Full-thickness closure using reopenable clip-over-the-line method for a large defect after duodenal full-thickness resection
Tatsuma Nomura, Morihito Setsuda, Shinichiro Nakamura, Takashi Hamada, Hiroshi Kaneko, Katsumi Mukai

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
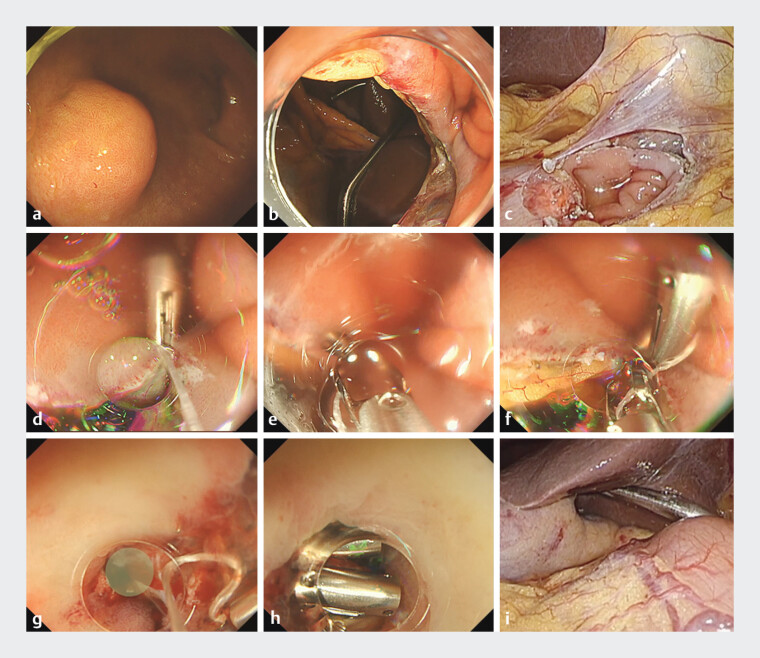 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Esophageal and GI Pathology · Gallbladder and Bile Duct Disorders
Laparoscopic-assisted full-thickness resection of duodenal gastrointestinal stromal tumors (GISTs) is a safe and reliable procedure 1 . However, due to the narrow lumen of the duodenum, there exists a possibility that the mucosal closure on the gastrointestinal side could be insufficient 2 . We have previously described the feasibility of the reopenable clip-over-the-line method (ROLM), which can be used to close large mucosal defects even in narrow lumens 3 4 . In this report, we present a case of full-thickness defect closure of the anterior wall of the duodenal bulb using the ROLM.
A male patient in his 60s was diagnosed with a GIST by biopsy of the anterior wall of the duodenal bulb ( Fig. 1 , Video 1 ). We completely resected the GIST laparoscopically. The bulb defect was approximately 25 mm in size. We used the ROLM to close the defect. First, a clip with a line was placed to grasp the edge of the defect on the anal side, including the serous muscle layer. A reopenable clip with a line threaded through one of the teeth placed on the contralateral edge to grasp the mucosa and fat tissue. Even in a narrow lumen, such as the duodenum, the use of a tapered tip hood made it possible to repeatedly place the reopenable-clips without existing clips obstructing the view 5 . Laparoscopic observation confirmed that the defect was completely closed, except for the defect near the pyloric ring, and the serous muscle layer was surgically sutured. The pyloric stenosis was confirmed to be free from narrowing under endoscopic visualization, and the remaining full-thickness defect was completely closed. The patient was discharged from the hospital 7 days postoperatively without any adverse events. Five weeks later, endoscopy confirmed that the clips were still in place and that there was no gastrointestinal stenosis.
Endoscopy_UCTN_Code_TTT_1AO_2AZ
Closure of a large full-thickness defect in the duodenum using the reopenable clip-over-the-line method (ROLM). a A 13-mm gastrointestinal stromal tumor (GIST) in the anterior wall of the duodenal bulb. b Full-thickness defect of the anterior duodenal bulb up to the pyloric ring, approximately 25 mm in size, after full-thickness resection of the SMT. c Full-thickness defect of the duodenum observed via laparoscopy. d The first clip with a line is placed on the anal side of the duodenum. e A clip with a line threaded through a tooth is placed on the opposite side to grasp the mucosa and serous muscle layers. f If fat tissue is identified, the clip is placed by grasping the fat in addition to the mucosa and serous muscle layers. g A small full-thickness defect (green area) is identified near the pyloric ring after surgical serous suturing. h After confirming the absence of stenosis of the pyloric ring under endoscopic visualization, the remaining full-thickness defect is completely closed. i After observing the duodenum in the abdominal cavity, the absence of gas leakage due to insufflation through the endoscope is confirmed. Abbreviations: GIST gastrointestinal stromal tumors; ROLM, reopenable clip-over-the-line method.
Closure of a large full-thickness defect in the duodenum using the reopenable clip-over-the-line method.Video 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nunobe S Ri M Yamazaki K Safety and feasibility of laparoscopic and endoscopic cooperative surgery for duodenal neoplasm: a retrospective multicenter study Endoscopy 2021531065106810.1055/a-1327-593933264810 · doi ↗ · pubmed ↗
- 2Xu P Liu Z Wang L Free-hand endoscopic full-thickness resection for duodenal subepithelial lesions J Gastroenterol Hepatol 202510.1111/jgh.1687839844340 · doi ↗ · pubmed ↗
- 3Nomura T Sugimoto S Temma T Reopenable clip-over-the-line method for closing large mucosal defects following gastric endoscopic submucosal dissection: Prospective feasibility study Dig Endosc 20233550551110.1111/den.1446636346166 · doi ↗ · pubmed ↗
- 4Nomura T Sugimoto S Oyamada J Application of a new loop cutter for nylon lines and the reopenable clip-over-line method for large defect closure after duodenal endoscopic submucosal dissection Endoscopy 202355 E 503E 50410.1055/a-2032-369736894140 PMC 9998226 · doi ↗ · pubmed ↗
- 5Nomura T Sugimoto S Fujimura Y Full-thickness defect closure using the reopenable clip over-the-line method with omental patch Endoscopy 202355 E 969E 97037604446 10.1055/a-2133-6266 PMC 10442211 · doi ↗ · pubmed ↗