Endoscopic ultrasound-guided hepaticogastrostomy using a 22G needle with a 0.018-inch ultra-stiff guidewire without tract dilation
Takeshi Ogura, Jun Matsuno, Takafumi Kanadani, Ahmad F. Aboelezz, Hiroki Nishikawa

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1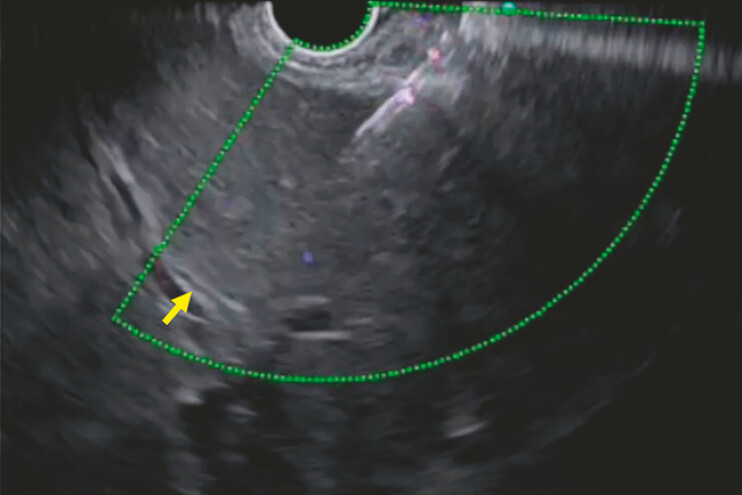 Fig. 2
Fig. 2 Fig. 3
Fig. 3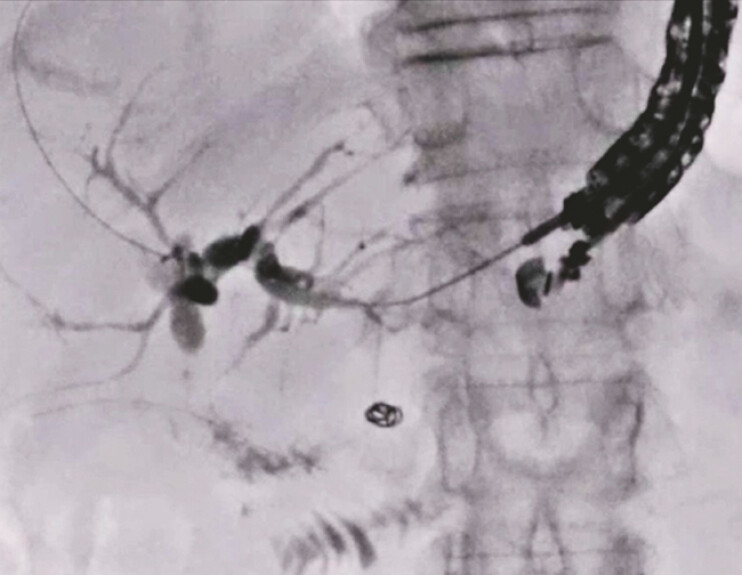 Fig. 4
Fig. 4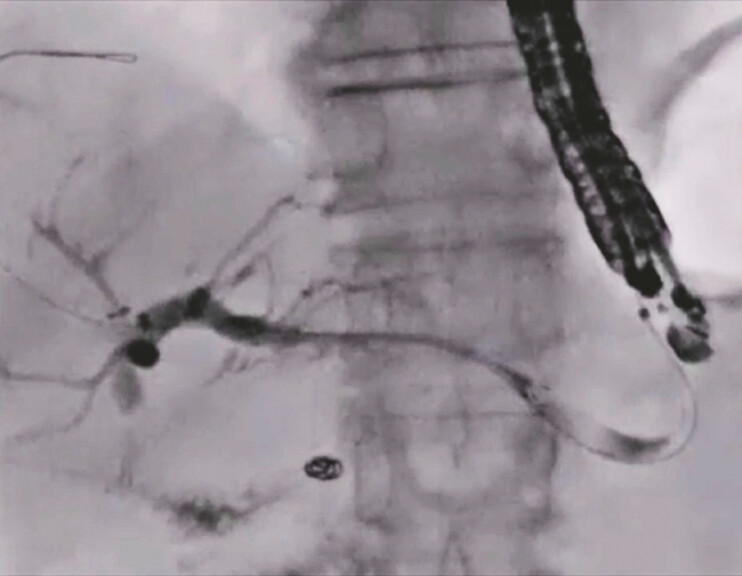 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Gallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments
Endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) is indicated for the treatment of malignant biliary strictures in cases where attempts at biliary drainage under endoscopic retrograde cholangiopancreatography have failed. Recently, EUS-HGS is also increasingly being performed for benign biliary diseases, such as common bile duct or hepaticojejunostomy strictures 1 2 3 . However, since strictures cause greater narrowing of the intrahepatic bile duct than malignant biliary disease does, puncturing a stricture using a 19G needle is sometimes challenging. In such cases, using a 22G needle may enable successful puncture of the biliary tract – but there may still be a problem, because a 22G needle would require insertion of a 0.018-inch guidewire, the stiffness of which is less than that of the 0.025-inch guidewire. This could result in a longer procedure time, because the 0.018-inch guidewire needs to be exchanged for a 0.025-inch guidewire for the insertion of various devices.
Recently, a novel 0.018-inch ultra-stiff guidewire (J-Wire Premier NM, J-MIT, Shiga, Japan) has become available in Japan ( Fig. 1 ). This guidewire is made of a titanium, nickel, and cobalt alloy, and the sheath material is coated with polytetrafluoroethylene. The enhanced stiffness of this guidewire allows device insertion without the need to exchange the guidewire. Herein, we describe EUS-HGS using this guidewire.
A novel 0.018-inch ultra-stiff guidewire made of a titanium, nickel, and cobalt alloy, with a sheath material coated with polytetrafluoroethylene.
A 59-year-old man, who had undergone pancreaticoduodenectomy because of pancreatic head cancer 3 years earlier, was admitted to our hospital due to complications of hepaticojejunostomy stricture and obstructive jaundice. EUS-HGS was attempted. Since the diameter of the intrahepatic bile duct was 1 mm on EUS imaging ( Fig. 2 ), a 22G needle was selected. Contrast medium was injected after successful bile duct puncture using the 22G needle ( Fig. 3 ), and the novel 0.018-inch guidewire was inserted and successfully deployed ( Fig. 4 ). Finally, a partially covered self-expandable metal stent delivery system was successfully inserted into the biliary tract without tract dilation, and was deployed from the intrahepatic bile duct to the stomach without any adverse events ( Fig. 5 ) ( Video 1 ).
The diameter of the intrahepatic bile duct is 1 mm on EUS imaging.
Contrast medium is injected after successful bile duct puncture using the 22G needle.
The novel 0.018-inch guidewire is inserted, followed by successful deployment.
A partially covered self-expandable metal stent delivery system is successfully inserted into the biliary tract without tract dilation, and is deployed from the intrahepatic bile duct to the stomach.
The novel 0.018-inch guidewire is inserted and successfully deployed in an intrahepatic bile duct with an intraluminal diameter of 1 mm.Video 1
In conclusion, the new 0.018-inch ultra-stiff guidewire may be useful in cases in which a 22G needle is used for biliary puncture during EUS-HGS, as it may eliminate the need to change to a 0.025-inch guidewire.
Endoscopy_UCTN_Code_TTT_1AS_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Caillol F Godat S Solovyev AEUS-BD for calibration of benign stenosis of the bile duct in patients with altered anatomy or inaccessible papilla Endosc Int Open 202412 E 377E 38410.1055/a-2261-296838464978 PMC 10919993 · doi ↗ · pubmed ↗
- 2Matsunami Y Itoi T Sofuni AEUS-guided hepaticoenterostomy with using a dedicated plastic stent for the benign pancreaticobiliary diseases: a single-center study of a large case series Endosc Ultrasound 20211029430434259218 10.4103/EUS-D-20-00232 PMC 8411555 · doi ↗ · pubmed ↗
- 3Ogura T Nishioka N Yamada M Novel transluminal treatment protocol for hepaticojejunostomy stricture using covered self-expandable metal stent Surg Endosc 20213520921510.1007/s 00464-020-07381-231932928 · doi ↗ · pubmed ↗