The combination of three advanced endoscopic techniques achieves recanalization of anastomotic stenosis after pancreatogastrostomy
Shan-Shan Hu, Jie Hou, Rui Huang, Wei-Hui Liu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
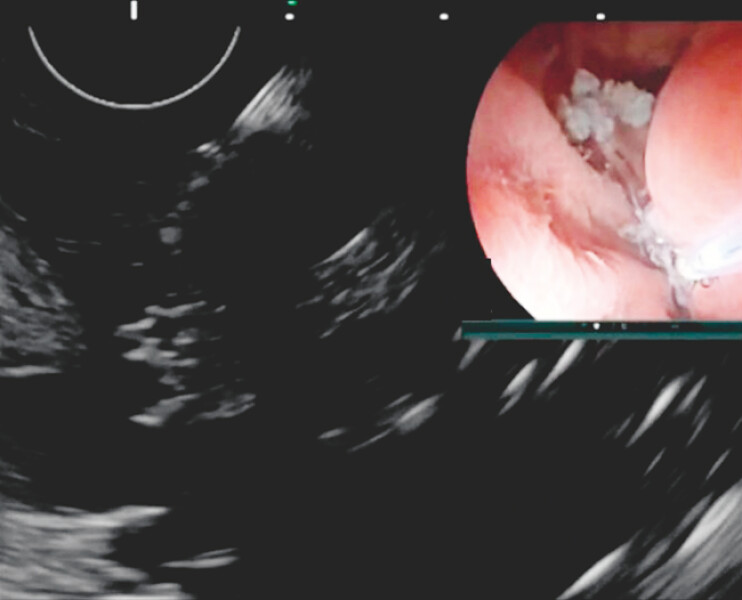 Fig. 1
Fig. 1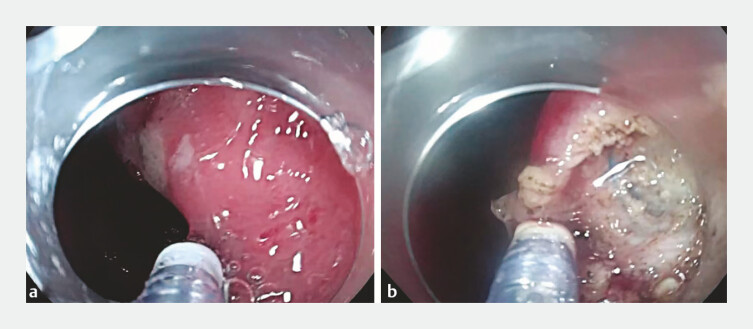 Fig. 2
Fig. 2 Fig. 3
Fig. 3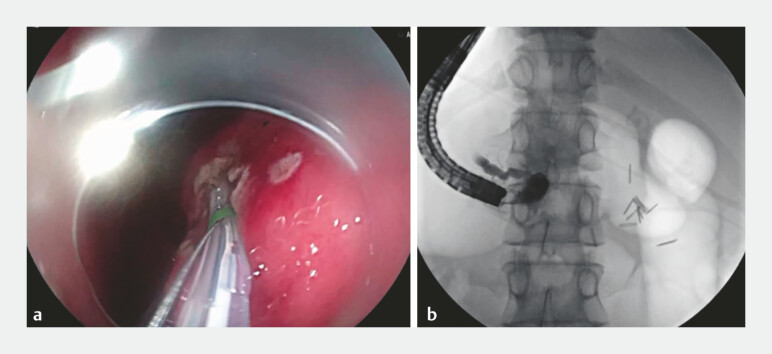 Fig. 4
Fig. 4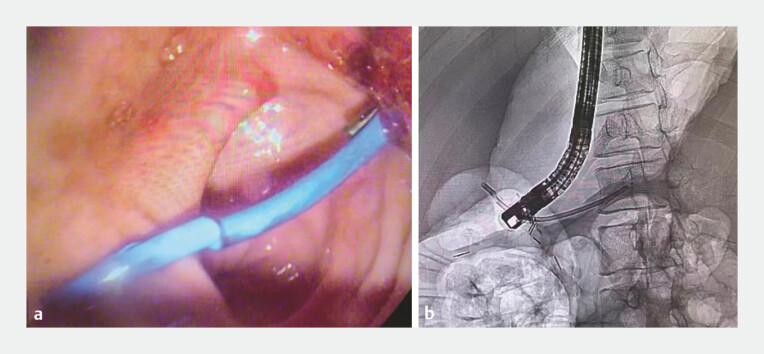 Fig. 5
Fig. 5- —Science & Technology Department of Sichuan Province
- —Sichuan Medical and Health Care Promotion Institute
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Gallbladder and Bile Duct Disorders · Esophageal and GI Pathology
With the rise in cases of pancreaticogastrostomy, managing anastomotic stenosis has become particularly challenging. The most prevalent method, endoscopic ultrasound-guided pancreatic duct drainage (EUS-PD) surgery 1 2 3 , currently faces two main issues: one is the limited success rate of the procedure, and the other is the difficulty in achieving the widest possible drainage of pancreatic juice 4 . Here, we present a case of an anastomotic stricture following pancreaticogastrostomy, successfully treated by recanalizing the original stricture using a combination of three advanced endoscopic techniques, offering a potential approach for managing similar cases ( Video 1 ).
The combination of three advanced endoscopic techniques achieves recanalization of anastomotic stenosis after pancreatogastrostomy.Video 1
A male patient underwent laparoscopic duodenum-preserving pancreatic head resection with pancreaticogastrostomy for a pancreatic head hamartoma. Recently, he experienced recurrent pancreatitis due to an anastomotic stricture. Gastroscopy confirmed complete anastomotic occlusion, and the procedure was planned to reopen the occlusion and restore normal pancreatic duct function.
The stomach cavity was filled with water, and endoscopic ultrasound (EUS) was used to locate the pancreatic duct. The weakest part of the pancreatic-gastric anastomosis was identified, and cauterization marking was performed under EUS guidance to designate the starting point for the later dissection process using the endoscopic submucosal dissection (ESD) technique ( Fig. 1 ). A gastroscope with a transparent cap was then used to confirm the cauterization point. ESD was performed along the marked points, initially cutting through the mucosal layer and progressively dissecting the submucosal and muscle layers. During the dissection, blue surgical sutures were fortunately identified, confirming the location of the pancreatic-gastric anastomosis ( Fig. 2 ). A small incision was made adjacent to the sutures, allowing the pancreatic fluid to flow out ( Fig. 3 ). Since the pancreatic-gastric anastomosis was observed, the endoscopic retrograde cholangiao-pancreatography (ERCP) technique was applied to cannulate the body part of the pancreatic duct with a guide wire ( Fig. 4 ). The anastomosis was subsequently dilated with a dilating probe. Finally, a pancreatic duct stent was placed using a duodenoscope in combination with ERCP techniques ( Fig. 5 ). Pancreatic fluid drained smoothly into the stomach cavity, and the patient recovered well postoperatively.
EUS was used to locate the pancreatic duct. The cauterization marking was performed under EUS guidance. Abbreviation: EUS, endoscopic ultrasound.
A gastroscope was used to confirm the cauterization point. ESD was performed along the marked points, initially cutting through the mucosal layer and progressively dissecting the submucosal and muscle layer. Abbreviation: ESD, endoscopic submucosal dissection.
Pancreatic juice flowed into the stomach cavity.
The ERCP technique was applied to cannulate the pancreatic duct with a guide wire. Abbreviation: ERCP, endoscopic retrograde cholangiao-pancreatography.
The pancreatic duct stent was placed successfully.
In this case, the precise positioning of EUS, the channel creation of ESD, and the stent placement of ERCP are not merely a combination of techniques but rather a collaborative effort. Through careful planning and a seamless sequence of actions, they successfully resolved the issue of anastomotic stenosis following pancreaticogastrostomy, providing an ideal treatment approach for such diseases.
Endoscopy_UCTN_Code_TTT_1AO_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jagielski M Bella E Jackowski M Endoscopic pancreatogastric anastomosis in the treatment of symptoms associated with inflammatory diseases of the pancreas World J Gastrointest Endosc 20241640641210.4253/wjge.v 16.i 7.40639072251 PMC 11271716 · doi ↗ · pubmed ↗
- 2Sakai T Koshita S Kanno Y Early and long-term clinical outcomes of endoscopic interventions for benign pancreatic duct stricture/obstruction-the possibility of additional clinical effects of endoscopic ultrasonography-guided pancreatic drainage Pancreatology 202222586610.1016/j.pan.2021.10.00634742630 · doi ↗ · pubmed ↗
- 3Bhurwal A Tawadros A Mutneja HEUS guided pancreatic duct decompression in surgically altered anatomy or failed ERCP – A systematic review, meta-analysis and meta-regression Pancreatology 202121990100010.1016/j.pan.2021.03.02133865725 · doi ↗ · pubmed ↗
- 4Khan Z Hayat UEUS-guided pancreatic ductal intervention: A comprehensive literature review Endosc Ultrasound 2021109810210.4103/eus.eus_67_2033463554 PMC 8098848 · doi ↗ · pubmed ↗