepiness scale reduction. Linear regression models were applied, and P values were adjusted for multiple comparisons using the Benjamini-Hochberg methodVariableEstimate with 95% CIp valuep value adjustedAge (years)0.00 (-0.07–0.06)0.940.97 Gender (female)
2.98 (0.34–5.61)
0.03 0.30Neck circumference (cm)-0.1 (-0.34–0.14)0.410.87Height (cm)-0.04 (-0.15–0.07)0.430.87Weight (kg)-0.03 (-0.09–0.03)0.310.83BMI (kg/m2)-0.06 (-0.27–0.15)0.570.92 Epworth Sleepiness Scale preoperative
0.79 (0.68–0.90)
< 0.01
< 0.01
Snoring (VAS) preoperative
0.45 (0.03–0.87)
0.04 0.30Impaired nasal breathing0.56 (-1.81–2.93)0.640.92Tonsil grade1.06 (0.05–2.07)0.040.30Friedman tongue position0.26 (-0.66–1.18)0.580.92Friedman stage-0.8 (-2.38–0.78)0.320.83Pharyngeal webbing0.34 (-0.74–1.42)0.540.92Uvula grade1.28 (-0.74–3.3)0.210.82Tongue base hyperplasia1.44 (-1.21–4.09)0.280.83Epiglottis form0.39 (-2.77–3.56)0.800.97Occlusion angle3.08 (-7.75–13.91)0.570.92Septal deviation-0.12 (-2.37–2.12)0.910.97Turbinate hypertrophy-0.13 (-2.59–2.33)0.920.97 Preoperative Sleep Testing Recording time (hours)-0.58 (-1.2–0.05)0.070.47 Apnea-hypopnea index (events/hour)
0.04 (0.00–0.08)
0.04 0.30 Apnea index (events/hour)
0.09 (0.02–0.15)
0.01 0.26Central Apnea-hypopnea index (events/hour)-0.27 (-0.64–0.09)0.140.59Oxygen desaturation index (events/hour)0.01 (-0.05–0.06)0.830.97Mean oxygen saturation (%)0.03 (-0.53–0.59)0.920.97Time below 90% oxygen saturation (%)-0.02 (-0.09–0.06)0.680.92Cartwright Index-0.19 (-0.65–0.27)0.420.87Supine time (% of total sleep time)0.01 (-0.02–0.04)0.370.87Apnea-hypopnea index supine (events/hour)0.02 (-0.01–0.05)0.240.83Oxygen desaturation index supine (events/hour)-0.01 (-0.05–0.03)0.670.92Heart rate (beats/minute)0.02 (-0.12–0.15)0.780.97
Snoring
We observed a significant postoperative reduction in snoring intensity across the entire cohort, decreasing from 7.9 ± 2.0 to 3.3 ± 2.3 (p < 0.01; Fig. 1b). Individuals with higher preoperative snoring intensity experienced a more pronounced reduction in snoring (β = 0.73; 95% CI: 0.54–0.92; p < 0.01; Table 4, Online Resource Fig. S5). Although uncorrected univariate correlations were identified between snoring reduction and both BMI (Online Resource Fig. S6) and Friedman Stage (Online Resource Fig. S7), these associations were no longer significant after correcting for multiple comparisons. Notably, the snoring reduction did not correlate with the AHI reduction (β = 0.007; 95% CI: -0.021–0.036; p = 0.63; Online Resource Fig. S8).
Snoring responders were defined as individuals achieving a postoperative VAS score of ≤ 3 with at least a 50% reduction from baseline. No significant predictors of snoring responders were identified (Online Resource Table S4).
Table 4. Univariate analysis for the snoring reduction. Linear regression models were applied, and P values were adjusted for multiple comparisons using the Benjamini-Hochberg methodVariableEstimate with 95% CIp valuep value adjustedAge (years)-0.02 (-0.06–0.03)0.510.95Gender (female)0.84 (-0.97–2.65)0.360.95Neck circumference (cm)-0.11 (-0.3–0.08)0.270.95Height (cm)0.02 (-0.05–0.08)0.650.95Weight (kg)-0.03 (-0.07–0.01)0.130.86 BMI (kg/m2)
-0.14 (-0.27 - -0.01)
0.04 0.56Epworth Sleepiness Scale preoperative0.11 (0.00–0.22)0.050.56 Snoring (VAS) preoperative
0.73 (0.54–0.92)
< 0.01
< 0.01 Impaired nasal breathing0.35 (-1.61–2.3)0.720.95Tonsil grade0.02 (-1.15–1.19)0.970.98Friedman tongue position1.12 (-0.80–3.04)0.250.95 Friedman stage
-1.44 (-2.39 - -0.48)
< 0.01 0.09Pharyngeal webbing0.06 (-1.08–1.21)0.910.98Uvula grade0.42 (-0.87–1.71)0.520.95Tongue base hyperplasia1.12 (-0.80–3.04)0.250.98Epiglottis form-0.09 (-2.98–2.79)0.950.98Occlusion angle1.38 (-5.59–8.34)0.690.95Septal deviation-0.5 (-2.3–1.3)0.580.95Turbinate hypertrophy-0.05 (-2.26–2.17)0.970.98 Preoperative Sleep Testing Recording time (hours)0.23 (-0.22–0.68)0.320.95Apnea-hypopnea index (events/hour)0.01 (-0.01–0.04)0.370.95Apnea index (events/hour)0.01 (-0.03–0.06)0.550.95Central Apnea-hypopnea index (events/hour)-0.19 (-0.43–0.05)0.120.86Oxygen desaturation index (events/hour)0.01 (-0.03–0.05)0.620.95Mean oxygen saturation (%)0.07 (-0.34–0.49)0.720.95Time below 90% oxygen saturation (%)-0.01 (-0.06–0.04)0.690.95Cartwright Index-0.26 (-0.8–0.29)0.350.95Supine time (% of total sleep time)0.00 (-0.02–0.02)0.740.95Apnea-hypopnea index supine (events/hour)0.01 (-0.02–0.03)0.550.95Oxygen desaturation index supine (events/hour)0.01 (-0.02–0.04)0.590.95Heart rate (beats/minute)0.03 (-0.06–0.12)0.540.95
Discussion
Across the entire cohort, we observe a significant improvement in PROMs, with a clinically relevant reduction of daytime sleepiness and snoring intensity following rfUPP + TE in adult patients. The observed improvements in ESS scores and snoring intensity corroborate findings from earlier studies [5, 11, 14]. In our analysis, higher preoperative ESS and snoring intensity scores emerged as the only significant predictors of postoperative reduction. Patients presenting with more pronounced daytime sleepiness or severe snoring preoperatively experienced more substantial symptom relief. Greater preoperative daytime sleepiness increased the odds ratio for being a responder on ESS, whereas snoring responders could not be predicted. Interestingly, no anatomical parameter or sleep-testing index consistently predicted improvements.
The multifactorial nature of subjective symptom relief likely explains this lack of clear anatomical and polysomnographic predictors. Daytime sleepiness and snoring intensity are influenced by numerous factors, including individual sensitivity, perception of sleep quality, lifestyle, psychological status, and even partner-reported sleep disturbances [3, 4, 6, 10]. These variables are typically not captured comprehensively by routine clinical examinations or polysomnography, emphasizing the complexity of accurately predicting surgical outcomes based solely on objective measurements.
Interestingly, objective improvements in AHI were associated with reduced daytime sleepiness, whereas the snoring improvements did not correlate. This might be explained by the finding that nocturnal hypoxemia is a causal factor for daytime sleepiness [27]. Snoring intensity is judged by the beholder’s ear and subject to the psychoemotional disposition of the bedpartner towards the snorer, as shown in the seminal article by Hoffstein et al. [28]. Subjective assessment of snoring has been shown to be highly reliable. However, bed partners might confuse snoring intensity with annoyance caused by nocturnal snoring [29]. For the ESS, the test-retest reliability is relatively low, which might confound the accuracy of the statistical analysis [30]. This further underscores the loose correlation between objective testing and PROMs [6, 8]. Further, night-to-night variability in sleep testing might limit the predictive power and correlation [31, 32].
Strengths
This study’s strengths include a relatively large and homogeneous patient cohort, comprehensive and systematic preoperative head and neck assessments, and the use of a standardized surgical technique. Importantly, the study is characterized by a structured and consistent postoperative follow-up protocol, incorporating validated and standardized questionnaires to capture PROMs reliably. This systematic approach enhances the robustness and clinical relevance of the findings.
Limitations
Our study has several limitations. Its retrospective and unblinded design introduces the risk of bias. A considerable proportion of patients were lost to follow-up. While no significant differences were observed between the groups, the results may still be negatively biased, as patients with symptom resolution might be less likely to attend follow-up consultations. The follow-up period was restricted to three months, limiting the ability to assess long-term PROMs. Some patients underwent concomitant nasal surgery, which may be a confounder, despite the sleep testing and PROM outcomes not differing between the groups. The surgical technique using rfUPP + TE may differ from other commonly used techniques, limiting our results’ generalizability. Moreover, the substantial variability inherent in objective sleep studies [31, 32] and subjective PROMs [28–30] may mask subtle predictive associations, warranting further prospective studies with larger cohorts. Due to this retrospective design, no additional PROMs, such as disease-specific quality of life, could be analyzed.
Future research
Future research should analyze a broader spectrum of PROMs to better depict disease-specific quality of life. Examining additional variables, such as psychometric and environmental factors, could improve patient selection, individualized patient counseling, and enhance surgical outcome predictions. Future research on sleep surgery should routinely incorporate PROMs as endpoints, as they are crucial for patients’ decision-making and essential for patient satisfaction.
Conclusion
While rfUPP + TE reliably improves daytime sleepiness and snoring, only baseline severity of symptoms predicted the degree of improvement. Anatomical features and sleep testing parameters did not consistently correlate with patient-reported symptoms. Acknowledging the multifactorial basis of daytime sleepiness and snoring is crucial when counseling patients preoperatively and setting realistic expectations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sundman J, Nerfeldt P, Fehrm J, Bring J, Browaldh N, Friberg D (2022) Effectiveness of tonsillectomy vs modified uvulopalatopharyngoplasty in patients with tonsillar hypertrophy and obstructive sleep apnea: the TEAMUP randomized clinical trial. JAMA Otolaryngol Neck Surg 10.1001/jamaoto.2022.3432. 10.1001/jamaoto.2022.3432 PMC 963459336326742 · doi ↗ · pubmed ↗
- 2Tschopp S, Tschopp K (2019) Tonsil size and outcome of uvulopalatopharyngoplasty with tonsillectomy in obstructive sleep apnea: tonsil size and outcome of UPPP with TE. 10.1002/lary.27899. The Laryngoscope 10.1002/lary.2789930848478 · doi ↗ · pubmed ↗
- 3Sundman J, Browaldh N, Fehrm J, Friberg D (2021) Eight-Year Follow‐up of modified uvulopalatopharyngoplasty in patients with obstructive sleep apnea. The Laryngoscope 131 10.1002/lary.28960.10.1002/lary.2896033405253 · doi ↗ · pubmed ↗
- 4World medical association declaration of Helsinki: ethical principles for medical research involving human subjects (2013). JAMA 310:2191. 10.1001/jama.2013.28105310.1001/jama.2013.28105324141714 · doi ↗ · pubmed ↗
- 5Buuren SV, Groothuis-Oudshoorn K (2011) Mice: multivariate imputation by chained equations in R. J Stat Softw 45. 10.18637/jss.v 045.i 03
- 6Tschopp S, Wimmer W, Caversaccio M, Borner U, Tschopp K (2021) Night-to-night variability in obstructive sleep apnea using peripheral arterial tonometry: a case for multiple night testing. J Clin Sleep Med jcsm 9300(jcsm 9300). 10.5664/jcsm.930010.5664/jcsm.9300 PMC 863634033783347 · doi ↗ · pubmed ↗