The effect of resistance inspiratory muscle training in the management of breathlessness in patients with thoracic malignancies: a randomised controlled trial
Meng-Yuan Li, Xian-Liang Liu, Bo Peng, Tao Wang, Li-Qun Yao, Hou-Qiang Huang, Wai Hang Kwok, Jing-Yu Benjamin Tan, Alex Molassiotis

TL;DR
This study found that resistance inspiratory muscle training can temporarily reduce breathlessness in patients with thoracic cancers, but long-term benefits are uncertain due to low adherence.
Contribution
The study provides new evidence on the short-term effectiveness of IMT for managing breathlessness in thoracic malignancy patients.
Findings
IMT led to a significant reduction in breathlessness severity at week 8, as measured by the Dyspnoea-12 scale.
Participants showed improved breathlessness scores at week 12, but no significant long-term effects were observed for other outcomes like anxiety or walking distance.
Low adherence to the IMT program suggests the need for strategies to improve long-term compliance.
Abstract
To assess the effects of resistance inspiratory muscle training (IMT) on breathlessness in patients with thoracic malignancies. This is a two-arm, non-blinded, randomised controlled trial (RCT). A total of 196 participants were randomly assigned (1:1) into two groups: a control group (routine care) and an intervention group (routine care + IMT training using a pressure threshold device). The intervention duration was 12 weeks with 30 min/day, 5 days/week. The primary outcome was breathlessness severity, assessed by the modified Borg scale (mBorg). Secondary outcomes were worst and average breathlessness over the past 24 h (assessed by the 11-point Numerical Rating Scale), breathlessness severity (assessed by the Dyspnoea-12, D-12), the 6-min walk distance (assessed by the 6-min walk test, 6MWT), quality of life (assessed by the St George’s Respiratory Questionnaire, SGRQ), and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
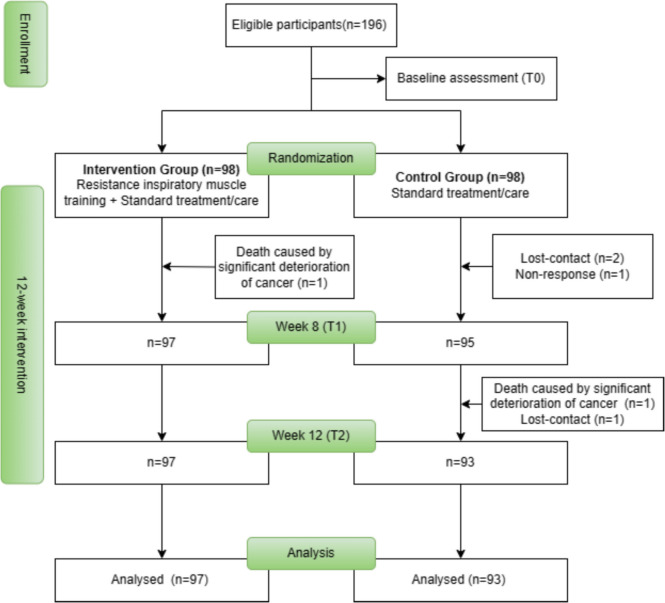 Figure 1
Figure 1- —University of Southern Queensland
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Obstructive Pulmonary Disease (COPD) Research · Cancer survivorship and care · Cystic Fibrosis Research Advances
Introduction
Thoracic malignancies have become a significant global health burden with high morbidity and mortality, particularly lung cancer (LC), which is the leading cause of cancer mortality worldwide [1]. In China, patients diagnosed with LC ranked first, with new cases of 815,000 and 714,000 deaths in 2020 [2]. Due to the cancer progression and side effects of cancer treatments, LC patients commonly experience breathlessness [3]. Reductions in expiratory and inspiratory muscle strength can persist up to 12 weeks following thoracotomy in LC [4]. Research has reported that the weighted grand mean prevalence of breathlessness in LC patients was 34.9% [5], which has a detrimental impact on overall well-being, and impedes patients from engaging in daily activities [6]. Management of breathlessness in LC patients is generally focusing on medication and oxygen as prescribed [7]. However, breathlessness tends to be more refractory to treatment than other symptoms (e.g., pain) and less responsive to medications, making it a poorly controlled symptom [8]. Considering the uncertainty of breathlessness occurrence, oxygen therapy may not always be readily accessible and self-administered when needed. Additionally, the utilisation of home oxygen therapy can be limited due to its high costs and side effects (e.g., risk of epistaxis related to the irritation of nasal cannula) [9].
Inspiratory muscle training (IMT) refers to a targeted strengthening of the inspiratory muscles by applying resistance during inspiration [10]. It has been used for respiration symptom relief since the 1980 s [10]. The most common method of providing IMT is inspiratory threshold pressure loading [11], which has demonstrated beneficial effects on quality of life (QoL), exercise capacity, and breathlessness in non-cancer respiratory diseases over a long time [12]. IMT requires participants to breathe against set resistance, which increases the workload of the breathing muscles. With continued practice and progressive resistance, IMT improves the strength and endurance of the inspiratory muscles [13]. Enhancement in inspiratory muscle strength and endurance could be in increasing the inspiratory flow, decreasing the inspiratory time, and improving the expiratory time, consequently reducing the sensation of breathlessness during daily activities [11]. In a clinical trial conducted by Liu et al. [13], the recovery of respiratory muscle strength was well documented in LC patients after a combination of IMT and aerobic exercise training. Considering the reduction of breathing muscles resulting from the long-term impact of cancer treatments, IMT could be a potentially encouraging intervention for managing breathlessness in patients with thoracic malignancies. Moreover, cancer and its treatment have numerous impacts that can be counteracted through IMT, potentially relieving breathlessness [14]. These include improvements in lung function, respiratory muscle sarcopenia, loss of chest mobility due to surgery, and pulmonary fibrosis caused by chest radiotherapy [15, 16].
A latest systematic review assessing the various breathing exercises on breathlessness and QoL in LC patients, highlighted the promising role of IMT in enhancing the well-being of these patients [17]. Another meta-analysis indicated that IMT is effective in improving pulmonary function in cancer patients, particularly highly recommending its application in LC patients [18]. However, IMT did not yield statistically significant results on exercise capacity and QoL due to the limited sample size and unsatisfactory methodology of the included studies [18]. Ambiguous results of IMT on exercise capacity, maximal inspiratory pressure, maximal expiratory pressure, and QoL were reported by one systematic review with only five trials on postoperative patients with LC [14]. In addition, strategies using the IMT for improving breathlessness management and QoL in LC patients have been reported in the literature [16, 19]. However, due to the limited sample size, and wide heterogeneity in the utilisation of IMT, full-scale and high-quality randomised controlled trials (RCTs) are needed to confirm the effects of IMT in patients with thoracic malignancies. To the best of our knowledge, no large-scale RCT has been conducted so far to assess IMT aiming to reduce breathlessness in thoracic malignancies. A pilot study in patients with clinically stable LC was conducted by Molassiotis et al. [16], showing that IMT was not only feasible, acceptable, and safe for LC patients, but also associated with statistical and clinical improvements in the breathlessness-related parameters, depression and QoL. Following the modification of the RCT study protocol, a fully powered RCT was conducted to draw definitive conclusions on the effects of IMT on breathlessness among patients with thoracic malignancies.
Methods
Design and participants
The study methods followed the previous pilot study [16] and the CONSORT guideline. A two-arm, non-blinded, RCT was utilised. Recruitment took place in the Affiliated Hospital of Southwest Medical University (Sichuan, Mainland China).
Adult participants were eligible for recruitment if they (1) were diagnosed with primary LC or mesothelioma (histological diagnosis); (2) have an expected prognosis (over 3 months) as determined by the clinicians; (3) have refractory breathlessness and have not responded to current treatment for the past two weeks as determined by the clinicians; and (4) have an oxygen saturation above 85% at rest. Participants were ineligible if they (1) were with unstable COPD and the condition was under acute or frequent exacerbation; (2) were rapidly worsening breathlessness and needed urgent medical intervention; (3) have palliative radiotherapy to the chest received within four weeks or chemotherapy within two weeks; and (4) were experiencing intractable cough and have unstable angina or clinically significant pleural effusion requiring drainage.
The estimation of sample size was based on the primary outcome of the modified Borg scale (mBorg) score. The change score of mBorg from baseline to 3-month assessment was 0.80 and the established minimally important difference was 1 according to the pilot study [16]. Since a 25% attrition was reported in the pilot study [16], the required sample size was 196 totally (98 in each group).
Randomisation and blinding
Two arms (a control arm and an IMT arm) were designed. An independent statistician prepared the computer-generated random sequence. After completion of the baseline assessment of an eligible participant, the investigator (responsible for recruitment) contacted the independent statistician to request the group allocation. Participants included in the study were told what was being applied. The blinding design of the participants, investigators, and outcome assessors was not achieved given that most of the outcome measures were self-reported and the participants were deemed as the outcome assessors. A single blinding design (outcomes assessor) was described in the registered clinical trial protocol, and this paper acknowledges this minor discrepancy.
Study interventions
All the participants received routine methods of care (‘standard treatment’ as indicated in the registered clinical trial protocol, which was utilised in both groups as usual care), including standard health education (pain management, medication management, exercise guidance, lifestyle adjustment) and regular follow-ups. Participants in the intervention group received additional IMT intervention. The IMT intervention was detailed in the published pilot study [16]. Participants in the IMT group used a threshold inspiratory muscle training device from Phillips Respironics for five days per week, 30 min per day, for 12 weeks. The daily 30-min training can be divided into two sessions. Before initiating the intervention, participants’ maximum inspiratory pressure (MIP) was measured by using an inspiratory pressure measuring instrument as a baseline. Then participants were required to perform 3–5 min of exercise under the Research Assistant’s supervision to assess whether they had encountered difficulties (e.g., tiredness or shortness of breath) in completing the entire session. The IMT exercise intensity was determined based on the measured participants’ MIP. Specifically, the initial training intensity started from 40% MIP, with a weekly increase of 5% until reaching 70% MIP as the maximum intensity [16]. To maintain the effectiveness of IMT usage, a nose clip was suggested to prevent patients from inhalation through the nose to overcome the resistance from the valve. If using a nose clip is uncomfortable for the participants, the participants were suggested to manually pinch the nostrils with their hands during the IMT exercise. The inspiratory duration lasted for 1.5 to 2 s, while the expiratory duration was extended to 6 s, maintaining an inhalation-to-exhalation (IE) ratio of 1:3 [20]. This aims to enhance tidal volume, reduce dead space ventilation, improve alveolar ventilation, decreases respiratory effort, and alleviates breathlessness symptoms [20]. Consequently, the respiratory rate was maintained at about 8 breaths per minute.
Study procedures
Participants’ recruitment was conducted at the outpatient clinic of study site. Eligible participants who provided written informed consent were recruited. Baseline assessments were performed before randomisation. Participants allocated to the intervention group received IMT training using a pressure threshold device. A study investigator explained and demonstrated how to use and adjust the exercise intensity until the participants mastered the skills with a return demonstration. During the intervention period, participants in the IMT group received weekly reminders to increase the IMT’s resistance level and concurrently monitor their exercise progress. Participants in the intervention group were also required to document their IMT practice sessions. Instruction videos on the use of the pressure threshold device were provided to the participants in the IMT group, ensuring that they could strengthen the IMT technique at home. Consistency in each stage of this study was maintained by a detailed protocol, constant supervision of the research activities, and regular meetings among the study investigators.
Demographic and clinical characteristics of patients were collected face-to-face at baseline (T1). All the clinical outcomes were assessed via either face-to-face (for participants who returned to the study site) or telephone (for those who were unable to return due to the COVID policies) immediately after the completion of the intervention (8-week, T2) and the completion of the follow-up (12-week, T3). Since all the subjective outcomes were self-administrated questionnaires, the participants were encouraged to complete the questionnaires independently. Only necessary interpretation was provided in a neutral way when the participants had confusions about terms or items in the questionnaires.
Outcome measures
Baseline assessment
The participants’ sociodemographic data, medical history, medication regimen, and other baseline data were collected via a predesigned baseline data collection form. The spirometry assessment at baseline was also recorded.
Primary outcome
Severity of breathlessness: modified Borg scale (mBorg)
The mBorg is a vertical 11-point scale, from ‘0’ (nothing at all) to ‘10’ (maximal) to assess the level of breathlessness at the time of assessment. A higher score represents a higher breathlessness level [21]. The within-groups minimal clinically important difference (MCID) of 1 point in the mBorg score was deemed to indicate a clinically significant change in breathlessness [21].
Secondary outcomes
Severity of breathlessness: Dyspnea-12 Questionnaire (D-12)
The D-12 obtained an overview of the severity of breathlessness, consisting of both physical aspect and affective aspect [22]. Each item was rated from ‘0’ (none) to ‘3’ (severe), with a total score range of 0 to 36. A higher score reflects a greater severity of breathlessness [22]. The D-12 has been widely used for the assessment of breathlessness in patients with lung disease [22]. The Chinese version of D-12 exhibited strong internal consistency, with Cronbach’s alpha coefficients of 0.83 in lung cancer patients [23].
Severity of breathlessness over ‘the past 24 h’: Numerical Rating Scale (NRS)
This study also used a 0–10 NRS (0 = no,10 = as bad as can be) to assess the ‘average’ level and ‘worst’ level of the severity of breathlessness and the distress caused by breathlessness over ‘the past 24 h’ [24]. The NRS has been validated and used for the severity of breathlessness [24].
Exercise capacity: the 6-min walk test (6MWT)
The exercise capacity was assessed using the 6-min walk test (6MWT), which is patient-friendly, well-validated, and exhibits strong correlations with lung function in clinical trials [25]. In accordance with the American Thoracic Society (ATS) guidelines, participants were directed to a quick walk back and forth and stop or rest as necessary on a demarcated 30-m linear path on a flat surface. At each minute, reminders of the time remaining were provided to participants to ensure consistency with standardized procedures [25]. Following the completion of 6 min, the test administrator recorded the 6-min walk distance (6MWD). During the baseline assessment, the 6MWT was conducted in person by the researcher who provided detailed instructions explaining the procedure and safety precautions. As the 6MWT is simple to administer, requiring no specialized equipment or advanced training [26], participants were therefore provided standardized instructions on how to self-administer the 6MWT at home using their phones during the COVID-19 outbreak. The instructions were as follows: (1) participants were instructed to wear comfortable clothing and supportive shoes; (2) choose a flat, straight walking path recorded in length; (3) a smartphone timer was set for a 6-min countdown; (4) the timer was started when the participant began walking, and they stopped immediately when the timer rang; (5) distance was recorded by measuring the number of laps completed along their designated walking path; and (6) participants were advised to have a family member or caregiver present during the test in case of any issues.
Health-related QoL: St George’s Respiratory Questionnaire (SGRQ)
The SGRQ was specifically designed to measure and quantify health-related status in patients with chronic airflow limitation, and it has been validated for assessing QoL in patients with lung disease (including lung cancer patients) [27, 28]. The SGRQ consists of 50 items with 76 weighted responses, yielding into ‘symptoms’, and ‘activity’, ‘impact’ sections [29]. The total score also summarizes the impact of the disease on overall health status ranging from 0–100, where a lower score indicates better health [29].
Emotional Status: Hospital Anxiety and Depression Scale (HADS)
The HADS is a 14-ite scale for measuring anxiety and depression. It has been validated in cancer patients [30]. The items are rated on a 4-point scale from 0 (not present) to 3 (considerable), with higher scores representing more anxiety/depression. The Mandarin Chinese version has a satisfactory psychometric property, with Cronbach’s alpha ≥ 0.840 in the total and subscales [30].
Data analysis
Data was analyzed using the IBM SPSS 25.0 software. The statistical significance was set at a *p-*value of < 0.05. The participants’ demographic and clinical characteristics were reported as frequencies and percentages or means and standard deviations. Categorical variables were analyzed using the chi-square test or independent t-test to conduct baseline comparisons. The description of normally and non-normally distributed continuous data was reported as mean (standard deviation [SD]) and median (interquartile range [IQR]), respectively. Mann–Whitney U test was conducted to compare non-parametric variables while independent t-test was used for the comparison of normally distributed variables. Generalized estimating equations (GEE) models were used to compare differences in the outcomes (mBorg, NRS, D-12, 6MWT, SGRQ, HADS) between the two groups across multiple time points (T1-T2-T3) with adjustment for potential confounding factors. The potential confounding factors are variables that were significantly different between the two groups at baseline (BMI, D-12 score) and other potential covariates (age, weight, smoking, exercise, insomnia) [31, 32]. The GEE model accounts for the following: (1) group effect: assumes the outcome varies based on group assignment, independent of time; (2) time effect: assumes the outcome varies over time, independent of group assignment; and (3) group-by-time effect (main effect): examines the interaction between group assignment and time, comparing the intervention group at later time points with both the baseline and the control group at all time points [33]. The group-by-time effect is the primary result in this analysis, indicating the divergence in outcome trajectories over time between groups. A modified intention-to-treat analysis was followed.
Results
Sociodemographic and clinical characteristics
A total of 196 participants were recruited and randomly allocated to each group (Fig. 1). The attrition rate was 3%. Table 1 shows the baseline characteristics of the participants. No statistically significant between-group differences were found in baseline characteristics except the total score of D-12 (P = 0.02) and BMI (P = 0.02) which were introduced as two of the potential confounders in the adjusted GEE model. In the IMT group, approximately one-third of participants (31.63%) adhered strictly to the IMT protocol. The remaining participants (68.37%) completed most of the required training sessions due to malfunctioning IMT devices and discontinued monitoring strategies resulting from the implementation of COVID-19 policies.Fig. 1CONSORT diagram for the study populationTable 1Baseline demographic and clinical characteristics of the participantsVariablesControl groupIntervention groupValueP**n (%)n (%)Educational background(n = 196, 98/98)No formal education9 (9.2)11 (11.2)2.28^A^0.81Primary school26 (26.5)24 (24.5)Secondary school33 (33.7)38 (38.8)High school/technical school12 (12.2)9 (9.2)Junior college8 (8.2)10 (10.2)Bachelor’s degree or above10 (10.2)6 (6.1)Gender (n = 196,98/98)Male50(51.0)41(41.8)1.66^A^0.20Female48(49.0)57(58.2)Marital status (n = 196, 98/98)Single1 (1.0)1 (1.0)0.00^A^1.00Married97 (99.0)97 (99.0)Occupation (n = 194, 98/96)Professional and technical personnel5(5.1)11 (11.5)4.30^A^0.37Labour worker29 (29.6)20 (20.8)Clerical or administrative worker4 (4.1)6 (6.3)No longer working39 (39.8)38 (39.6)Other21 (21.4)21 (21.9)Household income (RMB) (n = 178, 90/88) < 300054 (60.0)52 (59.1)1.43^A^0.703000–600030 (33.3)31 (35.2) > 6000–100006 (6.7)4 (4.5) > 10,0000 (0)1 (1.1)Source of healthcare insurance (n = 195, 98/97)New Rural Cooperative Medical System42 (42.9)46 (47.4)0.86^A^0.65Resident Medical Insurance/Employee Medical Insurance55 (56.1)49 (50.5)Self-paid1 (1.0)2 (2.1)BMI (n = 194,98/98)Underweight (< 18.5)9 (9.2)3 (3.1)5.64^A^0.13Normal/healthy weight (18.5 ~ 22.9)43 (43.9)42(42.9)Overweight (23 ~ 24.9)25 (25.5)21(21.4)Obese (≥ 25)21 (21.4)32 (32.7)Cancer stage (n = 183, 94/89)I63 (67.0)61 (68.5)5.63^A^0.47IIA4 (4.3)4 (4.5)IIB7 (7.4)3 (3.4)IIIA6 (6.4)9 (10.1)IIIB6 (6.4)2 (2.2)IIIC1 (1.1)0 (0)IV7 (7.4)10 (11.2)Surgery types (n = 169,87/82)Left upper lobectomy20 (23.0)26 (31.7)3.04^A^0.69Left lower lobectomy6 (6.9)6 (7.3)Right upper lobectomy28 (32.2)23 (28.0)Right lower lobectomy19 (21.8)14(17.1)Microwave ablation0 (0)1 (1.2)Other14 (16.1)12 (14.6)Hypertension (n = 195, 98/97)Yes19 (19.4)26 (26.8)1.51^A^0.22No79 (80.6)71 (73.2)Diabetes (n = 196,98/98)Yes4 (4.1)11 (11.2)2.60^A^0.11No94 (95.9)87 (88.8)Asthma (n = 196,98/98)Yes2 (2.0)2 (2.0)0.00^A^1.00No96 (98.0)96 (98.0)Pneumonectasis (n = 196,98/98)Yes3 (3.1)5 (5.1)0.13^A^0.72No95 (96.9)93 (94.9)Pulmonary tuberculosis (n = 196,98/98)Yes3 (3.1)3 (3.1)0.00^A^1.00No95 (96.9)95 (96.9)Heart diseases (n = 194,96/98)Yes7 (7.3)5 (5.1)0.40^A^0.53No89 (92.7)93 (94.9)Targeted therapy (n = 196,98/98)Yes23(23.5)23(23.5)0.00^A^1.00No75(76.5)75(76.5)Exercise (Hour/week) (n = 195, 98/97)0–279 (80.6)78 (80.4)1.36^A^0.723–411 (11.2)14 (14.4)5–66 (6.1)3 (3.1)More than 62 (2.0)2 (2.1)Smoking (n = 195, 98/97)Never smoked64 (65.3)65 (67.0)0.35^A^0.84Current smoking2 (2.0)1 (1.0)Previous smoking32 (32.7)31 (32.0)Alcohol consumption (n = 196, 98/98)Yes34 (34.7)37 (37.8)0.20^A^0.66No64 (65.3)61 (62.2)Insomnia (n = 196, 98/98)Yes38 (38.8)34 (34.7)0.35^A^0.55No60 (61.2)64 (65.3)**Mean ± SD*Mean ± SDAge (n = 196, 98/98)58.8 ± 5.1058.78 ± 9.750.05^B^0.96BMI index22.64 ± 2.7923.63 ± 3.27 − 2.28^B^0.02Blood oxygen level (%) (n = 196,98/98)97.58 ± 1.4797.63 ± 1.374870.50^C^0.856MWD (n = 194, 96/98)389.82 ± 60.90393.04 ± 57.454830.00^C^0.75mBorg score (n = 195, 97/98)4.25 ± 1.714.21 ± 1.364848.50^C^0.80SGRQ total score (n = 196, 98/98)27.06 ± 12.7229.29 ± 13.395294.50^C^0.22HADS-D score (n = 191, 94/97)1.74 ± 2.511.92 ± 2.594653.00^C^0.80HADS-A score (n = 195, 97/98)2.96 ± 2.423.19 ± 2.914746.00^C^0.99D-12 total score (n = 192, 95/97)7.13 ± 3.788.16 ± 3.935537.50^C^0.02NRS-worst score (n = 195, 97/98)4.36 ± 2.234.53 ± 1.944979.00^C^0.56NRS-average score (n = 195, 97/98)2.54 ± 1.352.54 ± 1.264805.00^C^0.89^A^, Chi square test; ^B^, independent t-test; ^C^, Mann–Whitney U test; *, including housewife, unemployment, and retired; 6MWD, 6-min walk distance; mBorg, modified Borg scale; SGRQ, St George’s Respiratory Questionnaire; HADS, Hospital Anxiety and Depression Scale; D-12, Dyspnea-12 Questionnaire; NRS-worst, worst breathlessness over the past 24 h assessed by the Numerical Rating Scale; NRS-average, average breathlessness over the past 24 h assessed by the Numerical Rating Scale
Primary outcome
mBorg
Significant within-group differences were found in both the intervention group and control group, with its mBorg score at T2 and T3 being significantly lower than the score at baseline (all P < 0.05, Table 2), suggesting the breathlessness was reduced over time. The observed change in mBorg score in the IMT group at both T2 and T3 reached the minimally important clinical difference (MCID) of 1, while the MCID of mBorg score in the control group was observed until at T3. Group-comparison showed that the mBorg score of the control group was significantly higher (worse breathlessness) than the IMT group at T2 (P = 0.002). The group-by-time effect was not significant for the mBorg score (Table 3). Table 2. Group-effect and time-effect of intervention on outcomes by adjusted GEE modelOutcomeTimepointComparisonAdjustedMDSEEF \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$${\chi }^{2}$$\end{document} PmBorgT1IG VS. CG − 0.3000.190.222.460.117T2IG VS. CG − 0.5150.160.459.790.002T3IG VS. CG − 0.2400.160.212.180.140IGT3 VS. T2 − 0.1250.080.232.510.113T3 VS. T1 − 0.6630.130.7224.83** < 0.001T2 VS. T1 − 0.5380.100.7628.20 < 0.001CGT3 VS. T2 − 0.4000.070.7828.79 < 0.001T3 VS. T1 − 0.7230.120.8534.10 < 0.001T2 VS. T1 − 0.3240.130.376.520.011D-12-totalT1IG VS. CG0.9670.460.304.340.037T2IG VS. CG − 0.3040.420.110.530.468T3IG VS. CG − 0.4400.420.151.100.294IGT3 VS. T2 − 0.4340.130.4811.130.001T3 VS. T1 − 2.7430.321.2474.09 < 0.001T2 VS. T1 − 2.3090.311.0654.17 < 0.001CGT3 VS. T2 − 0.2980.170.263.180.075T3 VS. T1 − 1.3360.410.4810.620.001T2 VS. T1 − 1.0380.360.428.320.004D-12-physicalT1IG VS. CG0.7160.370.283.730.053T2IG VS. CG − 0.3020.370.120.660.415T3IG VS. CG − 0.4160.360.171.310.253IGT3 VS. T2 − 0.4990.120.6017.36 < 0.001T3 VS. T1 − 2.4060.261.3487.99 < 0.001T2 VS. T1 − 1.9070.231.1766.31 < 0.001CGT3 VS. T2 − 0.3850.140.407.450.006T3 VS. T1 − 1.2750.310.6117.38 < 0.001T2 VS. T1 − 0.8900.260.4911.460.001D-12-emotionnalT1IG VS. CG0.2670.190.201.970.160T2IG VS. CG − 0.0030.11 < 0.01 < 0.010.977T3IG VS. CG − 0.0390.120.050.110.740IGT3 VS. T20.0510.040.201.930.164T3 VS. T1 − 0.3640.150.355.950.015T2 VS. T1 − 0.4150.150.417.960.005CGT3 VS. T20.0860.050.253.030.082T3 VS. T1 − 0.0590.160.050.130.714T2 VS. T1 − 0.1450.150.140.900.344NRS-worstT1IG VS. CG0.0340.270.020.020.902T2IG VS. CG − 0.2470.200.181.530.217T3IG VS. CG0.1010.190.080.290.588IGT3 VS. T2 − 0.0140.080.030.030.859T3 VS. T1 − 0.3900.170.335.260.020T2 VS. T1 − 0.3800.150.376.770.009CGT3 VS. T2 − 0.3600.090.5614.69 < 0.001T3 VS. T1 − 0.4600.160.418.060.004T2 VS. T1 − 0.1000.150.100.440.507NRS-averageT1IG VS. CG − 0.1530.170.130.790.373T2IG VS. CG − 0.0570.130.060.180.674T3IG VS. CG0.0940.120.120.650.421IGT3 VS. T2 − 0.1260.070.273.600.058T3 VS. T1 − 0.1660.140.171.450.228T2 VS. T1 − 0.0410.120.050.120.734CGT3 VS. T2 − 0.2800.070.6016.65 < 0.001T3 VS. T1 − 0.4100.120.5112.23 < 0.001T2 VS. T1 − 0.1370.130.151.140.2856MWDT1IG VS. CG9.5807.570.181.600.206T2IG VS. CG10.9707.170.232.340.126T3IG VS. CG8.2187.900.161.080.298IGT3 VS. T27.7504.210.283.400.065T3 VS. T118.4576.430.428.230.004T2 VS. T110.7074.810.324.960.026CGT3 VS. T210.5023.350.479.810.002T3 VS. T119.8195.530.5312.86 < 0.001T2 VS. T19.3174.540.304.200.040HADS-AT1IG VS. CG − 0.0770.370.030.040.836T2IG VS. CG0.0790.320.040.060.807T3IG VS. CG0.0880.310.040.080.775IGT3 VS. T2 − 0.2400.130.283.670.055T3 VS. T1 − 0.1730.310.080.300.582T2 VS. T10.0670.300.030.050.821CGT3 VS. T2 − 0.2490.130.283.650.056T3 VS. T1 − 0.3380.270.181.550.213T2 VS. T1 − 0.0880.260.050.110.736HADS-DT1IG VS. CG − 0.1770.320.080.310.581T2IG VS. CG − 0.2520.230.161.160.282T3IG VS. CG0.0090.250.01 < 0.010.971IGT3 VS. T20.0930.110.120.760.385T3 VS. T1 − 0.1630.290.080.310.577T2 VS. T1 − 0.2560.280.130.840.361CGT3 VS. T2 − 0.1680.110.222.210.137T3 VS. T1 − 0.3490.300.171.370.241T2 VS. T1 − 0.1810.280.090.410.524SGRQ-totalT1IG VS. CG0.8381.160.100.530.469T2IG VS. CG1.1140.850.191.700.193T3IG VS. CG0.5560.820.100.460.497IGT3 VS. T20.2540.430.090.360.550T3 VS. T1 − 0.2811.010.040.080.781T2 VS. T1 − 0.5360.860.090.390.532CGT3 VS. T20.8130.460.263.170.075T3 VS. T10.0011.04 < 0.01 < 0.010.999T2 VS. T1 − 0.8111.030.110.620.430SGRQ-symptomT1IG VS. CG1.0971.740.090.400.527T2IG VS. CG3.0551.690.263.270.070T3IG VS. CG1.4151.610.130.770.381IGT3 VS. T2 − 2.4430.820.438.890.003T3 VS. T1 − 1.8791.510.181.550.213T2 VS. T10.5641.380.060.170.684CGT3 VS. T2 − 0.8030.690.171.370.243T3 VS. T1 − 2.1971.520.212.080.149T2 VS. T1 − 1.3941.470.140.900.342SGRQ-activityT1IG VS. CG1.5691.670.130.890.346T2IG VS. CG0.4421.060.060.170.676T3IG VS. CG0.1801.020.030.030.859IGT3 VS. T20.0270.560.01 < 0.010.962T3 VS. T1 − 1.0021.200.120.700.404T2 VS. T1 − 1.0281.090.140.890.345CGT3 VS. T20.2890.580.070.250.618T3 VS. T10.3881.300.040.090.765T2 VS. T10.0991.300.010.010.939SGRQ-impactT1IG VS. CG0.4341.210.050.130.719T2IG VS. CG0.6480.960.100.450.502T3IG VS. CG0.6370.910.100.490.483IGT3 VS. T21.2700.480.387.040.008T3 VS. T10.5051.200.060.180.675T2 VS. T1 − 0.7651.050.100.530.467CGT3 VS. T21.2810.530.355.930.015T3 VS. T10.3021.260.030.060.811T2 VS. T1 − 0.9781.160.120.710.401 IG, intervention group; CG, control group; NRS-worst, worst breathlessness over the past 24 h assessed by the Numerical Rating Scale; NRS-average, average breathlessness over the past 24 h assessed by the Numerical Rating Scale; SGRQ, St George’s Respiratory Questionnaire; 6MWD, 6-min walk distance; HADS, Hospital Anxiety and Depression Scale.Table 3. Group-by-time of intervention on outcomes by adjusted GEE modelOutcomesTime pointIntervention groupControl groupAdjusted group timeMeanSDMeanSD \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\beta$$\end{document} 95%CI PmBorg^A^T14.211.364.251.71T23.041.323.651.70 − 0.21 − 0.53, 0.100.175T32.791.513.101.620.06 − 0.29, 0.410.734D-12-TOTALT18.163.937.133.78T25.203.435.723.60 − 1.27 − 2.15, − 0.390.005T34.663.135.053.16 − 1.41 − 2.35, − 0.460.004D-12-physical*T17.322.856.612.79T25.042.775.513.07 − 1.02 − 1.66, − 0.370.002T34.492.554.862.67 − 1.13 − 1.86, − 0.400.002**D-12-affectiveT10.821.730.481.53T20.160.900.210.89 − 0.27 − 0.69, 0.150.208T30.160.850.190.88 − 0.31 − 0.73, 0.120.160NRS-worst^A^T14.531.944.362.23T23.561.433.941.92 − 0.28 − 0.69, 0.130.176T33.421.463.461.720.07 − 0.38, 0.510.767NRS-average^A^T12.541.262.541.35T21.941.022.121.490.10 − 0.22, 0.410.550T31.731.051.711.270.25 − 0.08, 0.570.1406MWD^B^T1393.0457.45389.8260.90T2418.7357.97408.6260.651.39 − 11.75, 14.530.836T3430.2258.30420.3563.92 − 1.36 − 17.95, 15.230.872HADS-A^C^T13.192.912.962.42T22.542.422.642.590.16 − 0.55, 0.860.666T32.272.292.302.390.17 − 0.57, 0.90.662HADS-D^C^T11.922.591.742.51T20.972.341.172.26 − 0.08 − 0.75, 0.60.827T30.902.030.851.860.19 − 0.51, 0.890.603SGRQ-total^D^T129.2913.3927.0612.72T221.5010.5122.8811.530.28 − 1.93, 2.480.807T320.4311.0920.9511.36 − 0.28 − 2.52, 1.950.804SGRQ—symptom^D^T124.9413.4123.0015.37T219.9114.2019.1112.501.96 − 1.68, 5.590.291T316.6113.7916.7512.000.32 − 3.28, 3.920.863SGRQ—activity^D^T146.1816.2143.1215.56T237.3011.1139.7413.15 − 1.13 − 4.23, 1.980.477T336.0711.6637.0512.01 − 1.39 − 4.53, 1.750.386SGRQ—impact^D^T120.8514.6118.9812.58T212.8111.4914.3711.850.21 − 2.34, 2.760.869T312.5511.8212.9712.480.20 − 2.43, 2.830.880^A^Adjusted for age, BMI, smoking, exercise, HADS-total, and D-12 total scores( adjusted for age, BMI, smoking, exercise, HADS-total score)^B^Adjusted for age, BMI, gender, and D-12 total scores^C^Adjusted for age, BMI, cancer stage, surgery types, diabetes, and D-12 total score^D^Adjusted for age, BMI, occupation, exercise, source of healthcare insurance, insomnia, mBorg score, D-12 total score, NRS-average score, NRS-worst score, and HADS total scoreNRS-worst, worst breathlessness over the past 24 h assessed by the Numerical Rating Scale.NRS-average, average breathlessness over the past 24 h assessed by the Numerical Rating Scale.SGRQ, St George’s Respiratory Questionnaire.6MWD, 6-min walk distance.
Secondary outcomes
D-12
In the IMT group, the D-12 total score, physical subscale score, and affective subscale score at T2 and T3 were significantly lower than the scores measured at T1 (all P < 0.05, Table 2), suggesting improvement of breathlessness severity. In the control group, only the D-12 total score and physical score at T2 and T3 were significantly lower than the scores measured at T1 (all P < 0.05, Table 2). No significant between-group difference was found at each time point for D-12 total, physical, or affective aspects (all P > 0.05) (Table 3). The significantly greater decreases in D-12 total and D-12 physical scores were seen in the IMT group at T2 (Ptotal= 0.005, Pphysical = 0.002) and T3 (Ptotal = 0.004, Pphysical = 0.002) compared to the control group (Table 3).
NRS: worst and average breathlessness over the past 24 h
No significant group-effect and group-by-time effect of NRS-worst and NRS-average scores were observed across time (all P > 0.05, Tables 2 and 3). The NRS-worst score at T1 was significantly higher than the scores at T2 and T3 in the IMT group (all P < 0.05, Table 2). The within-group difference of NRS-worst score in the control group was significant only between T3 and T1 (P = 0.004, Table 2). No time-effect was observed in the NRS-average score in the IMT group, while the NRS-average score at T1 was significantly lower than T3 in the control group (P < 0.001, Table 2). The within-group comparisons suggested the gradually alleviated worst breathlessness severity in both groups.
6MWD
The 6MWD increased in the IMT group over time, showing a significantly better exercise capacity at T2 and T3 compared with T1 (all P < 0.05, Table 2). Similar results were found in the control group (all P < 0.05, Table 2). However, there were no significant differences in 6MWD for between-group comparison (Table 2), indicating no changes in exercise capacity after IMT intervention. The group-by-time effect was not significant for the 6MWD (Table 3).
HADS
No significant group-effect, time-effect, and group-by-time interaction effect was observed in the scores of the HADS-A and HADS-D within the adjusted GEE module (Table 3).
SQRG
No significant group-effect, time-effect, and group-by-time interaction effect was observed in the scores of the SQRG-total and subscale within the adjusted GEE module (Table 3).
Discussion
Findings of this large-scale RCT demonstrated that IMT potentially supports the improvement of breathlessness severity (mBorg and D-12) in patients with thoracic malignancies. Further identification of the sustained effect of IMT on breathlessness is necessary, mainly due to the suboptimal adherence to the intervention. Yet these findings have crucial implications in efforts to manage breathlessness among this population.
The National Institute for Health and Clinical Excellence (NICE) recommended nonpharmacological interventions as the standard care for breathlessness in patients with LC [3]. However, high-intensity interventions (e.g., intensive exercise) impose a significant burden on patients with LC and are often difficult to sustain in many cases with breathlessness [34]. IMT provides a relatively low burden on LC patients, aiming to enhance both inspiratory and expiratory muscle performance through targeted training [14, 18]. As shown by the results of this study, after IMT, there was a significant decrease in the severity of breathlessness in a short-term (8 weeks). One explanation could be that the IMT potentially improved the inspiratory muscles at a mechanical disadvantage and optimised the pattern of thoracoabdominal motion with a higher level of inspiratory resistance. Also, the improved breathing during the IMT practice can improve breathlessness as well [35]. This finding aligns with the results of a retrospective cohort study which examined the efficacy of IMT in a consistent inspiratory pressure training load alongside exercise therapy among advanced LC patients experiencing breathlessness [19].
The current study only highlights the relatively short-term effects of IMT in alleviating breathlessness, the suboptimal compliance of the participants might be one of the attributing factors. One major barrier to adherence was the inability of participants to return to the study hospital for spirometry assessments and follow-ups due to the constraints imposed by COVID-19 policies. Strategies to improve adherence were classified into four types: technical solutions (such as decreased frequency and intensity); educational programs; behavioral interventions; and social support interventions [36]. The updated IMT protocol used in this study has been divided into two sessions and the intensity has been built up slowly according to participants’ tolerance. Future studies can include some behavioral change components to improve participants’ adherence further, for example, more effective reminders, regular monitoring, or reward-based initiation. The protocol could be modified to provide in-person home visits as an option, which could help with subsequent tracking effectively. Also, integrating some social platforms, such as the WeChat App, into self-management intervention could be another promising strategy for improving adherence. Additionally, the between-group differences in D-12 total score and BMI at baseline in this study indicated the benefits of using stratified randomisation in future studies to minimize statistical bias.
This study found no significant group-time interaction effects on the QoL, consistent with two systematic reviews showing that the effects of IMT on QoL among LC patients remain ambiguous [14, 18]. QoL of patients with thoracic malignancies may be impacted by multiple factors (e.g., the severity and the number of cancer-related symptoms, detreated lung function etc.), which may reflect differently in a subjective measure of the QoL [37]. The findings of this study on anxiety and depression were the same as previous studies, indicating that breathing exercise programs (including IMT and incentive deep-breathing exercise) could not significantly improve the emotional status of patients with LC [34]. However, an undeniable fact is that high levels of anxiety and depression in patients with LC are primarily attributed to progressive disease and worsening symptoms in LC patients [38, 39]. Also, anxiety and depression were regarded as factors associated with dropout and non-adherence with IMT in previous literature [40]. Thus, a combination of psychological support (e.g., cognitive-behavioral therapy) with the IMT intervention could be considered in future studies to promote participants’ engagement and maximise the interventional effects among this population.
In the pilot study, spirometry was used to assess lung function but was excluded from the current trial due to two reasons: (a) the pilot study indicated no change in lung function at any assessments, suggesting minimal expected improvements in lung function among this population with advanced cancer. Thus, the preservation of stable breathlessness emerges as a critical concern. (b) Current literature consistently shows a lack of association between lung function and perceived breathlessness improvement [41]. Given this insight, the current study included the 6MWT based on the expert’s recommendations. A meta-analysis showed similar findings, indicating that breath exercise (including IMT intervention) did not improve the 6MWD in LC patients undergoing surgery [42]. A retrospective pilot study has reported conflicting findings, suggesting that IMT combined with pulmonary rehabilitation appears effective on exercise capacity in non-small cell LC patients receiving radiotherapy [43]. Additionally, a recent RCT observed a 6-week IMT combined with aerobic exercise led to improved exercise capacity (measured by 6MWT) in LC patients after surgery [13]. These results could potentially be attributed to the sub-optimal adherence to the IMT intervention and the heterogeneity of subsequent self-assessment of 6MWD using a phone at home. To overcome this challenge, it would be advisable for future studies to encourage patients to visit the hospital for a standardized measurement. Alternatively, employing healthcare practitioners or trained researchers for home or community-based evaluations could enhance the accuracy of assessments.
Strengths and limitations
To our knowledge, this study represents the first large-scale RCT to thoroughly investigate the effects of IMT among patients with thoracic malignancies. This study focuses on the patients’ self-practice at home, indicating a practical combination of the intervention into their daily care routines. The adherence to IMT practice was reported by diary alone across the COVID-19 outbreak, limiting interpretation of results. The incorporation of electronic monitoring has been suggested to assess adherence and is considered the ‘gold standard’ for measuring adherence in similar interventions [44]. Due to resource constraints, the blinding of participants was not achieved. Although the 6MWT is simple to self-administer with standardized instructions provided, having this test at home without direct supervision during the COVID-19 outbreak may affect the consistency and generalizability of the results. Also, given that the 6MWD tends to increase after 3 walks due to a learning effect [45], 1 to 2 practice tests are suggested before determining an individual’s exercise capacity in future studies. Future studies should consider adopting a sham-controlled design, such as instructing participants to use the same device with no or minimal resistance, to further strengthen the internal validity and minimise potential bias.
Conclusions
The IMT intervention potentially reduced breathlessness in patients with thoracic malignancies in the short term. Further study could incorporate a follow-up and advanced monitoring strategy to better explore its long-term effects on breathlessness in patients with thoracic malignancies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization (2023) Lung Cancer. https://www.who.int/news-room/fact-sheets/detail/lung-cancer . Accessed 11 Apr 2024
- 2National Institute for Health and Care Excellence (2023) Lung cancer: diagnosis and management. www.nice.org.uk/guidance/ng 122. Accessed Jan 2024 31211540 · pubmed ↗
- 3Lo SB, Ruprecht AL, Post KE et al (2024) Dyspnea-related dimensions and self-efficacy: Associations with well-being in advanced lung cancer. J Pain Symptom Manage 67(5):366–374. 10.1016/j.jpainsymman.2024.01.03210.1016/j.jpainsymman.2024.01.032PMC 1103223538307373 · doi ↗ · pubmed ↗
- 4Dy SM, Lorenz KA, Naeim A et al (2008) Evidence-based recommendations for cancer fatigue, anorexia, depression, and dyspnea. J Clin Oncol 26(23):3886–3895. 10.1200/JCO.2007.15.952510.1200/JCO.2007.15.952518688057 · doi ↗ · pubmed ↗
- 5Geddes E, Reid WD, Brooks D et al (2010) A primer on inspiratory muscle trainers. Available at: http://dev.ersnet.org/uploads/Document/WEB_CHEMIN_419_1163420850.pdf. Accessed 13 Jan 2025
- 6Wang X, Ma X, Yang M et al (2022) Proportion and related factors of depression and anxiety for inpatients with lung cancer in China: a hospital-based cross-sectional study. Support Care Cancer 30(6):5539–5549. 10.1007/s 00520-022-06961-310.1007/s 00520-022-06961-3PMC 904632935318530 · doi ↗ · pubmed ↗
- 7Vestbo J, Hurd SS, Agustí AG et al (2013) Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med 187(4): 347–365. 10.1164/rccm.201204-0596 PP 10.1164/rccm.201204-0596 PP 22878278 · doi ↗ · pubmed ↗