Endoscopic removal of a large rectal foreign body using an endoscopic retrograde cholangiopancreatography guidewire snare
Kuangjing Wang, Yuan Wang, Zhengyuan Cheng, Haitao Wang, Min Wang, Yingzhou Shen

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
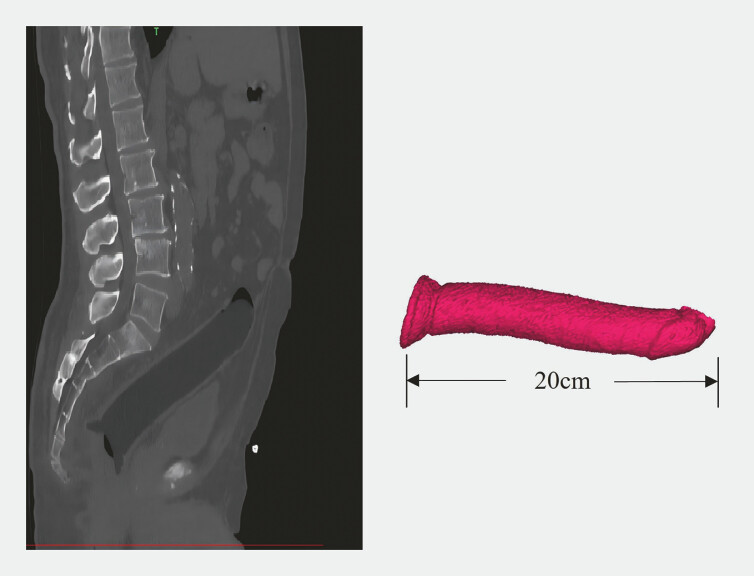 Fig. 1
Fig. 1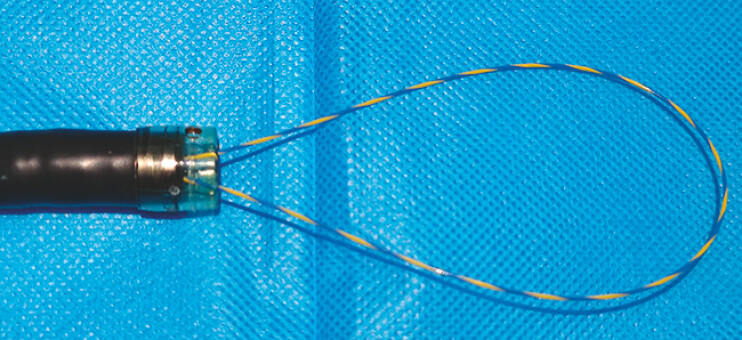 Fig. 2
Fig. 2 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Esophageal and GI Pathology · Hemostasis and retained surgical items
Rectal foreign bodies are a common presentation in emergency departments, predominantly observed in males and often associated with masturbation or sexual practices 1 2 . Endoscopic removal using a snare is the most common approach, but this method often fails for larger, smoother objects 3 4 . In this report, we report a case of successful removal of a rectal foreign body using a self-made snare, which was created by folding a 0.035-inch, 460-cm guidewire into a loop ( Video 1 ).
Endoscopic removal of a large rectal foreign body using an ERCP guidewire snare.Video 1
A 68-year-old man presented to the emergency department 8 hours after unsuccessful attempts to remove a foreign body he had inserted into his rectum. Abdominal CT and 3D reconstruction revealed a large foreign body lodged in the left colon, approximately 20 cm in length with an enlarged tail segment ( Fig. 1 ). Emergency colonoscopy confirmed its presence 15 cm from the anus.
The CT imaging of foreign body. Abdominal CT and 3D reconstruction revealed a large foreign body lodged in the left colon, approximately 20 cm in length with an enlarged tail segment.
Initial attempts to remove the object using foreign body forceps and a snare were unsuccessful due to the object’s smooth surface and the significant resistance it presented. Similarly, a standard 40-mm polypectomy snare failed to grasp the distal end of the object because of its size. To address this, we designed a novel snare device using an endoscopic retrograde cholangiopancreatography (ERCP) guidewire ( Fig. 2 ). A 0.035-inch, 460-cm guidewire was folded, and both ends were inserted retrogradely through the endoscopic accessory channel. This design allowed for adjustable snare diameter based on the foreign body’s size.
The self-made snare. A 0.035-inch, 460-cm ERCP guidewire was folded, and both ends were inserted retrogradely through the endoscopic accessory channel to form a snare. Abbreviation: ERCP, endoscopic retrograde cholangiopancreatography.
Using this self-designed device, we carefully secured the distal edge of the object and successfully extracted it. The foreign body was identified as a silicone penile prosthesis measuring approximately 200 mm in length and 50 mm in diameter ( Fig. 3 ).
The foreign body. The foreign body was identified as a silicone penile prosthesis measuring approximately 20 cm in length and 5 cm in diameter.
Endoscopy_UCTN_Code_TTT_1AQ_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maddah G Abdollahi A Tavassoli A An uncommon problem: Overcoming the challenges of rectal foreign bodies-A case series and literature review Clin Case Rep 202311 e 831310.1002/ccr 3.831338089487 PMC 10714057 · doi ↗ · pubmed ↗
- 2Ye H Huang S Zhou Q Migration of a foreign body to the rectum: A case report and literature review Medicine (Baltimore)201897 e 1151210.1097/MD.0000000000011512 PMC 607619429995819 · doi ↗ · pubmed ↗
- 3Morais R Marques M Macedo G Endoscopic treatment of a foreign body-associated colonic perforation Int J Colorectal Dis 20203516516710.1007/s 00384-019-03465-131820075 · doi ↗ · pubmed ↗
- 4Chilakamarry S Klipfel AA. Novel Approach to Removal of Rectal Foreign Bodies Dis Colon Rectum 202164 e 368e 37010.1097/DCR.000000000000204833769318 · doi ↗ · pubmed ↗