Diagnostic Power of Head-Up Tilt Test Enhanced by Autonomic ECG Parameters and Beat-to-Beat Hemodynamic Monitoring
Mathias Klemm, Antonia Kellnar, Dominik Naumann, Stefan Brunner, Christopher Stremmel

TL;DR
This study shows that adding advanced ECG and blood pressure monitoring to a tilt test improves the ability to diagnose syncope.
Contribution
The study introduces autonomic ECG parameters and continuous hemodynamic monitoring to enhance the diagnostic accuracy of the head-up tilt test.
Findings
The extended protocol detects more pronounced hemodynamic fluctuations and enables real-time trend analysis.
Patients with syncope showed significantly higher PRD values during the tilt phase (8.14 vs. 3.91 deg², p=0.043).
Continuous monitoring allows earlier recognition of impending syncope and better identification of its cause.
Abstract
Objectives: The head-up tilt test (HUTT) is a well-established diagnostic procedure used to differentiate between the types of syncope. Since its introduction in 1986, the protocol has undergone several refinements aimed at increasing diagnostic accuracy. Despite growing interest in advanced autonomic ECG parameters and beat-to-beat blood pressure monitoring, their integration into routine HUTT protocols remains limited. Methods: In this study, we compared the conventional HUTT protocol using two-minute interval monitoring with an advanced protocol incorporating autonomic ECG parameters—periodic repolarization dynamics (PRD) and deceleration capacity (DC)—as well as continuous beat-to-beat hemodynamic monitoring. Results: The extended protocol improves diagnostic resolution by detecting more pronounced hemodynamic fluctuations, enabling real-time trend analysis, and allowing earlier…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
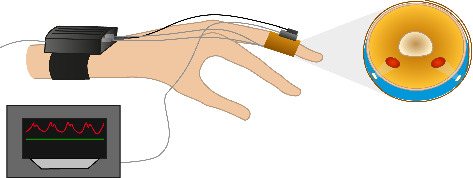 Figure 1
Figure 1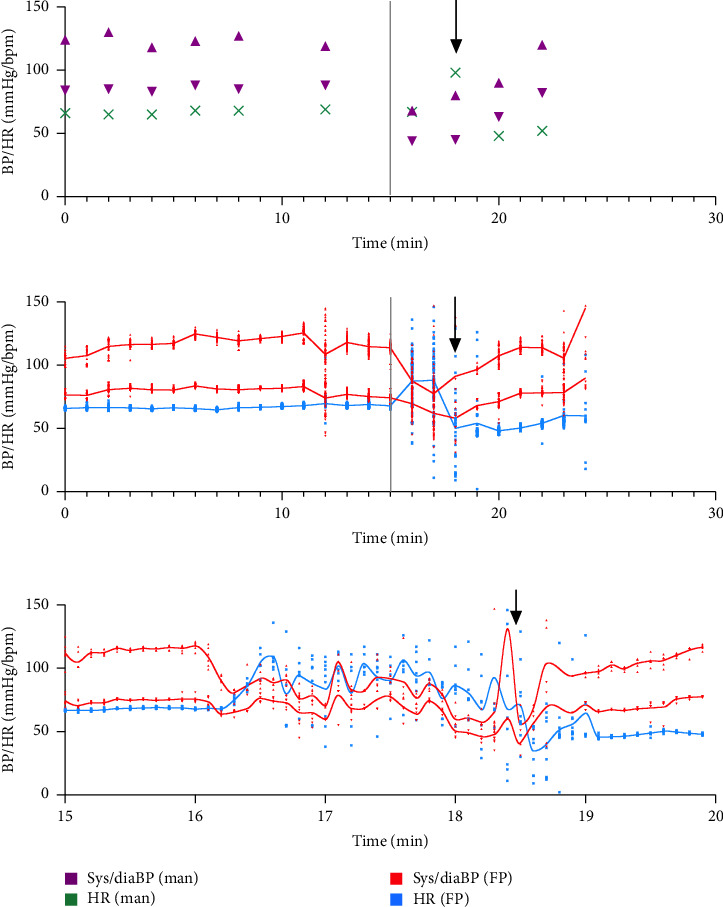 Figure 2
Figure 2- —Projekt DEAL
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Syncope and Autonomic Disorders · Heart Rate Variability and Autonomic Control · Non-Invasive Vital Sign Monitoring
1. Introduction
Syncope is defined as a transient loss of consciousness due to transient global cerebral hypoperfusion. Although a sudden drop in systemic blood pressure (BP) is commonly the immediate trigger, identifying the underlying pathophysiological mechanism remains challenging. The head-up tilt test (HUTT) is routinely employed to detect various forms of autonomic dysregulation in patients with recurrent syncope or presyncope [1, 2]. In its original publication in 1986, Kenny and coworkers exposed the patient to a 40° tilt for 60 min to provoke vasovagal syncope [3, 4]. In the following years, this original protocol was modified to enhance sensitivity and reduce duration. According to the 2018 ESC guidelines and the 2017 ACC/AHA/HRS guidelines on syncope, HUTT is recommended with a Class IIa level B indication for evaluating suspected reflex syncope, orthostatic hypotension, and psychogenic pseudosyncope [1, 2].
Despite its widespread use, diagnostic limitations persist. We hypothesized that the integration of high-resolution ECG-derived autonomic markers—namely, periodic repolarization dynamics (PRD) and deceleration capacity (DC)—could optimize HUTT performance and facilitate pathophysiological understanding in patients with unexplained syncope. PRD quantifies low-frequency sympathetic modulation of ventricular repolarization, while DC reflects parasympathetic influence via analysis of RR-interval dynamics [5–8]. In addition, beat-to-beat BP monitoring, as suggested by the current ESC and ACC/AHA/HRS guidelines (Class IIb), can capture rapid hemodynamic changes often missed by interval measurements, potentially increasing the diagnostic yield [1, 2]. Therefore, we included continuous noninvasive BP monitoring and the abovementioned ECG parameters in our advanced testing protocol to evaluate their optimization potential during HUTT.
2. Methods
2.1. Patients
In this prospective pilot study, we aimed to optimize the standard-of-care HUTT protocol by incorporating continuous recording of autonomic ECG parameters and beat-to-beat BP monitoring. We enrolled 22 patients with suspected autonomic syncope between March 2019 and November 2023. In accordance with the Declaration of Helsinki and German data protection laws, all patients in this analysis provided informed consent, and the study was approved by the local ethics committee (approval code: 370-16, LMU Munich, Germany).
2.2. Study Definition and Endpoints
Orthostatic syncope is defined as a progressive fall of 20 mmHg or more in systolic BP, or 10 mmHg or more in diastolic BP after a few minutes of standing or a 60° tilt. Syncope occurring within 3 min is commonly defined as classic orthostatic hypotension, and syncope occurring after more than 3 min is defined as delayed orthostatic hypotension [1]. Reflex syncope is characterized by a rapid decrease in both BP and heart rate, usually triggered externally by pain, emotion, or orthostatic stress, and often begins with prodromal symptoms such as a feeling of warmth, abdominal discomfort, or nausea. According to the Vasovagal International Study classification, there are three main forms: Type 1 is a mixed form with a significant drop in BP followed by a decrease in heart rate; Type 2, the cardioinhibitory form, is characterized by a predominant drop in heart rate to less than 40 beats per minute (bpm) for at least 10 s, or asystole for more than 3 s; Type 3, the vasodepressor form, features a predominant drop in BP while the heart rate remains stable [9]. Classification into these types of syncope was performed by five independent cardiologists. In cases of disagreement, the final classification was determined by a majority vote.
2.3. Data Collection
Baseline data were collected as part of the routine diagnostic and treatment protocol, and the indication for HUTT was independent of this study. During HUTT, we performed automated interval BP monitoring every two minutes and continuous ECG recording (Philips IntelliVue X2) for a total of 60 min according to the standard of care protocol: After 15 min, patients were transferred to a 60° tilt for up to 45 min. If syncope did not occur spontaneously, 0.4 mg of sublingual glyceryl trinitrate was administered. The test was terminated at the onset of (pre)syncope or after 60 min. In parallel, but not as an indicator of test termination, noninvasive continuous BP monitoring (Finapres, Nova, the Netherlands) and high-resolution ECG signals (TMSi Porti, the Netherlands) were recorded for retrospective evaluation of the potential for test optimization.
The ECG signals were recorded at 2000 Hz using Frank leads. The DC and PRD were calculated from these signals for the baseline (horizontal position) and tilt phase of HUTT using our proprietary SMARTlab software (Version 1.5.4). In addition, to increase temporal resolution, we calculated short-term DC and PRD from one-minute ECG segments using a sliding window.
DC is a measure of heart rate variability. It is calculated from RR-intervals using phase-rectified signal averaging to isolate vagal modulations of the heart rate. PRD is a measure of sympathetic influence at the myocardial level. It analyzes the beat-to-beat variability of the T-wave repolarization vector and quantifies periodic sympathetic modulations at frequencies below 0.1 Hz.
2.4. Statistical Analysis
Statistical analysis was performed using R 4.3.1 and Prism 9 (GraphPad, USA) software. Continuous variables were reported as median and interquartile range (IQR). The Wilcoxon rank sum test was used to compare groups, with p values < 0.05 considered statistically significant.
3. Results
3.1. Baseline Characteristics
Twenty-two patients with a history of syncope and an indication for HUTT were enrolled in this study. Ten patients (45.5%) were female with a median age of 52 years and a BMI of 23.9 kg/m^2^. Left ventricular ejection fraction was normal in all patients, among them, one of whom had hypertrophic cardiomyopathy. Coronary artery disease was present in three of 22 patients (13.6%). The baseline BP was 123/75 mmHg with a heart rate of 78 bpm. Regarding preexisting cardiac arrhythmias, three patients had atrial fibrillation, and one patient had a history of cardiac arrest. The reported conduction disorders were left bundle branch block in one patient and 1st degree atrioventricular block in another (Table 1).
3.2. Beat-to-Beat Monitoring Improves HUTT Resolution
In addition to the conventional HUTT protocol, we performed continuous noninvasive hemodynamic monitoring using the Finapres NOVA device (Finapres Medical Systems, the Netherlands; Figure 1) to evaluate its potential advantages over standard interval BP measurements. Compared to standard interval BP recordings, beat-to-beat monitoring revealed a broader spectrum of systolic and diastolic values, allowing for earlier and more precise detection of hemodynamics. Systolic peaks were higher and nadirs lower, confirming the added sensitivity of continuous monitoring (Table 2).
3.3. Syncope Classification
The median duration of HUTT was 53 min. The primary endpoint, consisting of presyncope and syncope, was observed in two (9.1%) and ten (45.5%) patients, respectively, after a median study duration of 41 min. Five independent cardiologists classified the cause of syncope as reflex syncope Type 1 (mixed type) in three cases (13.6%), reflex syncope Type 2 (cardioinhibitory type) in five cases (22.7%), reflex syncope Type 3 (vasodepressor type) in two cases (9.1%), and as orthostatic syncope in two cases (9.1%) (Table 3).
3.4. Continuous BP Assessment Improves HUTT Quality
The recordings of the syncopal event itself also showed lower nadirs in continuous versus interval measurements (Tables 3 and 4). When comparing the cohorts based on the study endpoint, patients with syncope had significantly lower systolic BP and heart rate at the time point of syncope in both interval and continuous recordings (Table 4). Graphical data presentation was used to illustrate our findings (Figure 2).
3.5. Syncope and Autonomic ECG Parameters
To further strengthen our HUTT setup, we also evaluated Frank leads recordings to assess ECG parameters reflecting autonomic function, namely, PRD and DC. These parameters have been evaluated for cardiac risk prediction and are considered useful tools for studying events related to the autonomic nervous system [5–8]. Only 18 of 22 patients in our study population could be analyzed for autonomic ECG parameters due to insufficient quality and a corrupted data file. Two of the excluded patients had syncope.
The median baseline PRD value in our study cohort was 4.14 (2.07; 7.02) deg^2^. PRD was numerically higher during the tilt phase at 5.82 (3.66; 8.30) deg^2^ (p=0.182), with a significant increase in PRD during the first minutes of the tilt phase independent of syncope events (p=0.015 for Minute 1, p=0.002 for Minute 2, and p=0.004 for Minute 3). PRD during the entire tilt phase was significantly higher in patients with syncope (8.14 (6.36; 10.60) deg^2^) compared to patients without syncope (3.91 (3.64; 4.63) deg^2^, p=0.043) (Table 5).
The median baseline DC was 5.63 (3.56; 7.77) ms. There was a numerical trend toward lower DC values during the tilt phase, with a median of 4.58 (1.58; 7.56) ms (p=0.212) for the entire cohort (Table 5). Patients with (pre)syncope showed a nonsignificant increase in PRD (ΔPRD with syncope: +0.77 vs. ΔPRD without syncope: +0.08; p=0.360) as well as a decrease in DC in the tilt position (ΔDC with syncope: −1.73 vs. ΔDC without syncope: +0.30; p=0.068), independent of the type of syncope.
4. Discussion
In this study, we demonstrate the added potential of an advanced noninvasive monitoring system during HUTT. Continuous BP monitoring allows for earlier detection of impending syncope and increases the awareness of the attending physician immediately prior to the event. In addition, BP and heart rate values are more accurate due to very short recording intervals (i.e., more than one data point per second) and repetitive measurements. While the interval method carries the risk of potentially missing the most extreme measurements, this problem can be overcome by continuous recording. In addition, the classification of syncope types becomes much easier compared to the classical interval method. Especially in the very low BP range around the time of syncope, automated interval BP measurements may fail and important information is irretrievably lost. Even when compared to intrabrachial invasive BP measurements, Finapres measurements provided reliable results [10].
In the future, it may be possible to identify clear cutoffs for rapid BP changes sufficient to make a reliable diagnosis while avoiding the unpleasant event of complete loss of consciousness. Similarly, a study by Pitzalis et al. identified the first 15 min of tilt as having the highest predictive potential, which could be further enhanced by continuous recording [11]. The clear advantage of beat-to-beat BP monitoring is also reflected by ESC and ACC/AHA/HRS guideline recommendations, and we strongly suggest a further increase in the use of this technology worldwide.
It is important to note at this point that the concept of autonomic cardiac function analysis via ECG parameters has been present in the literature for several years. Even if the parameters PRD and DC analyzed here were not the focus at that time, the general concept has already proven to be very promising in HUTT and is further confirmed by our work [12–16]. For example, prior studies by Porta and colleagues highlighted the relevance of combined ventricular repolarization duration and heart period correlations for assessing autonomic function [13, 14].
PRD (sympathetic nervous system) and DC (parasympathetic nervous system) baseline values did not correlate with the occurrence of syncope. In general, our population had PRD and DC values considered physiological in previous studies [5, 6]. However, patients with syncope showed significantly higher PRD values in the tilt position, indicating the presence of autonomic dysregulation prior to syncope. All patients showed a significant increase in PRD during the first minutes of tilt, with no significant difference in PRD for the entire tilt phase. This suggests that patients who experience syncope during the tilt test exhibit more sustained sympathetic dysregulation than those without. Our study thus contributes novel insights by demonstrating the feasibility and clinical utility of integrating these parameters with noninvasive beat-to-beat BP monitoring.
Additionally, our methodology enables estimation of baroreflex sensitivity (BRS) through spontaneous fluctuations in RR-intervals and BP, as described in previous studies [17, 18]. While BRS was not a focus of this pilot study, we acknowledge its potential as a valuable metric in future research aimed at refining syncope diagnostics. Furthermore, characterizing HUTT responses could benefit from incorporating respiratory-related autonomic markers. Cardiorespiratory coupling, such as respiratory sinus arrhythmia or spectral components of RR-variability at the respiratory frequency, offers an additional window into vagal function. Although our setup did not include respiratory signal acquisition, future studies should consider integrating such measures to provide a more comprehensive assessment of autonomic cardiovascular regulation [19].
Our study is clearly limited by its sample size. However, it was designed as a pilot study to evaluate the feasibility of evaluating autonomic ECG parameters during HUTT. The current methods for calculating PRD and DC have been validated for measurements of at least 20 min. Therefore, some of the standing ECG recordings of patients with syncope are shorter than the usual recordings used. The error caused by artifacts, i.e., caused by movement, is greater in these measurements. Overall, the data quality in our study cohorts was good and promising for further evaluation in larger studies including these short-frame recordings.
5. Conclusions
The integration of autonomic ECG markers with beat-to-beat BP monitoring during HUTT is feasible, cost-effective, and diagnostically beneficial. Our findings support the inclusion of PRD and DC into clinical HUTT protocols and highlight future opportunities for autonomic profiling through BRS and respiratory-linked metrics. Larger, multicenter studies are warranted to validate these results and define clear diagnostic thresholds.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brignole M. Moya A. de Lange F. J. 2018 ESC Guidelines for the Diagnosis and Management of Syncope European Heart Journal 2018 June 39211883194810.1093/eurheartj/ehy 0372-s 2.0-8504806850129562304 · doi ↗ · pubmed ↗
- 2Shen W. K. Sheldon R. S. Benditt D. G. 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society Circulation 2017 August 1365 e 25e 5910.1161/CIR.00000000000004982-s 2.0-8501475315728280232 · doi ↗ · pubmed ↗
- 3Benditt D. G. Sutton R. Tilt-Table Testing in the Evaluation of Syncope Journal of Cardiovascular Electrophysiology 2005 March 16335635810.1046/j.1540-8167.2005.40768.x 2-s 2.0-1554437252415817101 · doi ↗ · pubmed ↗
- 4Kenny R. A. Ingram A. Bayliss J. Sutton R. Head-Up Tilt: A Useful Test for Investigating Unexplained Syncope Lancet 1986 June 184941352135510.1016/s 0140-6736(86)91665-x 2-s 2.0-849202125512872472 · doi ↗ · pubmed ↗
- 5Rizas K. D. Hamm W. Kaab S. Schmidt G. Bauer A. Periodic Repolarisation Dynamics: A Natural Probe of the Ventricular Response to Sympathetic Activation Arrhythmia & Electrophysiology Review 2016 May 51313610.15420/aer.2015:30:22-s 2.0-8504504495027403291 PMC 4939306 · doi ↗ · pubmed ↗
- 6Rizas K. D. Mc Nitt S. Hamm W. Prediction of Sudden and Non-Sudden Cardiac Death in Post-Infarction Patients With Reduced Left Ventricular Ejection Fraction by Periodic Repolarization Dynamics: MADIT-II Substudy European Heart Journal 2017 July 38272110211810.1093/eurheartj/ehx 1612-s 2.0-8502971677928431133 PMC 5837472 · doi ↗ · pubmed ↗
- 7Shusterman V. Swenne C. A. Hoffman S. Strollo P. J. London B. Tracking Autonomic Nervous System Activity Using Surface ECG: Personalized, Multiparametric Evaluation Journal of Electrocardiology 2025 January 88p. 15383710.1016/j.jelectrocard.2024.153837 PMC 1171760339615267 · doi ↗ · pubmed ↗
- 8Dash R. R. Samanta P. Das S. Heart Rate Variability in Unexplained Syncope Patients Versus Healthy Controls: A Comparative Study Cureus 2023 July 157p. e 4137010.7759/cureus.41370 PMC 1039996737546077 · doi ↗ · pubmed ↗