Pulmonary talcosis due to aspiration
Edson Marchiori, Bruno Hochhegger, Gláucia Zanetti

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
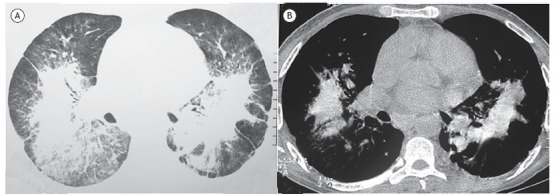 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSympathectomy and Hyperhidrosis Treatments · Restraint-Related Deaths · Tattoo and Body Piercing Complications
A 41-year-old man with dry cough and progressive dyspnea on moderate/high exertion was admitted to our service. He worked for 8 years in a cosmetics industry. A chest CT scan showed bilateral conglomerate masses (Figure 1). Tomographic findings associated with the occupational history allowed the diagnosis of pulmonary talcosis.
Figure 1CT scans of the lower lobes with lung window setting (in A) showing bilateral conglomerate masses, ground-glass opacities, areas of emphysema, and dense streaks in the periphery. In B (mediastinal window setting), areas of increased attenuation within the conglomerate masses are revealed, compatible with talc deposition.
Conglomerate masses can occur in four basic pulmonary conditions: silicosis, coal workers’ pneumoconiosis, sarcoidosis, and talcosis. Although the identification of conglomerate masses on chest CT restricts the diagnostic possibilities to these four diseases, clinical and occupational history, both current and past, is essential for final diagnosis.
Talcosis is an uncommon pneumoconiosis, related to the aspiration or injection of talc (magnesium silicate). Patients may be asymptomatic or present with a severe disease course. Symptomatic patients usually present with nonspecific complaints, including progressive dyspnea on exertion and cough.
Late complications include chronic respiratory failure, emphysema, pulmonary arterial hypertension, and cor pulmonale. Two distinct forms of lung disease caused by talc have been defined. One is associated with aspiration of the product, and one results from intravenous administration of talc, seen in drug users. Talc is a mineral widely used in various industries. Inhalation of a large amount of talc can occur during its extraction from mines, separation, milling, packaging, loading, and transportation. There have also been reports of talcosis in workers exposed to talcum powder in secondary industries such as rubber, paper, textiles, leather, ceramics, pharmaceuticals, cosmetics, insecticides, and herbicide manufacturers, as well as in soapstone workers. In addition to the possible occupational history, the possibility of the patient being a drug addict should be carefully evaluated, especially those who intravenously inject oral substances.
On CT, findings of small centrilobular nodules associated with heterogeneous conglomerate masses containing amorphous areas of high attenuation within them, determined by talc deposition, with or without panlobular emphysema in the lower lobes, are highly suggestive of pulmonary talcosis. On CT, the main difference between inhaled and intravenous forms is the possibility of emphysema developing in the latter. The histopathological feature of talc pneumoconiosis is the presence of birefringent, needle-shaped talc particles seen within giant cells and in areas of pulmonary fibrosis using polarized light.
Our patient also underwent BAL, which showed birefringent particles, confirming the diagnosis of pulmonary talcosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Marchiori E Souza ASJúnior Müller NL Inhalational pulmonary talcosis high-resolution CT findings in 3 patients J Thorac Imaging 2004191414410.1097/00005382-200401000-0000814712131 · doi ↗ · pubmed ↗
- 2Marchiori E Lourenço S Gasparetto TD Zanetti G Mano CM Nobre LF Pulmonary talcosis imaging findings Lung 2010188216517110.1007/s 00408-010-9230-y 20155272 · doi ↗ · pubmed ↗
- 3Gonçalves TA Barreto MM Marchiori E Pulmonary talcosis related to cocaine inhalation J Bras Pneumol 2021473 e 2021014610.36416/1806-3756/e 2021014634190865 PMC 8332722 · doi ↗ · pubmed ↗
- 4Marchiori E Hochhegger B Zanetti G Conglomerate masses J Bras Pneumol 201642423923910.1590/S 1806-3756201600000016127832228 PMC 5063437 · doi ↗ · pubmed ↗